



Clinical application of Iodixanol in hepatic CTA procedure
-
摘要:
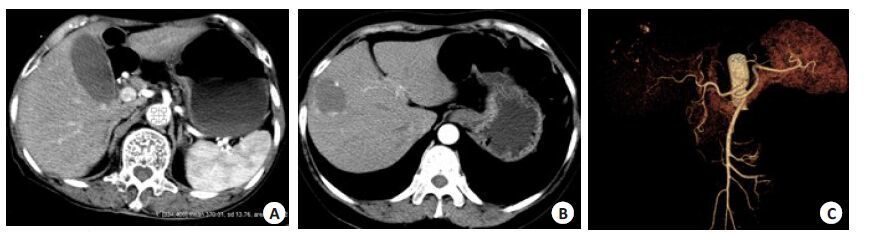
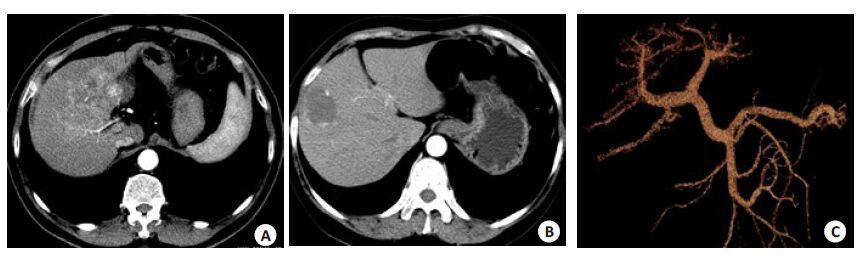
目的通过比较两种不同管电压、不同浓度的非离子型碘对比剂在肝脏血管CTA成像中的增强效果、图像质量及辐射剂量,探索碘克沙醇270 mgI/mL肝血管成像临床应用中的可行性。 方法选择我院76例(36名男性,40名女性)临床怀疑肝胆病变的患者行肝脏血管CTA扫描(动脉期及门脉期),将患者随机分为2组:A组(38例)对比剂为碘普罗胺350、管电压120 kV,B组(38例)碘克沙醇270、管电压100 kV,对比剂用量、注射流速均为1.2 mL/kg及5 mL/s。所有图像均同一图像后处理工作站通过VR、MIP及MPV进行后处理重建,对照2组患者的肝动脉、门静脉主干的CT值、对比噪声比及图像质量,并对照其扫描辐射剂量及对比剂不良反应。 结果两组患者肝动脉、门静脉的CT值、对比噪声比及图像质量均无统计学差异(P>0.05),低浓度组患者所接受的有效辐射剂量明显少于高浓度组,并且出现对比剂注射相关不适感的比例也明显少于高浓度组。 结论低浓度碘对比剂碘克沙醇270 mgI/mL结合低管电压扫描技术可用于肝脏血管CTA成像。 -
关键词:
- 肝动脉 /
- 门静脉 /
- 碘克沙醇270 /
- 辐射剂量 /
- 对比剂注射相关不适感
Abstract:Objective To explore the feasibility of Iodixanol 270 mg/mL in hepatic CTA procedure with comparison of the hepatic CTA enhancement, image quality and radiation dose between two scan procedure with different concentration contrast media and tube voltage. Methods A total of 76 patients (36 men and 40 women) with suspected hepatobiliary disease were underwent hepatic vascular CTA procedure with different contrast media and tube voltage. Patients were divided into 2 groups randomly, 38 in group A received Iopromide 370 mgI/mL at a rate of 5 mL/s with tube voltage of 120 kV, and the remaining 38 patients in group B received Iodixanol 270 mgI/mL at the same flow rate with 100 kV. All the raw data were transferred to an image post-processing workstation for VR, MIP and MPC reconstruction. The CT value, CNR, image quality of the hepatic artery and portal vein were assessed and compared between the groups, also the radiation dose and ADR were compared between the two groups. Results There was no statistically difference of CT value, CNR and image quality between 2 groups (P>0.05). The radiation dose of group B (low concentration group) was significant lower than group A. Incidence of injection related discomfort were less than group A. Conclusion Low concentration contrast media Iodixanol with low tube voltage scan procedure can be applied in the hepatic vascular CTA. -
Key words:
- hepatic artery /
- portal vein /
- iodixanol 270 /
- radiation dose /
- injection related discomfort
-
表 1 两组患者肝动脉、门静脉CNR结果
指标 A组 B组 t P CNRHA 5.02±1.04 4.88±0.98 3.457 0.317 CNRLPV 1.98±0.79 2.01±0.67 2.587 0.143 CNRRPV 1.82±1.04 1.77±0.86 3.334 0.388  下载: 导出CSV
下载: 导出CSV
表 2 两组患者辐射剂量的结果分析(n=38, x±s)
组别 DLP(mGy-cm) CTDIvol(mGy) ED(mSv) A组 2055.4±135.81 85.82±8.98 31.86±2.42 B组 1247.6±208.42 52.45±5.21 17.68±2.49
下载: 导出CSV
-
[1] Kagan A, Sheikh-Hamad D. Contrast-induced kidney injury: focus on modifiable risk factors and prophylactic strategies[J]. Clin Cardiol, 2010, 33(2): 62-6. doi: 10.1002/clc.20687 [2] 舒小钢, 查云飞. 低剂量对比剂CTU的可行性研究[J]. 临床放射学杂志, 2012, 31(4): 567-70. http://www.cnki.com.cn/Article/CJFDTOTAL-LCFS201204031.htm [3] Calvin AD, Misra S, Pflueger A. Contrast-induced acute kidney injury and diabetic nephropathy[J]. Nat Rev Nephrol, 2010, 6(11): 679-88. doi: 10.1038/nrneph.2010.116 [4] 李建华, 贺能树. 碘对比剂肾病的预防措施[J]. 临床放射学杂志, 2009, 28(9): 1331-3. http://www.cnki.com.cn/Article/CJFDTOTAL-LCFS200909051.htm [5] Lenhard DC, Pietsch H, Sieber MA, et al. The osmolality of nonionic, iodinated contrast agents as an important factor for renal safety[J]. Invest Radiol, 2012, 47(9): 503-10. doi: 10.1097/RLI.0b013e318258502b [6] Masui T, Katayama M, Kobayashi S, et al. Intravenous injection of high and medium concentrations of computed tomography contrast media and related heat sensation, local pain, and adverse reactions [J]. J Comput Assist Tomogr, 2005, 29(5): 704-8. doi: 10.1097/01.rct.0000171238.10678.54 [7] 彭主龙. 贺能树.孙丽莎.碘对比剂对红细胞变形能力的影响及其临床意义[J]. 中国医学影像技术, 2000(10): 67-9. http://www.cnki.com.cn/Article/CJFDTOTAL-ZYXX200010050.htm [8] 郑淑梅, 高波, 韩彦玲, 等. 等渗造影剂碘克沙醇在CT增强扫描中的临床应用观察[J]. 哈尔滨医科大学学报, 2007, 41(5): 491-3. http://www.cnki.com.cn/Article/CJFDTOTAL-HYDX200705030.htm [9] Aspelin P, Aubry P, Fransson S, et al. Nephrotoxic effects in high-risk patients undergoing angiography[ J]. N Engl J Med, 2003, 348(6): 491-9. doi: 10.1056/NEJMoa021833 [10] Pugh ND, Sissons GR, Ruttley MS, et al. Iodixanol in femoral arteriography (phase Ⅲ): a comparative double-blind parallel trial between iodixanol and iopromide[J]. Clin Radiol, 1993, 47(2): 96-9. doi: 10.1016/S0009-9260(05)81180-8 [11] Davidson CJ, Laskey WK, Hermiller JB, et al. Randomized trial of contrast media utilization in high-risk PTCA: the COURT trial[J]. Circulation, 2000, 101(18): 2172-7. doi: 10.1161/01.CIR.101.18.2172 [12] Huda W, Scalzetti EM, Levin G. Technique factors and image quality as functions of patient weight at abdominal CT[J]. Radiology, 2000, 217(2): 430-5. doi: 10.1148/radiology.217.2.r00nv35430 [13] Nakayama Y, Awai K, Funama Y, et al. Abdominal CT with low tube voltage: preliminary observations about radiation dose, contrast enhancement, image quality, and noise[J]. Radiology, 2005, 237(3): 945-51. doi: 10.1148/radiol.2373041655 [14] Hernandez-Giron I, Calzado A, Geleijns J, et al. Low contrast detectability performance of model observers based on CT phantom images: kVp influence[J]. Phys Med, 2015, 31(7): 798-807. doi: 10.1016/j.ejmp.2015.04.012 [15] Moos SI, van Vemde DN, Stoker J, et al. Contrast induced nephropathy in patients undergoing intravenous (IV) contrast enhanced computed tomography (CECT) and the relationship with risk factors: a meta-analysis[J]. Eur J Radiol, 2013, 82(9): e387-99. doi: 10.1016/j.ejrad.2013.04.029 -

 点击查看大图
点击查看大图
图(2) / 表(2)
计量
- 文章访问数: 675
- HTML全文浏览量: 246
- PDF下载量: 2
- 被引次数: 0