



MRI findings and postoperative follow-up of perianorectal intramuscular infection
-
摘要:
目的 分析肛管直肠周围肌组织脓肿长期被临床忽视的原因,并总结术后患者肛门功能的恢复情况。 方法 回顾性分析39例肛门外括约肌和/或耻骨直肠肌、肛提肌脓肿患者的MRI表现,并随访术后患者控便及排便能力。 结果 18例为单一肌组织脓肿,21例并发两组以上肌组织脓肿,其中存在肛门外括约肌深部脓肿28例,浅部脓肿26例,耻骨直肠肌脓肿9例,肛提肌脓肿4例,肛门外括约肌皮下部脓肿1例;感染肌组织肿胀增粗,基本保持解剖形态,其中外括约肌深部呈典型“U”形,肛提肌呈对称“蝴蝶翅膀样”表现;肛周脂肪间隙清晰34例,脂肪间隙结构不清5例,术中触及内口26例。35例未累及肛提肌患者术后控便和排便良好,3例肛提肌脓肿患者存在不同程度控便不良及排便无力,另1例失联。 结论 肛门外括约肌和/或耻骨直肠肌、肛提肌有时不能阻挡肛周感染的传播,甚至肌组织内部形成脓肿,肛门外括约肌及耻骨直肠肌脓肿术后患者肛门控便及排便功能很可能不受影响,肛提肌脓肿术后患者可能会出现肛门控便及排便功能不同程度降低。 Abstract:Objective To analyze the causes of long-term clinical neglect of perianorectal muscle tissue abscess, and summarize the recovery of anal function in patients after operation. Methods The MRI features of 39 patients with abscess of external anal sphincter and/or puborectalis muscle and levator ani muscle were analyzed retrospectively. The anal defecation control and defecation ability were followed up. Results There were 18 cases of single muscle tissue abscess and 21 cases of complicated with more than two groups of muscle tissue abscess. There were 28 cases of deep abscess of external anal sphincter, 26 cases of superficial abscess, 9 cases of puborectal abscess, 4 cases of levator ani abscess and 1 case of subcutaneous abscess of external anal sphincter. The infected muscle tissue swelled and thickened, basically maintaining the anatomical shape. The deep part of the external sphincter showed a typical "U" shape, and the levator ani muscle showed a symmetrical "butterfly wing" appearance. 34 cases had clear perianal fat space, 5 cases had unclear fat space and 26 cases had internal openings. 35 patients without involvement of levator ani muscle recovered well after operation. Three patients with abscess of levator ani muscle had different poor ability of fecal control and defecation after operation, and other patients with levator ani muscle abscess lost contact. Conclusion The external anal sphincter, puborectal muscle and levator ani muscle sometimes can not stop the spread of perianal infection, and even form an abscess inside the muscle tissue. The patients with external anal sphincter and puborectal muscle abscess have normal ability of fecal control and defecation after operation. Patients with levator ani abscess may have decreased ability of fecal control and defecation after operation. -
Key words:
- intramuscular infection /
- perianorectal /
- MRI
-

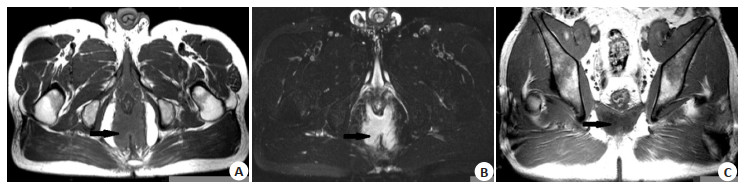
图 1 男性,16岁,双侧肛门外括约肌浅部和深部脓肿
A~B:分别为斜轴位T1WI、T2WI,双侧肛门外括约肌深部明显增粗(黑长箭),呈“U”形,其内充满脓液,T1WI呈等、低信号,T2WI呈高信号; C:斜冠状位T1WI,双侧肛门外括约肌深部及浅部均增粗(黑长箭),并可见括约肌间隙高信号脂肪(黑短箭).
Figure 1. A 16-year-old male patient, bilateral deep and superficial abscess of external anal sphincter.

图 2 男性,43岁,双侧肛提肌脓肿
A~B:分别为斜轴位T1WI、抑脂T2WI,双侧肛提肌对称性增粗(黑长箭),其内充满脓液,T1WI呈低信号,T2WI呈高信号,呈“蝴蝶样”改变; C:斜冠状位T1WI,双侧肛提肌增粗(黑长箭).
Figure 2. A 43-year-old male patient, bilateral levator ani abscess.
表 1 肛管直肠周围肌组织脓肿MRI扫描参数
Table 1. MRI scanning parameters of perianorectal muscle tissue abscess
序列 断面 TR(ms) TE (ms) 层厚(mm) 矩阵 视野 激励次数 脂肪饱和 FSE T2WI 矢状面 2900 100 3 320x224 26x23 4 加 FSE T2WI 斜冠状面 2800 89 3 384x256 26x26 4 加 FSE T1WI 斜冠状面 400 8 3 384x224 26x26 4 FSE T2WI 斜轴面 3250 120 3 384x224 28x28 4 加 FSE T1WI 斜轴面 450 8 3 384x224 28x28 4 FSE T2WI 斜轴面 3070 120 3 384x224 28x28 4 扩散加权成像(b=1000 s/mm2) 斜轴面 5000 66 3 96x130 34x34 8  下载: 导出CSV
下载: 导出CSV
表 2 肛管直肠周围肌组织脓肿感染部位统计及愈后情况
Table 2. Statistics of infection sites and healing of perianorectal muscle tissue abscess (n)
感染部位 例数 感染肌组织数目 随访 深部+浅部 11 22 愈后良好 深部 8 8 愈后良好 浅部 8 8 愈后良好 耻骨直肠肌+深部+浅部 6 18 愈后良好 肛提肌 2 2 1例2年后腹壁造瘘,例失联 肛提肌+耻骨直肠肌+深部 1 3 1年后愈后良好 肛提肌+耻骨直肠肌 1 2 控便及排便欠佳 耻骨直肠肌+深部 1 2 愈后良好 深部+浅部+皮下部 1 3 愈后良好 深部、浅部、皮下部分别指肛门外括约肌深部、浅部、皮下部.
下载: 导出CSV
-
[1] 张东铭. 盆底肛直肠外科理论与临床[M]. 2版. 北京: 人民军医出版社, 2011: 103-104. [2] Shafik A. A new concept of the anatomy of the anal sphincter mechanism and the physiology of defecation[J]. Am J Surg, 1986, 151(2): 278-84. doi: 10.1016/0002-9610(86)90087-5 [3] Pfenninger JL, Zainea GG. Common anorectal conditions[J]. Obstet Gynecol, 2001, 98(6): 1130-9. [4] Parés D. Pathogenesis and treatment of fistula in ano[J]. Br J Surg, 2010, 98(1): 2-3. doi: 10.1002/bjs.7341 [5] 朱杏莉, 郭茂林, 张伯英, 等. 直肠肛管周围肌组织感染的MRI诊断[J]. 临床放射学杂志, 2016, 35(9): 1395-7. https://www.cnki.com.cn/Article/CJFDTOTAL-LCFS201609029.htm [6] 程静, 赵云超, 张衡, 等. 磁共振成像检查对肛提肌脓肿的定位诊断及价值[J]. 实用医学影像杂志, 2018, 19(3): 221-4. https://www.cnki.com.cn/Article/CJFDTOTAL-SYXY201803018.htm [7] 陈孝平, 汪建平. 外科学[M]. 8版. 北京: 人民卫生出版社, 2013: 415. [8] 傅传刚, 陆建平, 李卫萍, 等. 盆底与肛管直肠疾病影像学图谱[M]. 北京: 人民军医出版社, 2010: 68. [9] 沈志军. 肛周脓肿MRI扫描的临床应用[J]. 影像研究与医学应用, 2019, 3(17): 194-5. https://www.cnki.com.cn/Article/CJFDTOTAL-YXYY201917128.htm [10] 杜秀明, 冷忠诚, 苏新森. 肛周脓肿的MRI诊断价值探讨[J]. 现代医用影像学, 2019, 28(4): 741-3. https://www.cnki.com.cn/Article/CJFDTOTAL-XDYY201904008.htm [11] O'Malley RB, Al-Hawary MM, Kaza RK, et al. Rectal imaging: part 2, Perianal fistula evaluation on pelvic MRI: what the radiologist needs to know[J]. AJR Am J Roentgenol, 2012, 199(1): 43-53. doi: 10.2214/AJR.11.8361 [12] 路通, 李忠华, 姜虎, 等. MRI瘘管造影联合直肠内扩张在复发性肛瘘治疗中的效果观察[J]. 中国肛肠病杂志, 2021, 41(3): 49-51. doi: 10.3969/j.issn.1000-1174.2021.03.023 [13] Sainio P. Fistula-in-ano in a defined population. Incidence and epidemiological aspects[J]. Ann Chir Gynaecol, 1984, 73(4): 219-24. [14] Toyonaga T, Matsushima M, Tanaka Y, et al. Microbiological analysis and endoanal ultrasonography for diagnosis of anal fistula in acute anorectal sepsis[J]. Int J Colorectal Dis, 2007, 22(2): 209-13. [15] 魏东, 高春芳. 现代结直肠肛门病学[M]. 西安: 西安交通大学出版社, 2016: 642-3. [16] Hori M, Oto A, Orrin S, et al. Diffusion-weighted MRI: a new tool for the diagnosis of fistula in ano[J]. J Magn Reson Imaging, 2009, 30(5): 1021-6. doi: 10.1002/jmri.21934 [17] 贾瑞娟, 杨侃荣, 赵继泉, 等. 盆腔MRI平扫、钆喷酸葡胺增强扫描及扩散加权成像对盆腔脓肿患者的诊断价值: 64例患者前瞻性研究[J]. 分子影像学杂志, 2020, 43(2): 286-90. doi: 10.12122/j.issn.1674-4500.2020.02.22 [18] 黄瑜亮, 黄斌, 严俊. 结直肠癌的早期诊断技术进展[J]. 分子影像学杂志, 2019, 42(1): 77-80. doi: 10.12122/j.issn.1674-4500.2019.01.18 [19] Bartram C, Buchanan G. Imaging anal fistula[J]. Radiol Clin N Am, 2003, 41(2): 443-57. doi: 10.1016/S0033-8389(02)00122-7 -

 点击查看大图
点击查看大图

计量
- 文章访问数: 269
- HTML全文浏览量: 121
- PDF下载量: 4
- 被引次数: 0