



A prognostic model for patients with ischemic cerebral infarction was established based on cerebral MRI perfusion imaging and clinical indicators
-
摘要:
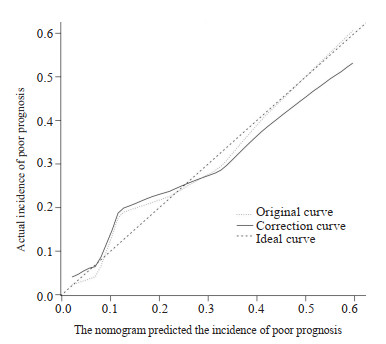
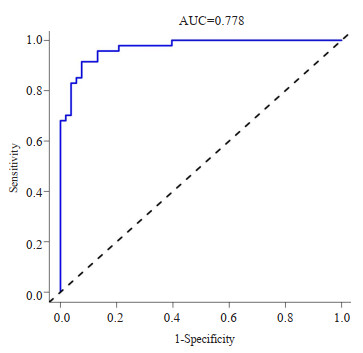
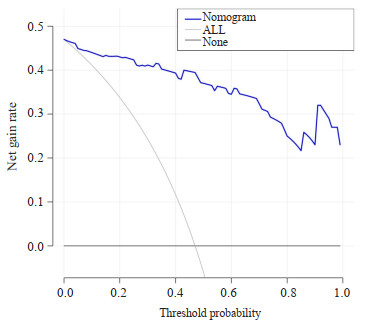
目的 探讨缺血性脑梗死患者预后不良的危险因素,并基于颅脑MRI灌注成像及临床指标构建缺血性脑梗死患者预后不良的列线图模型。 方法 选取2021年7月~2023年1月来我院就诊的100例缺血性脑梗死患者作为研究对象,对患者进行颅脑MRI灌注成像。根据预后情况分为预后不良组(n=47)和预后良好组(n=53)。采用Logistic回归分析筛选缺血性脑梗死患者预后不良的危险因素。采用R4.2.0软件建立缺血性脑梗死患者预后不良的列线图模型,并验证缺血性脑梗死患者预后不良的列线图模型。 结果 Logistic回归分析结果显示,年龄≥60岁、入院时NIHSS评分>12分、大梗死、后循环脑梗死、患侧峰值时间及患侧平均通过时间等是缺血性脑梗死患者预后不良的危险因素,患侧脑血容量及患侧脑血流量是缺血性脑梗死患者预后不良的保护因素(P < 0.05)。构建的缺血性脑梗死患者预后不良的列线图模型的结果显示:校正曲线的实际值与预测值的一致性较好;模型的ROC曲线下面积为0.778(95% CI:0.735~0.821);决策曲线显示阈值概率是1%~100%时,列线图预测缺血性脑梗死患者预后不良的净获益值较高。 结论 基于颅脑MRI灌注成像及临床指标构建的缺血性脑梗死患者预后不良的列线图模型具有较高的准确性及临床应用价值,可以用于缺血性脑梗死患者预后不良的预测。 Abstract:Objective To investigate the risk factors of poor prognosis in patients with ischemic cerebral infarction, and construct a nomogram model of poor prognosis in patients with ischemic cerebral infarction based on cerebral MRI perfusion imaging and clinical indicators. Methods A total of 100 patients with ischemic cerebral infarction who came to our hospital from July 2021 to January 2023 were selected as the study objects, and cerebral MRI perfusion imaging was performed on the patients. According to the prognosis, patients were divided into poor prognosis group (n=47) and good prognosis group (n=53). Logistic regression analysis was used to screen the risk factors of poor prognosis in patients with ischemic cerebral infarction. R4.2.0 software was used to establish and verify the poor prognosis of patients with ischemic cerebral infarction. Results Logistic regression analysis showed that age≥60 years old, NIHSS score>12 points at admission, major infarction, posterior circulation cerebral infarction, affected time to peak and affected mean transit time were risk factors for poor prognosis in patients with ischemic cerebral infarction, and affected cerebral blood volume and affected cerebral blood flow were protective factors for poor prognosis in patients with ischemic cerebral infarction (P < 0.05). The results of the constructed nomogram model for poor prognosis of patients with ischemic cerebral infarction showed that the actual value of the correction curve was in good agreement with the predicted value, the area under ROC curve of the model was 0.778 (95% CI: 0.735-0.821). When the decision curve showed that the threshold probability was 1%-100%, the net benefit value of the histogram predicting the poor prognosis of patients with ischemic cerebral infarction was higher. Conclusion The nomogram model of poor prognosis of patients with ischemic cerebral infarction based on cerebral MRI perfusion imaging and clinical indicators has high accuracy and clinical application value, and can be used to predict poor prognosis of patients with ischemic cerebral infarction. -

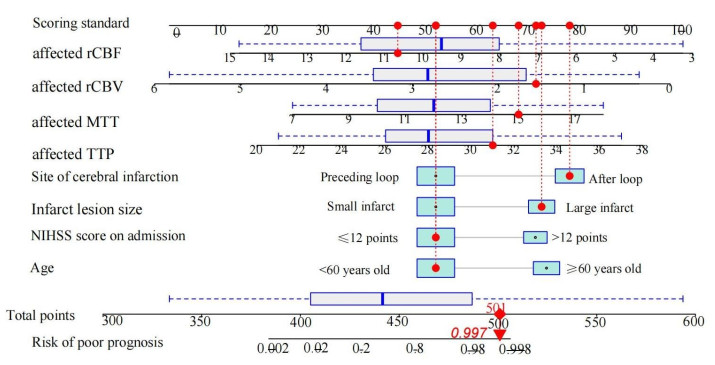
图 1 缺血性脑梗死患者预后不良的列线图
Figure 1. The poor prognosis of patients with ischemic cerebral infarction.
表 1 缺血性脑梗死患者预后不良的单因素分析
Table 1. Univariate analysis of poor prognosis in patients with ischemic cerebral infarction
Item Poor prognosis group
(n=47)Good prognosis group
(n=53)t/χ2 P Gender (n) 0.050 0.822 Male 25 27 Female 22 26 Age (n, years) 13.087 < 0.001 ≥60 24 9 < 60 23 44 NIHSS score on admission (n) 12.240 < 0.001 > 12 21 7 ≤12 26 46 History of cerebral infarction (n) 0.642 0.423 Have 11 9 Not have 36 44 Hypertension (n) 0.290 0.590 Yes 9 8 No 38 45 Coronary heart disease (n) 0.012 0.913 Yes 5 6 No 42 47 Hyperlipemia (n) 0.703 0.402 Yes 7 5 No 40 48 Smoking history (n) 0.321 0.571 Have 12 11 Not have 35 42 Drinking history (n) 0.027 0.869 Have 10 12 Not have 37 41 Infarct lesion size (n) 7.648 0.006 Major infarction 22 11 Small infarct 25 42 Site of cerebral infarction (n) 12.767 < 0.001 After loop 26 11 Preceding loop 21 42 Healthy side TTP (s, Mean±SD) 12.42±1.36 12.61±1.42 0.681 0.497 TTP on the affected side(s, Mean±SD) 29.12±3.67 27.66±3.47 2.044 0.044 Healthy side MTT(s, Mean±SD) 5.62±0.88 5.73±0.94 0.602 0.549 MTT on the affected side(s, Mean±SD) 13.15±2.37 11.12±1.96 4.686 0.000 Healthy side rCBV(mL/100g, Mean±SD) 4.54±0.61 4.47±0.55 0.603 0.548 rCBV on the affected side (mL/100g, Mean±SD) 2.15±1.01 3.24±1.15 5.007 < 0.001 Healthy side rCBF[mL/(100g×min), Mean±SD] 24.28±3.47 24.42±3.63 0.197 0.845 rCBF on the affected side [mL/(100g×min), Mean±SD] 8.34±2.09 10.86±2.14 5.942 < 0.001 NIHSS: National Institute of Health stroke scale; TTP: Time to peak; MTT: Mean transit time; rCBV: Relative cerebral blood volume; rCBF: Regional cerebral blood flow.  下载: 导出CSV
下载: 导出CSV
表 2 变量赋值表
Table 2. Variable assignment table
Variable Assignment mode Prognosis Good prognosis group = "0"; Poor prognosis group = "1" Age < 60 years old = 0; ≥60 years old = "1" NIHSS score on admission ≤12 points = "0"; > 12 points = "1" Infarct lesion size Small infarct = "0"; Large infarct = "1" Site of cerebral infarction Preceding loop = "0"; After loop = "1" TTP on the affected side Bring in original value MTT on the affected side Bring in original value rCBV on the affected side Bring in original value rCBF on the affected side Bring in original value
下载: 导出CSV
表 3 缺血性脑梗死患者预后不良的Logistic回归分析
Table 3. Logistic regression analysis of poor prognosis in patients with ischemic cerebral infarction
Factor β S.E. Wald P OR 95% CI Age 2.189 0.979 4.998 0.025 8.929 1.310-60.857 NIHSS score on admission 1.971 0.995 3.923 0.048 7.177 1.021-50.463 Infarct lesion size 2.094 0.927 5.104 0.024 8.120 1.320-49.954 Site of cerebral infarction 2.649 0.98 7.313 0.007 14.139 2.073-96.437 TTP on the affected side 0.424 0.154 7.577 0.006 1.528 1.130-2.067 MTT on the affected side 0.559 0.240 5.410 0.020 1.749 1.092-2.802 rCBV on the affected side -1.699 0.510 11.104 0.001 0.183 0.067-0.497 rCBF on the affected side -0.762 0.235 10.460 0.001 0.467 0.294-0.741 Constant -9.833 5.179 3.606 0.058 0.000
下载: 导出CSV
-
[1] Tian Y, Su G, Liu JF, et al. Rodent models for intravascular ischemic cerebral infarction: a review of influencing factors and method optimization[J]. NeuroReport, 2020, 31(16): 1154-60. doi: 10.1097/WNR.0000000000001529 [2] Guo ZN, Yang Y, Qu YM, et al. Identification of microRNAs and messenger RNAs involved in human umbilical cord mesenchymal stem cell treatment of ischemic cerebral infarction using integrated bioinformatics analysis[J]. Neural Regen Res, 2019, 14(9): 1610. doi: 10.4103/1673-5374.255998 [3] Qin JC, He Q, Zhang ZJ. Detrimental effect of increased blood pressure variability on clinical outcome in acute ischemic stroke treated with reperfusion therapy: a case control study[J]. BMC Neurol, 2022, 22(1): 87. doi: 10.1186/s12883-022-02605-5 [4] Kusdogan M, Ozturk S. Left ventricular apical mass with normal ejection fraction in a suspected COVID-19 patient suffering from acute ischemic stroke[J]. Anatolian J Cardiol, 2022, 26(3): 232-4. doi: 10.5152/AnatolJCardiol.2021.381 [5] Farag E, Liang C, Mascha EJ, et al. Oxygen saturation and postoperative mortality in patients with acute ischemic stroke treated by endovascular thrombectomy[J]. Anesth Analg, 2022, 134 (2): 369-79. doi: 10.1213/ANE.0000000000005763 [6] 李维民, 刘晓霞, 李娟. 豨蛭络达胶囊联合长春西汀治疗急性期风痰瘀血痹阻脉络型脑梗死的疗效观察及其对血液流变学指标的影响[J]. 中国药物应用与监测, 2022, 19(4): 213-6. https://www.cnki.com.cn/Article/CJFDTOTAL-YWYY202204002.htm [7] Sidhu GDS, Ayoub T, El Hajjar AH, et al. Atrial fibrillation and acute ischemic stroke: evaluation of the contemporary 2018 national inpatient sample database[J]. CJC Open, 2022, 4(6): 513-9. doi: 10.1016/j.cjco.2022.01.010 [8] 何江涛, 王苇, 赵义. 基于CT小肠成像预测中重度期克罗恩病的列线图模型构建[J]. 分子影像学杂志, 2023, 46(1): 63-9. doi: 10.12122/j.issn.1674-4500.2023.01.12 [9] 中华医学会神经病学分会, 中华医学会神经病学分会脑血管病学组, 彭斌, 等. 中国急性缺血性脑卒中诊治指南2018[J]. 中华神经科杂志, 2018, 51(9): 666-82. https://www.cnki.com.cn/Article/CJFDTOTAL-XDJB201911024.htm [10] Schoemaker R, Nayak S, Harnisch LO, et al. Modeling and simulation of the modified Rankin Scale and National Institutes of Health Stroke Scale neurological endpoints in intracerebral hemorrhage [J]. J Pharmacokinet Pharmacodyn, 2019, 46(5): 473-84. doi: 10.1007/s10928-019-09653-4 [11] Mai H, Chen T, Zhao B. Functional outcomes among patients with acute ischemic stroke after mechanical thrombectomy with or without intravenous thrombolysis[J]. JAMA, 2021, 325(19): 2019. doi: 10.1001/jama.2021.4034 [12] Pirson FAV, van Oostenbrugge RJ, van Zwam WH, et al. Repeated endovascular thrombectomy in patients with acute ischemic stroke: results from a nationwide multicenter database[J]. Stroke, 2020, 51 (2): 526-32. doi: 10.1161/STROKEAHA.119.027525 [13] Szmygin M, Sojka M, Tarkowski P, et al. Predictors of favorable outcome after endovascular thrombectomy for acute ischemic stroke due to large vessel occlusion in young patients[J]. Acta Radiol Stock Swed, 2022, 63(12): 1689-94. [14] Hwang J, Lee Y, Kang K, et al. Acute ischemic stroke caused by intracranial atherosclerosis associated with lorlatinib-induced dyslipidemia[J]. J Clin Neurol, 2023, 19(1): 90. doi: 10.3988/jcn.2023.19.1.90 [15] 林存山, 侯倩, 樊青俐, 等. 青海地区急性脑梗死患者2年预后不良的临床特点分析[J]. 心脑血管病防治, 2020, 20(5): 497-9. https://www.cnki.com.cn/Article/CJFDTOTAL-XXFZ202005013.htm [16] Kishi F, Nakagawa I, Park H, et al. Low relative diffusion weighted image signal intensity can predict good prognosis after endovascular thrombectomy in patients with acute ischemic stroke [J]. J Neurointerventional Surg, 2022, 14(6): 618-22. [17] Ling XA, Shen B, Li KZ, et al. Development of a prediction model for 1-year poor prognosis in patients with acute ischemic stroke[J]. J Investig Med, 2019, 67(6): 957-63. doi: 10.1136/jim-2018-000883 [18] 王辉. 血清NSE、IMA及LPA对急性脑梗死患者预后的评估价值[J]. 脑与神经疾病杂志, 2020, 28(2): 91-5. https://www.cnki.com.cn/Article/CJFDTOTAL-LYSJ202002006.htm [19] Joo L, Jung SC, Lee H, et al. Stability of MRI radiomic features according to various imaging parameters in fast scanned T2-FLAIR for acute ischemic stroke patients[J]. Sci Rep, 2021, 11: 17143. doi: 10.1038/s41598-021-96621-z [20] Ma JH, Zhao L, Yuan KM, et al. Crossed cerebellar diaschisis after acute ischemic stroke detected by intravoxel incoherent motion magnetic resonance imaging[J]. Neurol Sci, 2022, 43(2): 1135-41. doi: 10.1007/s10072-021-05425-6 [21] 徐娟, 张立庆, 董伟达, 等. 喉鳞状细胞癌术后患者预后列线图的构建和验证[J]. 临床耳鼻咽喉头颈外科杂志, 2022, 36(12): 902-9. https://www.cnki.com.cn/Article/CJFDTOTAL-LCEH202212003.htm -

 点击查看大图
点击查看大图
计量
- 文章访问数: 48
- HTML全文浏览量: 13
- PDF下载量: 4
- 被引次数: 0