



Multi-mode imaging study and clinical correlation analysis of patients with acute pulmonary thrombus embolism
-
摘要:
目的 探讨急性肺血栓栓塞症(PTE)患者多模态影像学研究结果与临床相关性。 方法 回顾性研究2018年1月~2022年1月首都医科大学附属北京中医医院55例急性PTE确诊患者的超声心动图、二维斑点追踪成像、双下肢血管超声、CT肺动脉造影(CTPA)结果及实验室指标[D-二聚体、脑钠肽(NT-proBNP)、C反应蛋白]。根据CTPA结果,将55例PTE患者分为5级,分析各级D-二聚体、NT-proBNP、C反应蛋白、三尖瓣返流速度(VTR)、肺动脉收缩压(PAPS)及右室游离壁长轴应变(RLS)相关性及变化趋势。 结果 NT-proBNP、VTR及PAPS随CTPA分级增高呈逐渐增高趋势,RLS绝对值随CTPA分级增高呈逐渐降低趋势,各CTPA分级组间差异有统计学意义(P < 0.05)。NT-proBNP、VTR、PAPS及RLS与CTPA分级的偏相关分析结果显示均有相关性(r=0.25、0.24、0.32、0.28,P < 0.05)。 结论 急性PTE患者增高的NT-proBNP、VTR、PAPS及RLS与肺栓塞的严重程度密切相关,对急性PTE患者临床诊治及预后评价具有重要的临床指导价值。 Abstract:Objective To explore the correlation between clinical diagnosis and prognosis in patients with acute pulmonary thrombus embolism (PTE) using multi-mode imaging. Methods Fifty-five patients with PTE confirmed in Beijing Hospital of Traditional Chinese Medicine from January 2018 to January 2022 were evaluated retrospectively. Echocardiography, twodimensional speckle tracking imaging, ultrasound, computer tomography pulmonary angiography (CTPA) and lab marker, including D-dimer, NT-pro brain natriuretic peptide (NT-proBNP) and C-reactive protein results were reviewed. 55 patients with PTE were ranked 5 classes according to CTPA results. Associations and correlations between CTPA classes of D-dimer, NT-proBNP, C-reactive protein, velocity of tricuspid regurgitation (VTR), pulmonary systolic pressure (PAPS) and longitudinal strain in right ventricular free wall (RLS) were analysed. Results NT-proBNP, VTR and PAPS showed a gradually increased trend with increased CTPA class and the absolute value of RLS showed a gradually decreased trend with increased CTPA class. The statistical difference among CTPA grading groups was significant (P < 0.05). Positive correlations were found between increased NT-proBNP, VTR, PAPS, decreased absolute value of RLS with higher CTPA class (r=0.25, 0.24, 0.32, 0.28, P < 0.05). Conclusion Increased NT-proBNP, VTR, PAPS and RLS are significantly associated with the severity of acute PTE patients, which has important clinical value for the diagnosis, treatment and prognosis evaluation of acute PTE patients. -
Key words:
- pulmonary thrombus embolism /
- acute /
- NT-proBNP /
- imaging /
- diagnosis
-

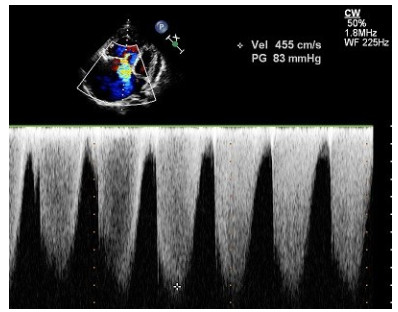
图 1 三尖瓣返流速度的测量
Figure 1. Analysis of tricuspid regurgitation velocity. On adjusted apical four chamber view, tricuspid regurgitation velocity was 455 cm/s, pressure evaluated was 83 mmHg.

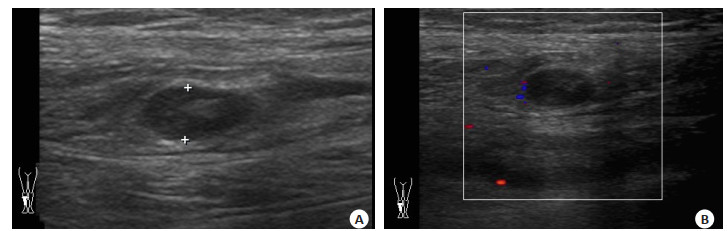
图 2 下肢静脉血栓声像图
Figure 2. DVT in calves. A: Two-dimension ultrasonic imaging; B: Color Doppler imaging.
表 1 PTE临床及实验室指标
Table 1. PTE clinical and lab parameters (Mean±SD)
CTPA classification Age (years) NT-proBNP(ng/L) CRP(mg/L) D-D(mg/L) 1 (n=24) 68±18 55.8±46.2 14.0±14.5 1.3±0.9 2 (n=18) 65±17 242.5±34.5 44.1±33.55 3.4±2.6 3 (n=8) 73±16 294.3±79.8 25.4±24.5 3.2±1.7 4 (n=2) 73±17 304.0±51.1 36.3±13.1 5.7±3.5 5 (n=3) 63±15 746.3±103.2 17.4±10.1 1.0±0.8 CTPA: CT pulmonary angiography; NT-proBNP: NT-pro brain natriuretic peptide; CRP: C reactive protein; D-D: D-dimer.  下载: 导出CSV
下载: 导出CSV
表 2 PTE多模态影像学指标
Table 2. PTE multi-mode imaging parameters (Mean±SD)
CTPA classification DVT(grade) VTR(m/s) PAP(SmmHg) RLS(%) 1 (n=24) 2±1 2.4±0.2 33.8±2.9 -28±3 2 (n=18) 2±2 2.8±0.6 43.7±16.8 -26±4 3 (n=8) 2±1 3.6±0.9 65.0±26.5 -19±3 4 (n=2) 3±1 3.8±0.8 68.1±17.8 -16±5 5 (n=3) 3±1 3.9±0.7 73.2±20.5 -12±3 DVT: Deep venous thrombosis; VTR: Velocity of tricuspid regurgitation; PAPS: Pulmonary arterial systolic pressure; RLS: Longitudinal strain of right ventricular free wall. Cases of McConnell's sign found were as follows: CTPA class 1 group 1 case, class 2 group 3 cases, class 3 group 6 cases, class 4 group 2 cases and class 5 group 3 cases.
下载: 导出CSV
-
[1] 中华医学会呼吸病学分会肺栓塞与肺血管病学组, 中国医师协会呼吸医师分会肺栓塞与肺血管病工作委员会, 全国肺栓塞与肺血管病防治协作组. 肺血栓栓塞症诊治与预防指南[J]. 中华医学杂志, 2018, 98(14): 1060-87. https://www.cnki.com.cn/Article/CJFDTOTAL-ZDLS201901007.htm [2] Otto CM. Textbook of clinical echocardiography. Fourth edition [M]. Philadelphia: Elsevier, 2009: 148-51. [3] Mediratta A, Addetia K, Medvedofsky D, et al. Echocardiographic diagnosis of acute pulmonary embolism in patients with McConnell's sign[J]. Echocardiography, 2016, 33(5): 696-702. doi: 10.1111/echo.13142 [4] Andresen MS, Sandven I, Brunborg C, et al. Mortality and recurrence after treatment of VTE: long term follow-up of patients with good life-expectancy[J]. Thromb Res, 2011, 127(6): 540-6. doi: 10.1016/j.thromres.2011.02.017 [5] Chaix M, Bosson JL, Pernod G. Letter by chaix et al regarding article, "impact of incident venous thromboembolism on risk of arterial thrombotic diseases"[J]. Circulation, 2014, 129(8): 855-63. doi: 10.1161/CIRCULATIONAHA.113.004168 [6] Grob D, Oostveen LJ, Prokop M, et al. Imaging of pulmonary perfusion using subtraction CT angiography is feasible in clinical practice[J]. Eur Radiol, 2019, 29(3): 1408-14. doi: 10.1007/s00330-018-5740-4 [7] Klok FA, van der Bijl N, de Roos A, et al. NT-pro-BNP levels in patients with acute pulmonary embolism are correlated to right but not left ventricular volume and function[J]. Thromb Haemost, 2012, 108(8): 367-72. doi: 10.1160/TH11-12-0901 [8] Wang J, Wang L, Jin L, et al. Predictive value of MPV and plasma NT-ProBNP combined with the simplified Geneva scale for the prognosis of acute pulmonary embolism[J]. Evid Based Complementary Altern Med, 2021, 2021: 1-8. [9] Duma A, Maleczek M, Wagner C, et al. NT-proBNP in young healthy adults undergoing non-cardiac surgery[J]. Clin Biochem, 2021, 96: 38-42. doi: 10.1016/j.clinbiochem.2021.07.009 [10] Carroll BJ, Beyer SE, Mehegan T, et al. Changes in care for acute pulmonary embolism through A multidisciplinary pulmonary embolism response team[J]. Am J Med, 2020, 133(11): 1313-21. e6. doi: 10.1016/j.amjmed.2020.03.058 [11] Taylor DM, Abramson SV, Hawthorne KM, et al. Pulmonary embolus imaging assessment with emphasis on echocardiography[J]. Radiol Technol, 2021, 92(3): 224-31. [12] Bhat V, Lane S, Orde S. Management of straddling thrombus through patent foramen ovale complicating pulmonary embolism [J]. BMJ Case Rep, 2021, 14(4): e240957. doi: 10.1136/bcr-2020-240957 [13] Righini M, Robert-Ebadi H, Le Gal G. Diagnosis of pulmonary embolism[J]. La Presse Médicale, 2015, 44(12): e385-91. doi: 10.1016/j.lpm.2015.10.007 [14] Shah S, Ogbonna AV, Nance J, et al. A multimodality imaging approach to defining risk in patients with acute pulmonary embolism[J]. J Am Soc Echocardiogr, 2023, 36(9): 933-40. doi: 10.1016/j.echo.2023.05.003 [15] 静脉血栓栓塞症抗凝治疗微循环血栓防治共识专家组. 静脉血栓栓塞症抗凝治疗微循环血栓防治专家共识[J]. 中华老年多器官疾病杂志, 2017, 16(4): 241-4. https://www.cnki.com.cn/Article/CJFDTOTAL-XGQW202101004.htm [16] Labropoulos N, Bekelis K, Leon LR. Thrombosis in unusual sites of the lower extremity veins[J]. J Vasc Surg, 2008, 47(5): 1022-7. doi: 10.1016/j.jvs.2007.12.044 [17] Wu Y, Potempa LA, El Kebir D, et al. C-reactive protein and inflammation: conformational changes affect function[J]. Biol Chem, 2015, 396(11): 1181-97. doi: 10.1515/hsz-2015-0149 [18] Saghazadeh A, Hafizi S, Rezaei N. Inflammation in venous thromboembolism: cause or consequence?[J]. Int Immunopharmacol, 2015, 28(1): 655-65. doi: 10.1016/j.intimp.2015.07.044 [19] Mukhopadhyay S, Johnson TA, Duru N, et al. Fibrinolysis and inflammation in venous Thrombus resolution[J]. Front Immunol, 2019, 10: 1348. doi: 10.3389/fimmu.2019.01348 [20] Mazur ES, Mazur VV, Rabinovich RM, et al. Right ventricular longitudinal strain in acute pulmonary embolism and right ventricular myocardial infarction in patients with McConnell's sign [J]. Kardiologiia, 2020, 60(7): 20-7. doi: 10.18087/cardio.2020.7.n1151 [21] Dandel M, Hetzer R. Echocardiographic strain and strain rate imaging-clinical applications[J]. Int J Cardiol, 2009, 132(1): 11-24. doi: 10.1016/j.ijcard.2008.06.091 [22] Peters Andrew C, Shaan MA, Olga K, et al. Temporal trends in right heart strain in patients undergoing pulmonary thromboendarterectomy for chronic thromboembolic pulmonary hypertension[J]. Echocardiogr Mo Kisco N Y, 2021, 38(11): 1932-40. doi: 10.1111/echo.15246 [23] Jenab Y, Saheb Jam M, Safir-Mardanloo A, et al. Strain imaging for evaluating response to thrombolytic therapy in pulmonary thromboembolism[J]. Acta Cardiol, 2014, 69(1): 23-8. doi: 10.1080/AC.69.1.3011341 [24] Park JH, Park YS, Park SJ, et al. Midventricular peak systolic strain and Tei index of the right ventricle correlated with decreased right ventricular systolic function in patients with acute pulmonary thromboembolism[J]. Int J Cardiol, 2008, 125(3): 319-24. doi: 10.1016/j.ijcard.2007.02.030 [25] Kamimura Y, Okumura N, Adachi S, et al. Usefulness of scoring right ventricular function for assessment of prognostic factors in patients with chronic thromboembolic pulmonary hypertension[J]. Heart Vessels, 2018, 33(10): 1220-8. doi: 10.1007/s00380-018-1168-7 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 47
- HTML全文浏览量: 9
- PDF下载量: 6
- 被引次数: 0