



Value of multimodal ultrasound in the diagnosis in optimizing BI-RADS 4 breast lesions category
-
摘要:
目的 探讨乳腺自动容积成像(ABVS)、超声弹性评分(UES)及两者联合在校正乳腺影像报告和数据系统分级(BI-RADS)4类乳腺肿块BI-RADS分级中的应用价值。 方法 收集我院经常规超声诊断为BI-RADS 4类的乳腺肿块患者109例, 共113个肿块。经ABVS及UES校正BI-RADS分级后, 与病理结果对比, 绘制ROC曲线, 比较常规超声、ABVS、UES、ABVS联合UES诊断BI-RADS 4类乳腺肿块的差异。 结果 109例患者113个肿块中包含良性78个, 恶性35个, ABVS联合UES校正后的敏感度、特异性、准确性、ROC曲线下面积分别为94.29%、93.59%、93.80%、0.975。 结论 ABVS联合UES有助于提高BI-RADS 4类肿块的总体诊断效能。两者联合诊断可以取长补短, 提高诊断率。 -
关键词:
- 乳腺自动容积成像 /
- 超声弹性评分 /
- 常规超声 /
- 乳腺影像报告和数据系统分级 /
- 乳腺肿块
Abstract:Objective To explore the application value of automatic breast volume scanning (ABVS), ultrasound elastography score (UES) and their combination in correcting the BI-RADS 4 breast lesions. Methods A total of 113 patients with 109 breast lesions diagnosed with BI-RADS 4 by conventional ultrasound were collected.After the BI-RADS grading was corrected by ABVS and UES, the ROC curve was compared with the pathological results, and the differences in the diagnosis of BI-RADS 4 breast lesions by conventional ultrasound, ABVS, UES, ABVS combined with UES were compared. Results Among 113 masses in 109 patients, 78 were benign and 35 were malignant.The sensitivity, specificity, accuracy and area under the ROC curve of ABVS combined with UES were 94.29%, 93.59%, 93.80% and 0.975 respectively. Conclusion US+ABVS+UES can significantly improve the diagnostic efficiency and accuracy of US in the diagnosis of BI-RADS 4 breast lesions. -

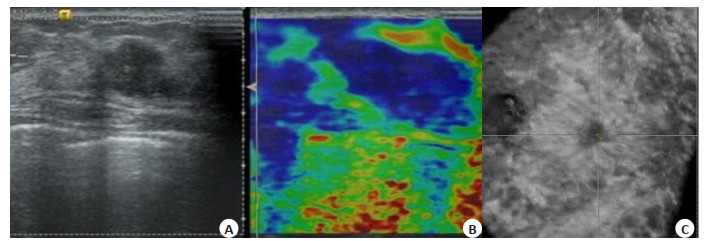
图 1 浸润性导管癌患者的US、UE、ABVS图像
Figure 1. US, UE, ABVS images of patients with invasive ductal carcinoma. A: Conventional ultrasound showed irregularly shaped lesions with blurred borders, and the diagnosis was BI-RADS 4A; B: UE image showing almost the entire lesion in blue with a UE score of 5; C: ABVS coronal converging sign. Adjusted to BI-RADS 5 according to the combined diagnostic optimization criteria in Tab. 1.

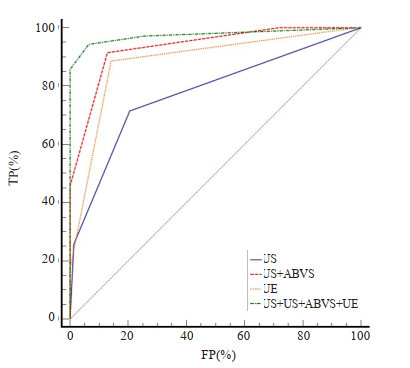
图 2 US、ABVS、UES、ABVS联合UES校正BI-RADS 4级乳腺肿块的ROC曲线
Figure 2. ROC curve of US, ABVS, UES, ABVS plus UES corrected for BI-RADS grade 4 breast lesions.
ABVS UES 1-3 4-5 ABVS appear complete medium-high echo boundaries Downgraded two levels Maintain the original level No malignant signs were observed in ABVS Downgraded one level/two levels Upgraded one level The coronal plane presents an additional malignant feature that was not present on conventional ultrasound Maintain the original level Upgraded two levels Once retraction phenomenon appears in the coronal plane of ABVS Upgraded to 4C Upgraded to 5 ABVS: Automated breast volume scanning; UES: Ultrasound elastography score.  下载: 导出CSV
下载: 导出CSV
表 2 常规超声及经ABVS联合UE校正后的乳腺肿块BI-RADS分类
Table 2. BI-RADS classification of breast lesions corrected for conventional ultrasound and ABVS combined with UE (n)
BI-RADS-US category BI-RADS-US category after ABVS combined with UES Pathology results Benign Malignant 4A(n=72) 3(n=55) 54 1 4A(n=8) 8 0 4C(n=3) 0 3 5(n=6) 0 6 4B(n=31) 3(n=4) 4 0 4A(n=8) 7 1 4B(n=7) 4 3 4C(n=7) 0 7 5(n=5) 0 5 4C(n=10) 4B(n=1) 1 0 4C(n=5) 0 5 5(n=4) 0 4
下载: 导出CSV
表 3 US、ABVS、UES、ABVS联合UES校正BI-RADS分类后的敏感性、特异性、准确率、阳性预测值、阴性预测值
Table 3. Sensitivity, specificity, accuracy, positive predictive value, negative predictive value, after US, ABVS, UES, ABVS and UES corrected BI-RADS classification
Methods Sensitivity (%) Specificiy (%) Positive predictive value (%) Negative predictive value (%) Accuracy (%) AUC 95% CI US 71.43 79.49 61.0 86.1 76.99 0.776 0.688, 0.849 ABVS 91.43 87.18 76.2 95.8 88.49 0.934 0.872, 0.972 UE 88.57 85.90 73.8 94.4 86.72 0.885 0.812, 0.937 US+ABVS+UE 94.29 93.59 100 94.0 93.80 0.975 0.926, 0.995
下载: 导出CSV
-
[1] Lei SY, Zheng RS, Zhang SW, et al. Global patterns of breast cancer incidence and mortality: a population-based cancer registry data analysis from 2000 to 2020[J]. 癌症通讯: 英文, 2021(11): 1183-94. [2] Cao W, Chen HD, Yu YW, et al. Changing profiles of cancer burden worldwide and in China: a secondary analysis of the global cancer statistics 2020[J]. Chin Med J (Engl), 2021, 134(7): 783-91. doi: 10.1097/CM9.0000000000001474 [3] 李崎, 温力牧, 吴旻骅, 等. 不同年龄段三阴性乳腺癌患者临床病理特点与生存状况研究[J]. 现代实用医学, 2019, 31(3): 292-5, 276. [4] Burnside ES, Sickles EA, Bassett LW, et al. The ACR BI-RADS experience: learning from history[J]. J Am Coll Radiol, 2009, 6(12): 851-60. doi: 10.1016/j.jacr.2009.07.023 [5] Elezaby M, Li G, Bhargavan-Chatfield M, et al. ACR BI-RADS assessment category 4 subdivisions in diagnostic mammography: utilization and outcomes in the national mammography database[J]. Radiology, 2018, 287(2): 416-22. doi: 10.1148/radiol.2017170770 [6] Wojcinski S, Gyapong S, Farrokh A, et al. Diagnostic performance and inter-observer concordance in lesion detection with the automated breast volume scanner (ABVS)[J]. BMC Med Imag, 2013, 13(1): 1-12. doi: 10.1186/1471-2342-13-1 [7] Itoh A, Ueno E, Tohno E, et al. Breast disease: clinical application of US elastography for diagnosis[J]. Radiology, 2006, 239(2): 341-50. doi: 10.1148/radiol.2391041676 [8] 马骥, 张艳, 陈青青, 等. 常规超声联合ABVS在乳腺BI-RADS 4类小结节诊断中的价值[J]. 同济大学学报: 医学版, 2021, 42(6): 825-30. [9] Evans A, Whelehan P, Thomson K, et al. Quantitative shear wave ultrasound elastography: initial experience in solid breast masses[J]. Breast Cancer Res, 2010, 12(6): 1-11. [10] Ren TT, Li XR, Xiang Y, et al. The diagnostic significance of the BI-RADS classification combined with automated breast volume scanner and shear wave elastography for breast lesions[J]. J Ultrasound Med, 2023, 42(7): 1459-69. doi: 10.1002/jum.16154 [11] 魏均羽, 徐皙婷, 潘丽莎, 等. 自动乳腺全容积成像联合超声弹性成像与传统手持二维超声对乳腺占位性疾病诊断价值的比较[J]. 广西医学, 2017, 39(6): 786-90. [12] 肖露, 褚雯, 王华. 超微血管成像技术对乳腺肿瘤血管形态分布特征及其诊断效能的初步分析[J]. 中华超声影像学杂志, 2018, 27(11): 973-6. doi: 10.3760/cma.j.issn.1004-4477.2018.11.012 [13] Liu XJ, Zhu Y, Liu PF, et al. Elastography for breast cancer diagnosis: a useful tool for small and BI-RADS 4 lesions[J]. Asian Pac J Cancer Prev, 2015, 15(24): 10739-43. doi: 10.7314/APJCP.2014.15.24.10739 [14] Burton GJ, Jauniaux E. Pathophysiology of placental-derived fetal growthrestriction[J]. Am J Obstet Gynecol, 2018, 218(2): S745-61. doi: 10.1016/j.ajog.2017.11.577 [15] Wenkel E, Heckmann M, Heinrich M, et al. Automated breast ultrasound: lesion detection and BI-RADS™ classification a pilot study[J]. Fortschr Rö ntgenstr, 2008, 180(9): 804-8. doi: 10.1055/s-2008-1027563 [16] Xiao YM, Zhou QC, Chen ZH. Automated breast volume scanning versus conventional ultrasound in breast cancer screening[J]. Acad Radiol, 2015, 22(3): 387-99. doi: 10.1016/j.acra.2014.08.013 [17] Kaplan SS. Automated whole breast ultrasound[J]. Radiol Clin N Am, 2014, 52(3): 539-46. doi: 10.1016/j.rcl.2014.01.002 [18] Chang RF, Huang SF, Wang LP, et al. Microcalcification detection in 3-D breast ultrasound[C]/2005 IEEE Engineering in Medicine and Biology 27th Annual Conference. Shanghai, China. IEEE, 2006: 6297-300. [19] Chen L, Chen Y, Diao XH, et al. Comparative study of automated breast 3-D ultrasound and handheld B-mode ultrasound for differentiation of benign and malignant breast masses[J]. Ultrasound Med Biol, 2013, 39(10): 1735-42. doi: 10.1016/j.ultrasmedbio.2013.04.003 [20] Fleury E. The importance of breast elastography added to the BI-RADS® (5th edition) lexicon classification[J]. Rev Assoc Med Bras, 2015, 61(4): 313-6. doi: 10.1590/1806-9282.61.04.313 [21] Gong X, Xu QH, Xu ZL, et al. Real-time elastography for the differentiation of benign and malignant breast lesions: a meta-analysis[J]. Breast Cancer Res Treat, 2011, 130(1): 11-8. doi: 10.1007/s10549-011-1745-2 [22] 智慧, 罗葆明, 欧冰, 等. 对乳腺弹性成像5分评分法的进一步探讨[J]. 中国超声医学杂志, 2007, 23(5): 349-51. [23] 张加孟, 王芳, 尹立雪. 超声弹性应变率比值法及弹性成像评分法对乳腺肿块定性诊断的比较[J]. 解放军医药杂志, 2017, 29(11): 93-5, 100 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 100
- HTML全文浏览量: 59
- PDF下载量: 3
- 被引次数: 0