



Construction and evaluation of a near-term prognostic model for aneurysmal subarachnoid hemorrhage based on arterial spin labeling: a prospective study
-
摘要:
目的 构建基于动脉自旋标记的动脉瘤性蛛网膜下腔出血(aSAH)短期预后模型,评价模型效能。 方法 前瞻性选取本院的107例aSAH患者作为研究对象,均行动脉自旋标记检查。根据出院后90 d的改良Rankin量表评分将患者分为预后良好组和预后不良组。比较2组的年龄、Hunt-Hess量表评分、改良Fisher量表评分、格拉斯哥昏迷量表(GCS)评分及血细胞参数等数据。用LASSO-Logistic回归分析aSAH预后的风险因素。构建预后模型,采用ROC曲线、校准曲线和决策曲线分析评估模型效能。 结果 预后不良组的年龄、Hunt-Hess量表评分、改良Fisher量表评分、中性粒细胞、淋巴细胞、中性粒细胞/淋巴细胞比值和系统免疫炎症指数均高于预后良好组(P < 0.05),GCS评分、血小板/淋巴细胞比值、同侧局部脑血流(rCBF)值和rCBF比值均低于预后良好组(P < 0.05)。LASSO-Logistic回归分析结果显示,年龄 > 44岁和Hunt-Hess量表评分3⁓5分是aSAH预后的独立危险因素(P < 0.05),GCS评分 > 9分和rCBF比值> 0.66是aSAH预后的独立保护因素(P < 0.05)。模型A(由年龄、Hunt-Hess量表评分和GCS评分构成,0.961)和模型B(由年龄、Hunt-Hess量表评分、GCS评分和rCBF比值构成,0.981)的ROC曲线下面积差异无统计学意义(P > 0.05)。模型A的校准曲线与理想曲线重合度中等,模型B的校准曲线与理想曲线重合度高;模型A(0.042)的平均绝对误差值高于模型B(0.014)。在大部分风险阈值范围内,模型B的净收益均高于模型A。 结论 aSAH患者的年龄、Hunt-Hess量表评分和GCS评分有助于判断其不良预后。联合rCBF比值构建的模型判断aSAH患者不良预后的价值更高。 Abstract:Objective To develop a short-term prognostic model for aneurysmal subarachnoid hemorrhage (aSAH) using arterial spin labeling and to assess the model's efficacy. Methods A total of 107 aSAH patients from our hospital underwent arterial spin labeling examination and were prospectively selected as study subjects. Patients were classified into good and poor prognosis groups based on their modified Rankin scale scores at 90 days post-discharge. Comparisons between the two groups were conducted for age, Hunt-Hess scale score, modified Fisher scale score, Glasgow coma scale (GCS) score, and blood cell parameters. Risk factors for the aSAH prognosis were then analyzed using LASSO-Logistic regression. A prognostic model was developed, and its effectiveness was evaluated using ROC curves, calibration curves, and decision curve analysis. Results Compared to the good prognosis group, the poor prognosis group exhibited higher levels of age, Hunt-Hess scale score, modified Fisher scale score, neutrophils, lymphocytes, neutrophils/lymphocytes and systemic immune inflammation index (P < 0.05). Conversely, the GCS score, platelets/lymphocytes, ipsilateral regional cerebral blood flow (rCBF) values, and rCBF ratio were lower than those in the good prognosis group (P < 0.05). LASSO-Logistic regression analysis revealed that age > 44 years old and a Hunt-Hess scale score of 3-5 were independent risk factors for the prognosis of aSAH (P < 0.05), while a GCS score > 9 and an rCBF ratio > 0.66 were independent protective factors for the prognosis of aSAH (P < 0.05). The model A, consisting of age, Hunt-Hess scale score, and GCS score, had an area under the ROC curve of 0.961, which was not statistically significantly different from the area under the ROC curve of model B, consisting of age, Hunt-Hess scale score, GCS score, and rCBF ratio (0.981) (P > 0.05). While the calibration curve of model A moderately overlapped with the ideal curve, model B exhibited a high overlap with the ideal curve. Moreover, the mean absolute error value was higher in model A (0.042) than in model B (0.014). The net benefit of model B outweighed that of model A across most of the risk threshold range. Conclusion The age, Hunt-Hess scale score, and GCS score of aSAH patients are significant in predicting poor prognosis. Incorporating the rCBF ratio into the model was found to enhance its value in assessing poor prognosis in aSAH patients. -
Key words:
- arterial spin labeling /
- aneurysm /
- subarachnoid hemorrhage /
- prognosis /
- model
-

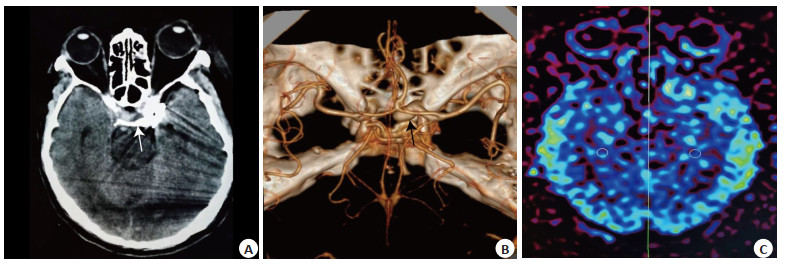
图 1 61岁女性患者的影像学表现
Figure 1. Imaging of a 61-year-old female patient. The patient was diagnosed with SAH on CT scan (A); anterior circulation aneurysm confirmed on digital subtraction angiography (B); CBF map (C).

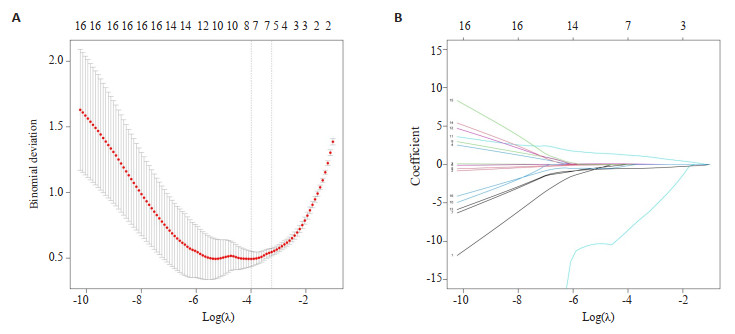
图 2 LASSO回归分析结果
Figure 2. LASSO regression analysis results. A: Range of λ values; B: Coefficients of each variable.

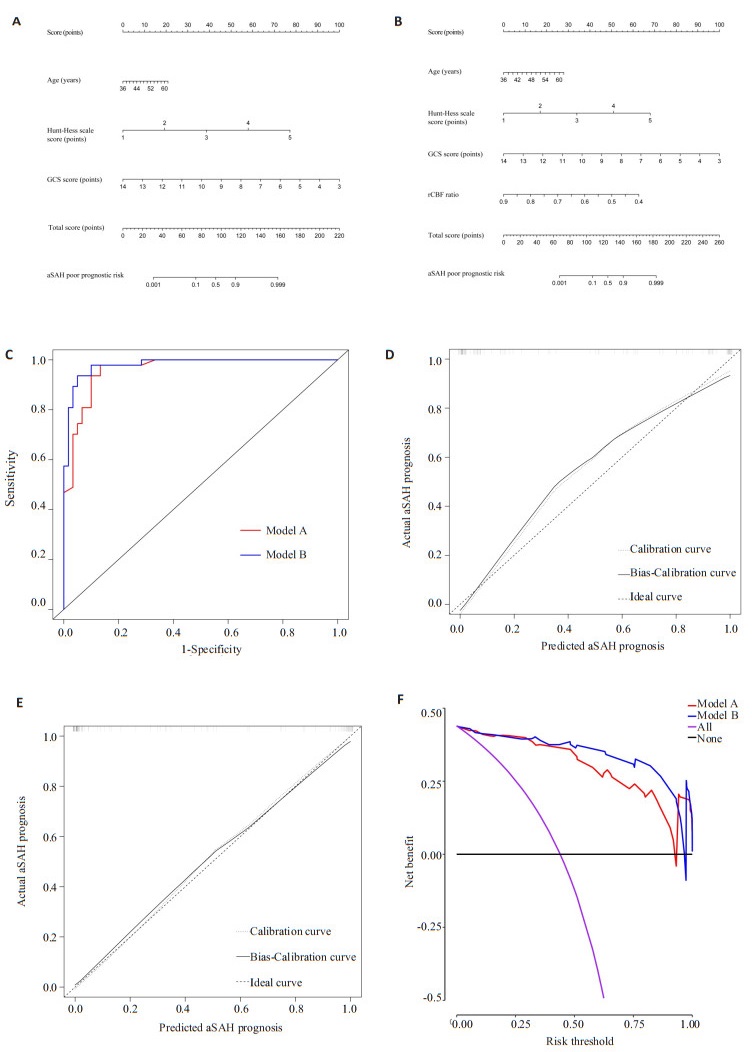
图 3 模型及评价结果
Figure 3. Models and evaluation results. A: Nomogram of model A; B: Nomogram of model B; C: ROC curve; D: Calibration curve of model A; E: Calibration curve of model B; F: DCA curve.
表 1 预后不良组和预后良好组临床资料比较
Table 1. Comparison of baseline information between the poor and good prognosis groups
Items Good prognosis group(n=60) Poor prognosis group(n=47) Z/χ2/t P Age(years) 43(41,45) 48(44,54) 3.987 < 0.001 Gender 0.079 0.778 Male 22(36.67) 16(34.04) Female 38(63.33) 31(65.96) BMI(kg/m2) 25.48±2.39 25.59±2.04 0.246 0.806 Diabetes mellitus 13(21.67) 8(17.02) 0.361 0.548 Hypertension 31(51.67) 31(65.96) 2.209 0.137 Aneurysm location 0.048 0.826 Pre-circulation 37(61.67) 28(59.57) Post-circulation 23(38.33) 19(40.43) Hunt-Hess scale score 2(2,2) 3(3,4) 7.682 < 0.001 Modified Fisher scale score 2(1,2) 3(2,3) 6.713 < 0.001 GCS score 10(9,12) 7(5,8) 7.932 < 0.001 Treatment 2.185 0.139 Surgery 15(25.00) 18(38.30) Intervention 45(75.00) 29(61.70) Cerebral vasospasm 16(26.67) 18(38.30) 1.645 0.200 Blood cell parameters NEU(×109/L) 10.52±2.08 13.69±2.47 7.188 < 0.001 LYM(×109/L) 1.14±0.10 1.27±0.08 7.405 < 0.001 PLT(×109/L) 183.90(158.83,234.14) 186.23(157.43,228.04) 0.025 0.980 NLR 8.96(7.61,11.11) 11.12(9.10,12.46) 3.477 0.001 PLR 164.86(135.86,204.18) 146.56(123.73,176.00) 2.348 0.019 SII 1778.40(1249.99,2303.51) 1933.62(1676.91,2520.86) 1.977 0.048 GCS: Glasgow coma scale; NEU: neutrophil; LYM: lymphocyte; PLT: platelet; SII: systemic immune inflammation index; NLR=NEU/LYM; PLR=PLT/LYM.  下载: 导出CSV
下载: 导出CSV
表 2 预后不良组和预后良好组的ASL参数比较
Table 2. Comparison of ASL parameters between the poor and good prognosis groups (Mean±SD)
Group Ipsilateral rCBF[mL/(100 g·min)] Contralateral rCBF[(mL/(100 g·min)] rCBF ratio Good prognosis group(n=60) 35.74±4.57 50.89±3.31 0.71(0.63, 0.80) Poor prognosis group(n=47) 31.26±3.59 52.18±3.76 0.60(0.54, 0.66) t/Z 5.511 1.884 4.994 P < 0.001 0.062 < 0.001 rCBF: Regional cerebral blood flow.
下载: 导出CSV
表 3 aSAH预后的风险因素的Logistic回归分析结果
Table 3. Logistic regression analysis results of risk factors for aSAH prognosis
Variables β SE Wald P OR 95% CI Age 1.741 0.756 5.307 0.021 5.701 1.296-25.065 Hunt-Hess scale score 3.443 0.795 18.780 < 0.001 31.289 6.593-148.493 GCS score -3.258 1.261 6.679 0.010 0.038 0.003-0.455 rCBF ratio -1.435 0.698 4.225 0.040 0.238 0.061-0.935 Constant -1.928 0.882 4.772 0.029 0.145 - Note: Age≤44 years (median)=0, > 44 years=1; Hunt-Hess scale score 1-2=0, 3-5=1; GCS score ≤9 (median)=0, > 9=1; rCBF ratio ≤0.66 (median)=0, > 0.66=1.
下载: 导出CSV
-
[1] Russel CK. Spontaneous subarachnoid haemorrhage[J]. Can Med Assoc J, 1933, 28(2): 133-40. [2] Feigin VL, Stark BA, Johnson CO, et al. Global, regional, and national burden of stroke and its risk factors, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019[J]. Lancet Neurol, 2021, 20(10): 795-820. doi: 10.1016/S1474-4422(21)00252-0 [3] Etminan N, Chang HS, Hackenberg K, et al. Worldwide incidence of aneurysmal subarachnoid hemorrhage according to region, time period, blood pressure, and smoking prevalence in the population: a systematic review and meta-analysis[J]. JAMA Neurol, 2019, 76(5): 588-97. doi: 10.1001/jamaneurol.2019.0006 [4] 中华医学会神经病学分会, 中华医学会神经病学分会脑血管病学组. 中国蛛网膜下腔出血诊治指南2015[J]. 中华神经科杂志, 2016, 49(3): 182-91. [5] Roland R, Christian S, Jürgen G, et al. Early cisternal fibrinolysis is more effective than rescue spasmolysis for the prevention of delayed infarction after subarachnoid haemorrhage[J]. Stroke Vasc Neurol, 2022, 7(2): 108-13. doi: 10.1136/svn-2021-001146 [6] Wenneberg SB, Block L, Sörbo A, et al. Long-term outcomes after aneurysmal subarachnoid hemorrhage: a prospective observational cohort study[J]. Acta Neuro Scandinavica, 2022, 146(5): 525-36. doi: 10.1111/ane.13674 [7] Zhou J, Ying X, Zhang J, et al. Emerging role of serum dickkopf-1 in prognosis of aneurysmal subarachnoid hemorrhage[J]. Clin Chim Acta, 2021, 521: 116-21. doi: 10.1016/j.cca.2021.07.009 [8] 中国医师协会神经介入专业委员会, 中国颅内动脉瘤计划研究组. 中国颅内破裂动脉瘤诊疗指南2021[J]. 中国脑血管病杂志, 2021, 18(8): 546-74. doi: 10.3969/j.issn.1672-5921.2021.08.007 [9] 陈琳. 磁共振3D ASL全脑灌注成像在动脉瘤性蛛网膜下腔出血后延迟性脑缺血中的应用研究[D]. 石河子: 石河子大学, 2017. [10] Tsivgoulis G, Palaiodimou L, Stefanou MI, et al. Predictors of functional outcome after symptomatic intracranial hemorrhage complicating intravenous thrombolysis: results from the SITS-ISTR[J]. Eur J Neurol, 2023, 30(10): 3161-71. doi: 10.1111/ene.15968 [11] 张鹏, 李育平, 王晓东, 等. 结合炎症反应指数的Nomogram模型对aSAH患者预后预测的价值[J]. 临床神经外科杂志, 2020, 17(2): 216-20. [12] Wan XC, Wu X, Kang JW, et al. Prognostic model for aneurysmal subarachnoid hemorrhage patients requiring mechanical ventilation[J]. Ann Clin Transl Neurol, 2023, 10(9): 1569-77. doi: 10.1002/acn3.51846 [13] Zhou Z, Lu W, Zhang C, et al. A visualized MAC nomogram online predicts the risk of three-month mortality in Chinese elderly aneurysmal subarachnoid hemorrhage patients undergoing endovascular coiling[J]. Neurol Sci, 2023, 44(9): 3209-20. doi: 10.1007/s10072-023-06777-x [14] 王淇民, 杨璇, 高飞. 脑电图联合脑CT灌注成像评定动脉瘤性蛛网膜下腔出血患者预后的价值[J]. 中国实用神经疾病杂志, 2021, 24(12): 1061-6. [15] 胡平, 叶立果, 邓钢, 等. 基于机器学习早期预测蛛网膜下腔出血后迟发性脑缺血和不良预后的研究进展[J]. 中国脑血管病杂志, 2022, 19(7): 504-8. [16] Lindner T, Bolar DS, Achten E, et al. Current state and guidance on arterial spin labeling perfusion MRI in clinical neuroimaging[J]. Magn Reson Med, 2023, 89(5): 2024-47. doi: 10.1002/mrm.29572 [17] Zhang MN, Shi Q, Yue Y, et al. Evaluation of T2-FLAIR combined with ASL on the collateral circulation of acute ischemic stroke[J]. Neurol Sci, 2022, 43(8): 4891-900. doi: 10.1007/s10072-022-06042-7 [18] Fan HL, Su P, Da May Lin D, et al. Simultaneous hemodynamic and structural imaging of ischemic stroke with magnetic resonance fingerprinting arterial spin labeling[J]. Stroke, 2022, 53(6): 2016-25. doi: 10.1161/STROKEAHA.121.037066 [19] Anna L, Klaus B, Verena R, et al. Lower initial Red Blood Cell Count in Cerebrospinal Fluid predicts Good Functional Outcome in Patients with Spontaneous Subarachnoid Hemorrhage[J]. Eur J Neurol, 2023, 30(8): 2315-23. doi: 10.1111/ene.15845 [20] Zhou ZX, Liu ZH, Yang H, et al. A nomogram for predicting the risk of poor prognosis in patients with poor-grade aneurysmal subarachnoid hemorrhage following microsurgical clipping[J]. Front Neurol, 2023, 14: 1146106. doi: 10.3389/fneur.2023.1146106 [21] Wang LT, Zhang QQ, Zhang GQ, et al. Risk factors and predictive models of poor prognosis and delayed cerebral ischemia in aneurysmal subarachnoid hemorrhage complicated with hydrocephalus[J]. Front Neurol, 2022, 13: 1014501. doi: 10.3389/fneur.2022.1014501 [22] Nadkarni NA, Maas MB, Batra A, et al. Elevated cerebrospinal fluid protein is associated with unfavorable functional outcome in spontaneous subarachnoid hemorrhage[J]. J Stroke Cerebrovasc Dis, 2020, 29(4): 104605. doi: 10.1016/j.jstrokecerebrovasdis.2019.104605 [23] Lai X, Zhang WB, Ye M, et al. Development and validation of a predictive model for the prognosis in aneurysmal subarachnoid hemorrhage[J]. J Clin Lab Anal, 2020, 34(12): e23542. doi: 10.1002/jcla.23542 [24] Hernandez-Garcia L, Aramendía-Vidaurreta V, Bolar DS, et al. Recent technical developments in ASL: a review of the state of the art[J]. Magn Reson Med, 2022, 88(5): 2021-42. doi: 10.1002/mrm.29381 [25] Wang Y, Bartels HM, Nelson LD. A systematic review of ASL perfusion MRI in mild TBI[J]. Neuropsychol Rev, 2023, 33(1): 160-91. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 55
- HTML全文浏览量: 28
- PDF下载量: 6
- 被引次数: 0