



The clinical research of axillary midline transthoracic approach for the upper and middle thoracic tuberculosis
-
摘要:
目的探讨经腋中线胸腔入路治疗上中胸椎结核的临床研究。 方法于2010年8月~2014年9月采用经腋中线胸腔病灶清除减压植骨内固定治疗上中胸椎结核患者,男13例,女8例。年龄33~77岁,平均45.5岁。所有患者均有结核中毒症状,胸椎后凸畸形。17例有神经压迫症状。 结果随访期内所有患者愈合良好,术后1例出现术区疼痛、麻木,经治疗后缓解。21例患者获得随访15~30个月,平均20.8个月。胸椎后凸角平均矫正1.58°。疼痛视觉模拟评分(VAS)平均改善4.14分,血沉均恢复正常。17例有神经系统症状的患者均有不同程度的恢复。 结论经腋中线胸腔入路可以达到治疗上中胸椎结核的目的。 Abstract:Objective To explore the curative effect of axillary midline transthoracic approach for treatment of upper and middle thoracic tuberculosis. Methods 21 patients with upper and middle thoracic tuberculosis underwent one-stage debridement and bone grafting with internal fixation via axillary midline transthoracic approach. There are 13 men and 8 women aging 35 to 77 year-old, with the average age of 45.5 years old. All patients had various degrees with tuberculosis poisoning symptoms and thoracic kyphotic deformity. Seventeen of the patients have different degrees of nerve compression symptoms. Results All patients recover well during the follow-up period. 1 case got pain, numbness in surgical site after operation, but rapidly alleviated after the treatment. 21 patients were followed from 15 to 30 months, with the average period of 20.8 months. The kyphosis Cobb's angle corrected with the average angle of 1.58° , visual analogue scale (VAS) have improvement with an average score of 4.14. And at the last follow-up, those 17 cases of patients with neurological symptoms impoved in varying degrees. Erythrocyte sedimentation rate (ESR) declined in varying degrees. Conclusions Axillary midline transthoracic approach can achieve the goal of treatment of upper and middle thoracic tuberculosis. -
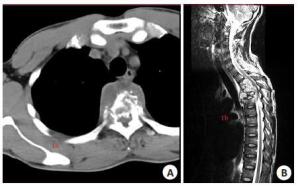
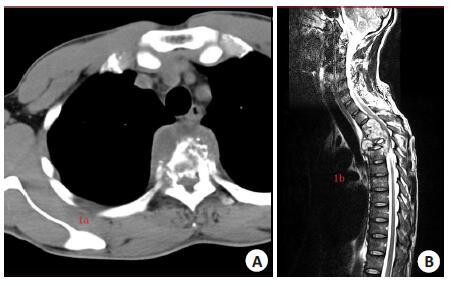
图 1 术前CT与MRI检查结果
Figure 1. The results of preoperative CT and MRI.A: preoperativeCT; B: preoperative MRI.
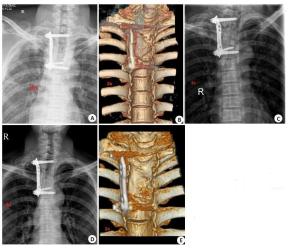
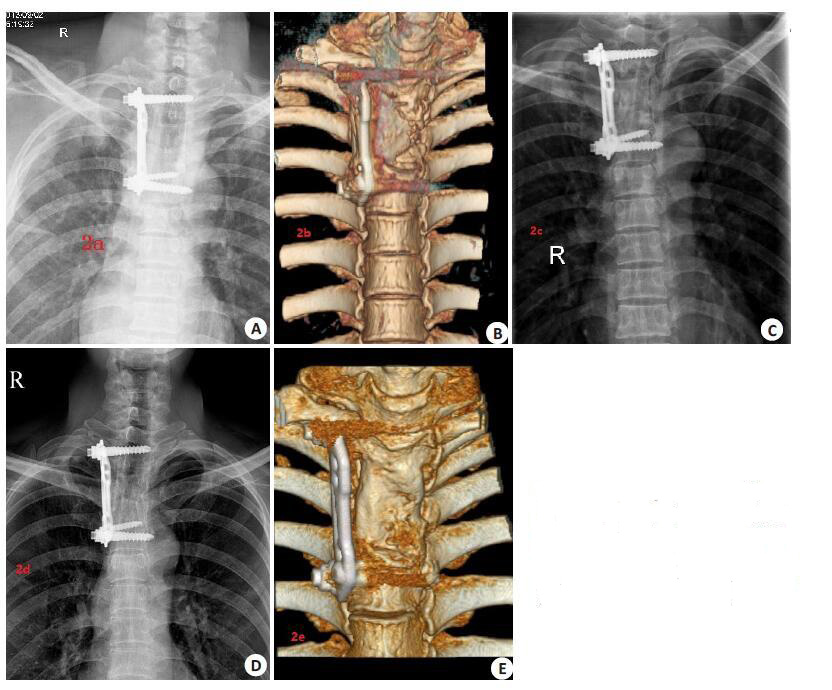
图 2 术后X线与CT检查结果
Figure 2. The results of postoperative ofX-ray and CT
A: Postoperative X-ray; B-C: X-rayand CT after 3 months; D-E: X-rayand CT after 2 years and a half.
表 1 术前与术后各项评估指标对比
Table 1. The ratio of preoperative and postoperative indexes(Mean±SD, n=21)
Groups VAS (score) Kyphosis Cobb's angle (°) ESR (mm/h) Preoperative 5.62±1.16 26.68±6.34° 38.90±16.08 Three months after operation 1.47±1.03 25.13±6.40° 24.38±4.26 Difference 4.14±1.27 1.58±0.58° 2.67±1.24  下载: 导出CSV
下载: 导出CSV
表 2 术前与术后随访神经功能情况对比(Frankel分级)
Table 2. The ratio of preoperative and postoperative neural function(Frankel classification)
Groups Preoperative cases Cases of 1 year after the operation Cases of the last follow-up after the operation Grade A 1 0 0 Grade B 2 0 0 Grade C 10 1 0 Grade D 4 8 9 Grade E 4 12 12 Total 21 21 21
下载: 导出CSV
-
[1] Tavera-Mendoza LE, White JH. Cell defenses and the sun-shine vitamin[J]. Sci Am, 2007, 297(5): 68-70. [2] 詹新立, 肖增明, 贺茂林, 等. 前方经胸骨或侧前方经肩胛下入路手术 治疗上胸椎结核[J]. 中国脊柱脊髓杂志, 2009, 19(11): 808-12. [3] 张祥英. 脊柱结核的外科治疗进展[J]. 中国矫形外科杂志, 2004, 12 (13): 1025-7. [4] 卢长巍. 上胸椎前方手术入路的研究进展[J]. 医学综述, 2013, 19 (15): 2791-3. [5] Narayan SM, Henry HM, Alan L, et al. Tumors of the spine: diagnosis and clinical management [M]. Saunders, 1990. [6] Miller DJ, Lang FF, Walsh GL, et al. Coaxial double-lumen methylmethacrylate Reconstruction in the anterior cervical and upper thoracic spine after tumor resection[J]. J Neurosurg, 2000, 92 (2, S): 181-90. [7] 张忠民, 付忠泉, 尹刚辉, 等. 胸椎结核外科治疗的长期临床随访[J]. 脊柱外科杂志, 2012, 10(4): 198-201. [8] Sharan AD, Przybylski GJ, Tartaglino L. Approaching the upper thoracic vertebrae without sternotomy or thoracotomy - A radiographic analysis with clinical application[J]. Spine (Phila Pa 1976), 2000, 25(8): 910-6. [9] Hamilton A, Webb JK. The role of anterior surgery for vertebral fractures with and without cord compression[J]. Clin Orthop Relat Res, 1994(300): 79-89. [10] Fidler MW, Goedhart ZD. Excision of prolapse of thoracic intervertebral disc. A transthoracic technique[J]. J Bone Joint Surg ( Br Vol), 1984, 66(4): 518-22. [11] 肖增明, 宫德峰, 詹新立, 等. 上胸椎前方手术入路的解剖及其临床意 义[J]. 中华骨科杂志, 2006, 26(3): 183-6. [12] 杨荣利, 曲华毅, 燕太强, 等. 肩胛下经胸入路切除及重建治疗上胸椎 肿瘤[J]. 中华外科杂志, 2008, 46(19): 1486-9. [13] 任先军, 张峡, 王建, 等. 肩胛下高位经胸入路行上胸椎前路减压融 合术[J]. 脊柱外科杂志, 2003, 1(1): 32-4. [14] 何海龙, 叶晓健, 谭俊铭, 等. 胸腔镜辅助下前路减压植骨融合术治疗 合并椎间盘损伤的下胸椎椎体爆裂骨折[J]. 中华骨科杂志, 2011, 31 (10): 1128-31. [15] 霍洪军, 邢文华, 杨学军, 等. 脊柱结核手术治疗方式的选择[J]. 中国 脊柱脊髓杂志, 2011, 21(10): 819-24. [16] 王自立. 恰当选择脊柱结核手术入路[J]. 中国脊柱脊髓杂志, 2012, 22(9): 769-70. [17] 杨永辉, 蔡玉强, 晁建虎, 等. 胸椎结核外科治疗不同术式选择探讨 [J]. 实用骨科杂志, 2014(9): 788-94. [18] 马远征. 关于脊柱结核病灶清除术的入路问题[J]. 中国脊柱脊髓杂 志, 2012, 22(9): 774. [19] [20] 刘鹏, 蒋晖, 瞿东滨, 等. 胸椎和腰椎脊柱结核手术入路术式选择研 究[J]. 中国医科大学学报, 2013, 42(3): 253-6. [21] 范俊, 秦世炳, 董伟杰, 等. 胸椎结核术后常见并发症的临床分析[J]. 北京医学, 2014, 36(3): 184-6. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 621
- HTML全文浏览量: 238
- PDF下载量: 0
- 被引次数: 0