



Efficacy of clinical factors-based MRI balanced steady-state free-forward sequence imaging histology for diagnosing extramural vascular invasion in rectal cancer
-
摘要:
目的 探讨基于临床因素结合MRI平衡式稳态自由进动序列(b SSFP)影像组学诊断直肠癌壁外血管(EMVI)的效能。 方法 纳入于同济大学附属东方医院庐江分院术前行MRI检查的135例直肠癌患者,其中71例EMVI阳性,64例EMVI阴性,均经术后病理大标本证实。首先分别从常规T2WI序列、b SSFP序列中提取影像组学特征,按7∶3的比例随机分为训练集(n=94)和验证集(n=41),采用t检验/Wilcoxon秩和检验、最小绝对收缩和选择算子算法、Spearman相关分析和Logistic回归模型分别对影像组学特征及临床特征进行分析,构建影像组学模型,然后绘制ROC曲线,并计算ROC曲线下面积(AUC)、特异性及敏感度,以量化模型对训练组、验证组的鉴别性能,并对比两序列影像组学诊断效能。最后结合临床因素,构建临床因素-b SSFP序列影像影像组学联合模型,进行诊断效能评估,并进行验证。 结果 影像组学模型在训练集和验证集中显示出良好的鉴别能力,其中训练集T2WI序列诊断AUC为0.751,特异性为0.746,敏感度为0.825;b SSFP序列的AUC为0.829,特异性为0.778,敏感度为0.939。验证集T2WI序列影像组学术前诊断AUC为0.676,特异性为0.650,敏感度为0.706;b SSFP序列AUC为0.792,特异性为0.716,敏感度为0.909。后者较前者诊断效能均有所提高,具有一定临床应用价值。临床因素结合b SSFP序列影像组学联合模型训练集AUC为0.954,特异性为0.891,敏感度为0.930;验证集AUC为0.915,特异性为0.803,敏感度为0.936,差异均有统计学意义(P < 0.05)。 结论 基于临床因素结合b SSFP序列影像组学对直肠癌EMVI具有良好的诊断效能,有助于影像科医生和临床医生进行准确的鉴别诊断和制定适当的治疗策略。 -
关键词:
- MRI成像 /
- 影像组学 /
- 平衡式稳态自由进动序列 /
- 直肠癌 /
- 壁外血管
Abstract:Objective To evaluate the effectiveness of combining MRI balanced steady-state free precession (b SSFP) sequence imaging histology based on clinical factors for diagnosing extra-mural vascular invasion (EMVI) in rectal cancer. Methods A total of 135 patients were included in the study whose diagnosed with rectal cancer and treated at the Lujiang Branch of Dongfang Hospital, affiliated with Tongji University. 71 cases were EMVI-positive, and 64 cases were EMVI-negative among the patients, all of which were confirmed by postoperative pathologic macroscopic specimens. Firstly, the imaging histological features were extracted from the conventional T2WI sequences and b SSFP sequences. The dataset was randomly divided into a training set (n=94) and a validation set (n=41) at a ratio of 7∶3. The imaging histological features and clinical features were analyzed, and the imaging histological model were constructed, by the t-test/Wilcoxon rank sum test, and least absolute shrinkage, and selection operator algorithms were utilized for analysis, and Spearman correlation analysis and logistic regression model. Subsequently, ROC curves were plotted, and the area under the ROC curve (AUC), specificity, and sensitivity were calculated. In order to assess and compare the diagnostic efficacy of the two sequential imaging histologies, it was imperative to quantify the discriminatory performance of the model for both the training and validation groups. Subsequently, the clinical factors were integrated to construct a joint clinical factor and b SSFP sequential imaging histology model for the assessment and validation of diagnostic efficacy. Results The imaging histology models displayed strong discriminatory ability in both the training and validation sets. Specifically, the training set of T2WI sequences demonstrated a diagnostic AUC of 0.751, a specificity of 0.746, and a sensitivity of 0.825, while the b SSFP sequences yielded an AUC of 0.829, a specificity of 0.778, and a sensitivity of 0.939. The validation set T2WI sequence imaging group demonstrated a pre-diagnostic AUC of 0.676, a specificity of 0.650, and a sensitivity of 0.706. In contrast, the b SSFP sequence exhibited an AUC of 0.792, a specificity of 0.716, and a sensitivity of 0.909. Comparison between the two indicates the latter's improved diagnostic efficacy and tangible clinical applicability. The combined clinical factors with b SSFP sequence imaging histology joint model exhibited an AUC of 0.954, specificity of 0.891, and sensitivity of 0.930 for the training set. For the validation set, the AUC was 0.915, specificity was 0.803, and sensitivity was 0.936. Both results were deemed statistically significant (P < 0.05). Conclusion The combination of clinical factors and b SSFP sequence imaging histology demonstrates strong diagnostic efficacy for rectal cancer EMVI. This facilitates imaging physicians and clinicians in making accurate differential diagnoses and formulating appropriate treatment strategies. -

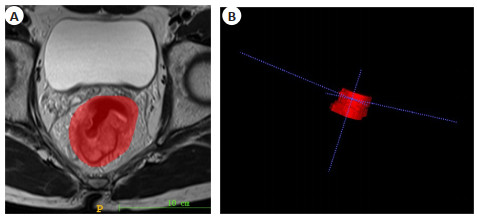
图 1 直肠癌手动三维分割示例
Figure 1. Example of manual 3D segmentation of rectal cancer. A: ROIs were manually outlined along the contours of the lesion; B: 3D volumetric reconstruction of the tumor.

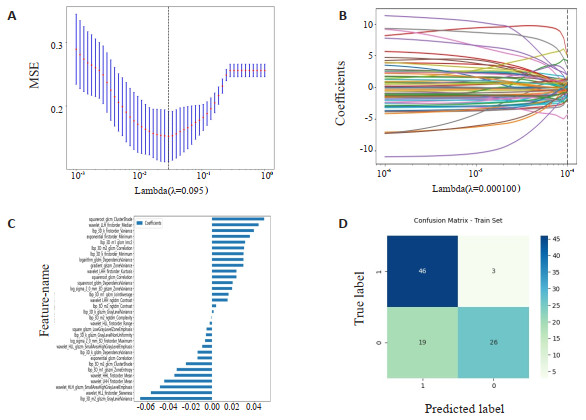
图 2 基于最小惩罚系数λ的b SSFP序列影像组学特征降维和影像组学标签构建图
Figure 2. Imageomics feature degradation and imageomics label construction of b SSFP sequences based on the minimum penalty coefficient λ. A: The Y- axis represents the binomial variance, and the X-axis represents the logarithmic transformation of the feature coefficient and penalty coefficient λ; B: The number of imageomic features constructed changes as the logarithm of λ varies; C: The weight coefficients of each feature when constructing imageomic features based on the minimum penalty coefficient λ; D: The confusion matrix shows true positive and true negative in the upper left and lower right corners, and false positive and false negative in the upper right and lower left corners.

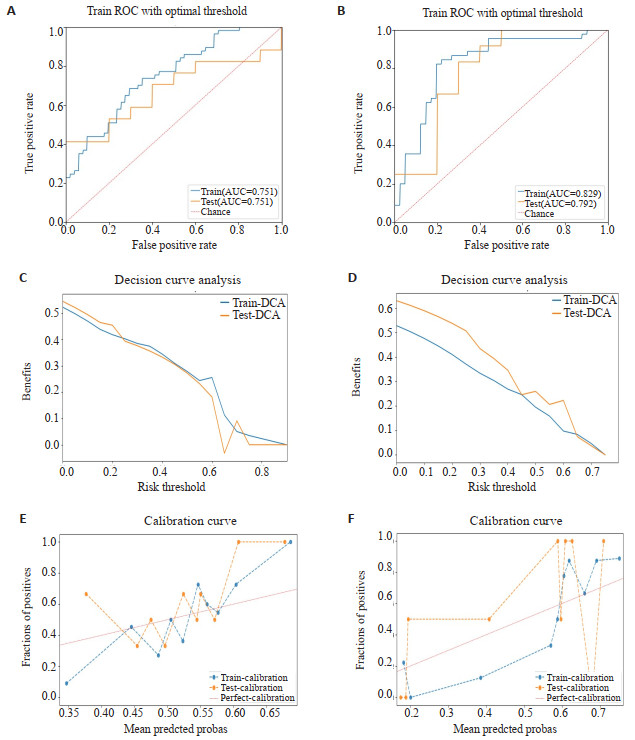
图 3 T2WI与b SSFP序列影像组学诊断效能对比。
Figure 3. Comparative analysis of the diagnostic performance of T2WI and b SSFP sequence imageomics. A: ROC curve of imageomic diagnosis of extramural vascular invasion in rectal cancer for T2WI sequence; B: ROC curve of imageomic diagnosis of extramural vascular invasion in rectal cancer for b SSFP sequence; C: DCA curve of imageomic model for T2WI; D: DCA curve of imageomic model for bSSFP sequence; E: Calibration curve of imageomic model for T2WI; F: Calibration curve of imageomic model for b SSFP sequence.

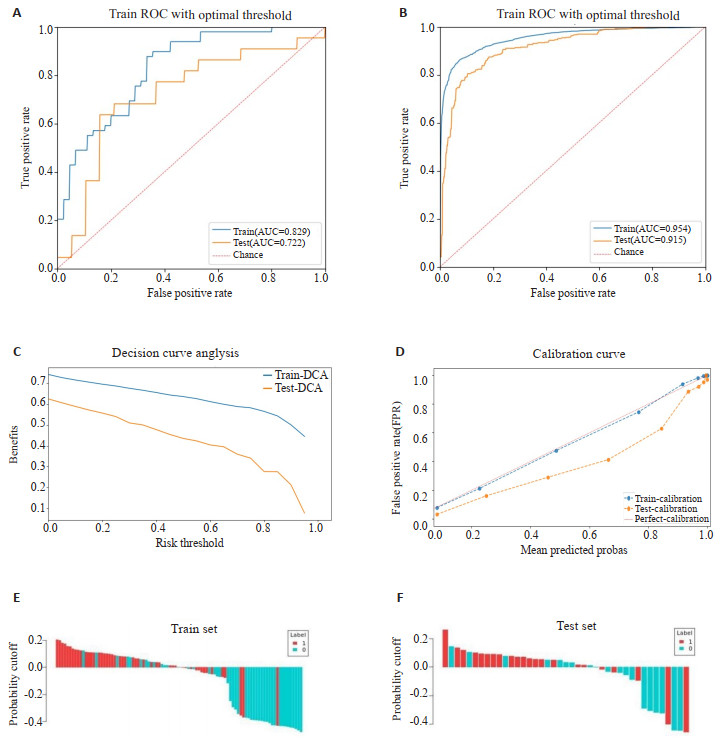
图 4 临床因素-b SSFP序列影像组学联合模型诊断效能。
Figure 4. Diagnostic efficiency of the clinical factor and bSSFP sequence imageomics combined model. A: ROC curve of clinical factor model for diagnosing extramural vascular invasion in rectal cancer; B: ROC curve of clinicalbSSFP sequence imageomics for diagnosing extramural vascular invasion in rectal cancer; C: DCA curve of the combined model; D: Calibration curve of the combined model; E-F: Waterfall plot of the combined model's experimental and validation imageomic model predictions, with samples predicted as negative below the threshold and samples predicted as positive above the threshold.
表 1 135例直肠癌患者的临床资料
Table 1. Clinical data of 135 patients with rectal cancer
Index EMVI(+)(n=71) EMVI(-)(n=64) t/χ2 P Age (year, Mean±SD) 66.85±11.95 69.00±10.61 1.013 0.272 Gender[n(%)] 0.423 0.416 Male 47(66.20) 44(68.75) Female 24(33.80) 20(31.25) T stage[n(%)] 1.017 0.679 cT1 0(0) 7(10.94) cT2 5(7.04) 22(34.38) cT3 42(59.15) 20(31.25) cT4 24(33.81) 15(23.43) CEA (ng/mL, Mean±SD) 27.59±29.69 13.10±17.46 3.407 < 0.001 CA125 (U/mL, Mean±SD) 18.45±21.54 15.27±16.61 0.952 0.343 CA199 (U/mL, Mean±SD) 79.71±236.57 40.44±126.29 1.220 0.225 ADC (×10-3mm2/s, Mean±SD) 0.81±0.14 0.79±0.12 0.282 0.779 Diameter (mm, Mean±SD) 49.96±20.87 42.58±16.14 2.280 0.024 Location [n(%)] 1.180 0.240 Middle upper segment 57(80.28) 54(84.37) Lower segment 14(19.72) 10(15.63)  下载: 导出CSV
下载: 导出CSV
表 2 常规T2WI序列、b SSFP序列影像组学诊断EMVI效能对比
Table 2. Comparative analysis of the diagnostic performance of conventional T2WI sequence and b SSFP sequence imageomics for EMVI
Model Group AUC(95% CI) Specificity Sensitivity P T2WI Train set 0.751(0.724-0.803) 0.746 0.825 < 0.001 Test set 0.676(0.618-0.763) 0.650 0.706 < 0.001 b SSFP Train set 0.829(0.822-0.855) 0.778 0.939 < 0.001 Test set 0.792(0.720-0.802) 0.716 0.909 < 0.001
下载: 导出CSV
表 3 临床因素模型、临床-b SSFP序列影像组学联合模型诊断EMVI效能
Table 3. Diagnostic efficiency of the clinical factor model, clinical & bSSFP sequence imageomics combined model for EMVI
Model Group AUC(95% CI) Specificity Sensitivity P Clinical factors Train set 0.829(0.821-0.871) 0.578 0.939 < 0.001 Test set 0.722(0.643-0.853) 0.316 0.909 < 0.001 Combined test Train set 0.954(0.953-0.954) 0.891 0.930 < 0.001 Test set 0.915(0.902-0.935) 0.883 0.936 < 0.001
下载: 导出CSV
-
[1] Shiraishi T, Ogawa H, Kumasaka S, et al. Comparison of risk factors for locally advanced lower rectal cancer recurrence evaluated by magnetic resonance imaging and pathological factors analysed by longitudinal slicing method[J]. Anticancer Res, 2021, 41(6): 3169-78. doi: 10.21873/anticanres.15103 [2] 徐启兰, 彭传勇, 吴宗山, 等. 高分辨MRI可精准评估直肠癌术前分期及淋巴结转移[J]. 分子影像学杂志, 2022, 45(2): 261-4. doi: 10.12122/j.issn.1674-4500.2022.02.20 [3] Guner OS, Tumay LV. Persistent extramural vascular invasion positivity on magnetic resonance imaging after neoadjuvant chemoradiotherapy predicts poor outcome in rectal cancer[J]. Asian J Surg, 2021, 44(6): 841-7. doi: 10.1016/j.asjsur.2021.01.011 [4] 黄伟康, 卿勇, 刘岘, 等. 探讨直肠腺癌壁外血管侵犯磁共振评分与ADC诊断EMVI的价值[J]. 临床放射学杂志, 2023, 42(7): 1149-53. https://www.cnki.com.cn/Article/CJFDTOTAL-LCFS202307018.htm [5] 王玉娟, 陈勇, 吕茜婷, 等. 3.0T磁共振成像术前诊断直肠癌壁外脉管侵犯的价值及相关因素[J]. 中华肿瘤杂志, 2019, 41(8): 610-4. [6] Lee ES, Kim MJ, Park SC, et al. Magnetic resonance imagingdetected extramural venous invasion in rectal cancer before and after preoperative chemoradiotherapy: diagnostic performance and prognostic significance[J]. Eur Radiol, 2018, 28(2): 496-505. doi: 10.1007/s00330-017-4978-6 [7] Gao F, Shi B, Wang PP, et al. The value of intravoxel incoherent motion diffusion-weighted magnetic resonance imaging combined with texture analysis of evaluating the extramural vascular invasion in rectal adenocarcinoma[J]. Front Oncol, 2022, 12: 813138. doi: 10.3389/fonc.2022.813138 [8] Zhao L, Liang M, Wu PY, et al. A preliminary study of synthetic magnetic resonance imaging in rectal cancer: imaging quality and preoperative assessment[J]. Insights Imaging, 2021, 12(1): 120. doi: 10.1186/s13244-021-01063-w [9] 张景, 靳恒军, 张芳, 等. DWI和T2WI直肠癌体积测量与壁外血管侵犯、淋巴结转移的相关性[J]. 放射学实践, 2020, 35(9): 1151-6. https://www.cnki.com.cn/Article/CJFDTOTAL-FSXS202009022.htm [10] Liu Y, Wei XQ, Feng X, et al. Repeatability of radiomics studies in colorectal cancer: a systematic review[J]. BMC Gastroenteroll, 2023, 23(1): 125. doi: 10.1186/s12876-023-02743-1 [11] 王滔, 陈梅鹃, 张笑, 等. 平衡稳态自由进动序列MRI评估直肠癌周围良、恶性淋巴结[J]. 中国医学影像技术, 2023, 39(3): 389-92. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYXX202303016.htm [12] Tong PF, Sun DQ, Chen GQ, et al. Biparametric magnetic resonance imaging- based radiomics features for prediction of lymphovascular invasion in rectal cancer[J]. BMC Cancer, 2023, 23(1): 61. doi: 10.1186/s12885-023-10534-w [13] Xie F, Zhao Q, Li SQ, et al. Establishment and validation of novel MRI radiomic feature- based prognostic models to predict progression- free survival in locally advanced rectal cancer[J]. Front Oncol, 2022, 12: 901287. doi: 10.3389/fonc.2022.901287 [14] Hou M, Zhou L, Sun JH. Deep-learning-based 3D super-resolution MRI radiomics model: superior predictive performance in preoperative T-staging of rectal cancer[J]. Eur Radiol, 2023, 33(1): 1-10. [15] 中国医师协会结直肠肿瘤专业委员会诊疗技术专委会, 中华医学会放射学分会腹部学组. 直肠癌MR扫描及结构式报告规范专家共识[J]. 中华放射学杂志, 2021, 55(11): 1121-7. [16] Liu H, Zhang C, Wang L, 等. MRI影像组学分析对直肠癌病人术前同期远处转移的预测[J]. 国际医学放射学杂志, 2019, 42(5): 631-2. https://www.cnki.com.cn/Article/CJFDTOTAL-GWLC201905101.htm [17] 秦思源, 陆思懿, 王奇政, 等. 不同MRI影像组学方法预测直肠癌新辅助治疗病理完全缓解的价值比较[J]. 磁共振成像, 2022, 13(11): 82-7, 114. https://www.cnki.com.cn/Article/CJFDTOTAL-CGZC202211015.htm [18] Chen QL, Cui YF, Xue T, et al. Computed tomography-based radiomics nomogram for the preoperative prediction of perineural invasion in colorectal cancer: a multicentre study[J]. Abdom Radiol (NY), 2022, 47(9): 3251-63. doi: 10.1007/s00261-022-03620-3 [19] 梁翠珊, 黄燕琪, 何兰, 等. 基于影像组学方法术前预测结直肠癌淋巴血管侵犯[J]. 中国医学影像学杂志, 2018, 26(3): 191-6, 201. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYYZ201803010.htm [20] 王滔, 陈梅鹃, 李娜, 等. MRI三维平衡式稳态自由进动序列在评估直肠癌壁外血管侵犯中的价值[J]. 实用放射学杂志, 2022, 38(4): 586-9. [21] 黄雨, 柴学, 肖朝勇, 等. 三维双激发平衡式稳态自由进动序列和三维时间飞跃MRA序列在原发性三叉神经痛中的诊断价值[J]. 临床神经病学杂志, 2020, 33(5): 362-6. https://www.cnki.com.cn/Article/CJFDTOTAL-LCSJ202005015.htm [22] Pat G, Jun Y, Levi P, et al. Threshold change in CEA as a predictor of non- progression to first- line systemic therapy in metastatic colorectal cancer patients with elevated CEA[J]. J Natl Cancer Inst, 2020, 112(11): 1127-36. doi: 10.1093/jnci/djaa020 [23] Khalyfa A, Randhawa N, Khan M, et al. S1979 De novo association between gastrin and CEA in colorectal cancer[J]. Am J Gastroenterol, 2022, 117(10S): e1363. [24] Gawiński C, Hołdakowska A, Wyrwicz L. Correlation between lymphocyte- to- monocyte ratio (LMR), neutrophil- to- lymphocyte ratio (NLR), platelet- to- lymphocyte ratio (PLR) and extramural vascular invasion (EMVI) in locally advanced rectal cancer[J]. Curr Oncol, 2022, 30(1): 545-58. doi: 10.3390/curroncol30010043 [25] Zou M, Yang ZQ, Gao F. Letter to the editor "Extramural venous invasion (EMVI) in colorectal cancer is associated with increased cancer recurrence and cancer-related death"[J]. Eur J Surg Oncol, 2023, 49(1): 298-9. doi: 10.1016/j.ejso.2022.08.010 [26] 柯钧文, 卢振东, 陈武标. 基于MR影像组学列线图在直肠癌壁外血管侵犯中的研究进展[J]. 分子影像学杂志, 2023, 46(5): 948-52. doi: 10.12122/j.issn.1674-4500.2023.05.32 [27] 王可欣, 余静, 徐青. 基于RESOLVE ADC的影像组学列线图在预测直肠癌壁外血管侵犯中的应用价值[J]. 肿瘤影像学, 2023, 32(2): 138-47. https://www.cnki.com.cn/Article/CJFDTOTAL-YXYX202302006.htm -

 点击查看大图
点击查看大图
计量
- 文章访问数: 59
- HTML全文浏览量: 22
- PDF下载量: 4
- 被引次数: 0