



Construction of a diagnostic model for smear- negative active pulmonary tuberculosis based on multi-slice CT imaging features
-
摘要:
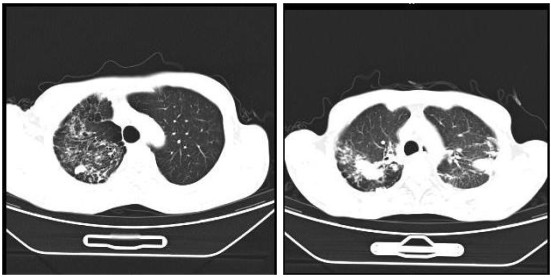
目的 分析菌阴活动性肺结核的多层螺旋CT(MSCT)影像学特征,并构建诊断模型。 方法 选择2020年1月~2023年1月本院收治的肺部疾病患者1016例,按照临床诊断分为菌阴肺结核组(n=478)、非结核肺病组(n=538,其中肺癌200例、肺炎338例),均行MSCT检查,分析两组MSCT影像学特征,以Logistic回归分析明确菌阴活动性肺结核的诊断相关征象,构建菌阴活动性肺结核诊断模型,以ROC曲线下面积评估模型诊断效能。 结果 两组间的树芽征、小叶中心结节、空洞、钙化、分叶征等MSCT征象差异有统计学意义(P<0.05)。Logistic回归分析结果显示树芽征、小叶中心结节、空洞是菌阴活动性肺结核的独立危险因素(P<0.05)。根据Logistic回归获得联合诊断模型方程式:Log(P)=-1.256+1.455×树芽征+0.982×小叶中心结节+1.023×空洞,该模型曲线下面积为0.825,诊断敏感度、特异性分别为93.94%、70.97%。 结论 以MSCT影像学特征构建的菌阴活动性肺结核诊断模型具有较高诊断价值,可为临床诊疗菌阴活动性肺结核提供可靠依据。 Abstract:Objective To analyze the multi- slice CT (MSCT) features of patients with smear- negative active pulmonary tuberculosis and construct a diagnostic model. Methods A total of 1016 patients with pulmonary diseases who were admitted to our hospital were enrolled from January 2020 to January 2023, and they were divided into smear- negative pulmonary tuberculosis group (n=478) and non-tuberculous pulmonary disease group (n=538, including 200 cases of lung cancer and 338 cases of pneumonia) according to clinical diagnosis. All patients received MSCT examination, and their MSCT imaging features were analyzed. Logistic regression analysis was conducted to identify the signs related to the diagnosis of smearnegative active pulmonary tuberculosis, and a diagnostic model for smear- negative active pulmonary tuberculosis was constructed. The diagnostic efficiency of the model was evaluated with AUC. Results There were statistically significant differences in MSCT signs such as tree in bud, centrilobular nodule, cavity, calcification and lobulation between the two groups (P < 0.05). Logistic regression analysis found that tree in bud sign, centrilobular nodule and cavity were independent risk factors for smear-negative active pulmonary tuberculosis (P < 0.05). The equation of the combined diagnosis model constructed based on logistic regression analysis was as follow: Log(P)=-1.256+1.455×tree in bud sign+0.982×centrilobular nodule+1.023×cavity. The AUC, sensitivity and specificity of this model were 0.825, 93.94% and 70.97%, respectively. Conclusion The diagnostic model constructed based on MSCT imaging features is of high value in diagnosis of smear- negative active pulmonary tuberculosis and can provide a reliable basis for clinical diagnosis and treatment of the disease. -

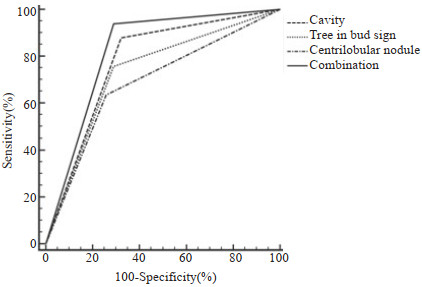
图 1 MSCT影像学特征诊断菌阴活动性肺结核的ROC曲线
Figure 1. ROC curve of MSCT imaging features in diagnosis of smearnegative active pulmonary tuberculosis.
表 1 两组MSCT影像学特征比较
Table 1. Comparison of MSCT imaging features between the two groups (n)
MSCT signs Smear-negative pulmonary tuberculosis group(n=478) Non-tuberculous pulmonary disease group(n=538) χ2 P Tree in bud sign 344.689 <0.001 Yes 381 115 No 97 423 Lobular consolidation 1.340 0.247 Yes 227 236 No 251 302 Centrilobular nodule 594.902 <0.001 Yes 445 89 No 33 449 Nodule with blurred border 0.407 0.523 Yes 310 300 No 368 238 Ground-glass opacity 1.462 0.227 Yes 212 259 No 266 279 Cavity 52.869 <0.001 Yes 95 27 No 383 511 Pulmonary consolidation 1.837 0.175 Yes 349 352 No 129 186 Bronchiectasis 2.855 0.091 Yes 267 272 No 211 266 Pleural effusion 0.099 0.753 Yes 79 85 No 399 453 Calcification 146.919 <0.001 Yes 172 30 No 306 508 Fibrous shadow 3.221 0.073 Yes 418 409 No 60 229 Enlargement of lymph nodes 0.004 0.952 Yes 255 286 No 223 252 Plaque 3.661 0.056 Yes 130 176 No 348 362 Spicule sign 0.590 0.442 Yes 150 181 No 328 357 Lobulation sign 50.104 0.001 Yes 81 198 No 397 147 Satellite lesion 1.460 0.227 Yes 177 159 No 301 119  下载: 导出CSV
下载: 导出CSV
表 2 菌阴活动性肺结核的多因素Logistic回归分析
Table 2. Multivariate Logistic regression analysis of smear-negative active pulmonary tuberculosis
MSCT signs β SE Wald χ2 OR 95% CI P Tree in bud sign 1.455 0.349 17.381 4.284 2.161-8.491 <0.001 Centrilobular nodule 0.982 0.401 5.997 2.670 1.217-5.859 0.015 Cavity 1.023 0.326 9.847 2.782 1.468-5.270 0.002 Calcification 0.767 0.458 2.805 2.153 0.877-5.284 0.095 Lobulation sign -0.869 0.642 1.832 0.419 0.119-1.476 0.177 Constant -1.256 0.571 <0.001
下载: 导出CSV
表 3 MSCT征象单独及联合诊断菌阴活动性肺结核的价值
Table 3. Value of MSCT signs alone and in combination in diagnosis of smear-negative active pulmonary tuberculosis
MSCT signs AUC Youden index P 95% CI Sensitivity(%) Specificity(%) Tree in bud sign 0.734 0.467 <0.001 0.608-0.836 75.76 70.97 Centrilobular nodule 0.689 0.378 <0.001 0.561-0.799 63.64 74.19 Cavity 0.778 0.556 <0.001 0.657-0.872 87.88 67.74 Combination 0.825 0.649 <0.001 0.709-0.908 93.94 70.97
下载: 导出CSV
-
[1] Goletti D, Delogu G, Matteelli A, et al. The role of IGRA in the diagnosis of tuberculosis infection, differentiating from active tuberculosis, and decision making for initiating treatment or preventive therapy of tuberculosis infection[J]. Int J Infect Dis, 2022, 124: S12-9. doi: 10.1016/j.ijid.2022.02.047 [2] 刘文林, 赵静, 崔琼. 肺组织结核菌培养、结核分枝杆菌-DNA检测对菌阴肺结核的诊断价值[J]. 医学临床研究, 2022(6): 937-9. [3] 刘二勇, 王前, 周林, 等. 我国部分地区病原学检测阴性肺结核诊断质量现状分析[J]. 中国防痨杂志, 2020, 42(9): 916-20. [4] 苏景瑞, 裴文杰. 不典型肺结核18例临床误诊分析[J]. 临床误诊误治, 2022, 35(6): 1-4. [5] 刘晓晨, 蔡思鹏, 刘文亚, 等. MRI及CT在菌阴肺结核诊断中的应用体会[J]. 中国医学计算机成像杂志, 2022, 28(3): 291-5. [6] 宗素英. 良、恶性肺磨玻璃结节MSCT影像学特征及诊断价值[J]. 中国CT和MRI杂志, 2022, 20(1): 98-100. [7] 李小容, 唐川婷, 高广川, 等. MSCT联合血清MP-IgM、MP-Ab检测对小儿支原体感染肺炎有较高的诊断价值[J]. 分子影像学杂志, 2022, 45(3): 378-81. doi: 10.12122/j.issn.1674-4500.2022.03.14 [8] 胡蝶. 多层螺旋CT对肺脓肿诊断及疗效评估的价值分析[J]. 中国CT和MRI杂志, 2020, 18(1): 82-4. [9] 中华人民共和国国家卫生和计划生育委员会. 肺结核诊断WS 288— 2017[J]. 中国感染控制杂志, 2018, 17(7): 642-52. [10] Ettinger DS, Aisner DL, Wood DE, et al. NCCN guidelines insights: non-small cell lung cancer, version 5.2018[J]. J Natl Compr Canc Netw, 2018, 16(7): 807-21. [11] 中华医学会, 中华医学会杂志社, 中华医学会全科医学分会, 等. 成人社区获得性肺炎基层诊疗指南(2018年)[J]. 中华全科医师杂志, 2019, 18(2): 117-26. [12] 其梅, 曹嘎, 张书. 2016-2020年拉萨市结核病病原学阳性情况分析与分子生物学检测设备的应用效果评价[J]. 预防医学情报杂志, 2021, 37(6): 855-8. [13] 邢少杰, 李旭, 曹兴旺. 支气管镜检查联合TB-RNA、血清TB-SA抗体测定用于菌阴肺结核诊断的特异性与敏感性分析[J]. 中华肺部疾病杂志: 电子版, 2020, 13(6): 794-6. [14] Chen J, Marusinec R, Brown R, et al. Epidemiology of culturenegative pulmonary tuberculosis-alameda County, 2010-2019[J]. J Public Health Manag Pract, 2023, 29(3): 353-60. [15] 张学文, 李国栋, 陈晨楠, 等. 三种检测技术在涂阴肺结核快速诊断中的应用[J]. 中华医院感染学杂志, 2022, 32(5): 650-3. [16] 马建军, 张铁娟, 侯伟, 等. 含分子生物学检测技术诊断流程在肺结核患者发现中的应用情况[J]. 中国防痨杂志, 2021, 43(10): 1089- 95. [17] 宗玲青, 钮志林, 赵刚, 等. 基因芯片技术联合T细胞斑点试验诊断肺结核及基因芯片技术检测耐药基因的应用研究[J]. 实用临床医药杂志, 2022, 26(10): 7-10, 14. [18] 何洪淳, 唐强. 脊柱结核病灶MSCT、MRI影像学表现及对内镜手术指导价值分析[J]. 中国CT和MRI杂志, 2022, 20(3): 159-61. [19] 欧国建, 凌杰, 黄和平. MSCT征象特征与活动性肺结核诊断及临床症状体征的相关性分析[J]. 临床和实验医学杂志, 2023, 22(12): 1319-23. [20] 李孝东, 廖潜, 游玉峰. 多层螺旋CT在肺结核空洞与肺癌空洞鉴别诊断中的临床应用[J]. 中国肿瘤临床与康复, 2021, 28(7): 850-3. [21] 徐宝静, 李云峰, 刘贵林, 等. 多层螺旋CT在诊断和鉴别单发性结核空洞和肺癌空洞中的应用价值[J]. 中国临床医生杂志, 2020, 48 (11): 1304-7. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 92
- HTML全文浏览量: 44
- PDF下载量: 5
- 被引次数: 0