



Clinical characteristics of children with family clusters of SARS-CoV-2 Omicron variant infection in Guangzhou in 2022
-
摘要:
目的 探讨家庭聚集性儿童新型冠状病毒Omicron变异株感染的临床特征及影像学变化。 方法 将2022年10~12月在广东省第二人民医院收治的241例6岁以下确诊为新型冠状病毒Omicron变异株感染的儿童作为研究对象, 根据感染年龄分为3组: 0~1岁(n=76), 1~3岁(n=80), 3~6岁(n=85)。比较3组患儿的临床特征、实验室检查结果、疫苗接种史、影像学检查结果及转归。 结果 241例患儿中, 轻型203例(84.2%), 重型38例(15.8%), 无中型及危重型。发热为主要症状(97.5%), 其次是咳嗽(54.4%)、腹泻(29.9%)、鼻塞或流涕(25.7%)、惊厥(15.4%)。3~6岁的发热热程最低, 核酸转阴时间最短, 容易出现上呼吸道症状; 0~1岁的发热热峰最低, 以咳嗽、腹泻及皮疹为主要症状。0~1岁婴儿较年长儿容易出现肺炎性状的影像学表型, X线可表现为双肺野见斑片状和或云雾状阴影; 胸部CT可表现为双肺纹理增粗, 肺野通亮度减低, 见条状和或片状高密度影, 边界模糊。1~3岁重型发生率最高(22.5%), 较0~1岁更容易发生惊厥。与轻型相比, 重型的SARS-CoV-2 N基因循环阈值更低, 更容易出现淋巴细胞计数减少、中性粒细胞与淋巴细胞计数比值升高及血清淀粉样蛋白A升高。在3~6岁患儿中, 与接种0剂或1剂疫苗者相比, 接种2剂疫苗的患儿发热热程超过2 d的风险更低(OR=0.373, 95%CI: 0.152~0.912, P=0.029), 发生腹泻的风险降低(OR=0.298, 95%CI: 0.096~0.922, P=0.030), 核酸转阴时间更短(OR=0.359, 95%CI: 0.149~0.867, P=0.021), 重型的发生率降低17.3%(OR=0.237, 95%CI: 0.061~0.922, P=0.040)。 结论 家庭聚集性Omicron变异株感染儿童以发热、咳嗽为主要症状, 胸部CT可呈现肺部炎性改变。1~3岁儿童较0~1岁更容易发生惊厥。中性粒细胞与淋巴细胞计数比值和血清淀粉样蛋白A有助于预测感染的严重程度。疫苗接种可降低3~6岁儿童发生重型的风险, 降低病毒载量, 减少核酸阳性持续时间。 -
关键词:
- 新型冠状病毒 /
- Omicron变异株 /
- 家庭聚集性 /
- 儿童 /
- 临床特征
Abstract:Objective To investigate the clinical characteristics and chest CT or X-ray features of family-clustered children infected with the Omicron variant of severe acute respiratory syndrome coronavirus 2(SARS-CoV-2). Methods A retrospective analysis was performed on the medical data of 241 children with SARS-CoV-2 Omicron variant infection who were admitted to Guangdong Second Provincial General Hospital, the designated hospital for COVID-19 from October 2022 to December 2022.The children were divided into 76 cases of 0-1 year, 80 cases of 1-3 years old and 85 cases of 3-6 years old according to the age of infection.The clinical characteristics, results of laboratory examination, chest CT or X-ray findings and outcome of the three groups were compared. Results Among 241 children, 203 cases (84.2%) were mild, 38 cases (15.8%) were severe, no moderate or critical.Fever was the most common symptom (97.5%), followed by cough (54.4%), diarrhea (29.9%), nasal congestion and/or runny nose (25.7%), and convulsion (15.4%).Children aged 3-6 years old were prone to upper respiratory symptoms, with the lowest fever duration and the shortest nucleic acid negative conversion time.Children aged 0-1 year mainly showed symptoms of cough, diarrhea and rash, with the lowest peak of fever.Infants aged 0-1 year were more likely to present radiological phenotype of pneumonia than older children.X-rays showed patchy and/or cloudy shadows in both lung fields, while chest CT showed thickened lung texture, decreased transparency of lung fields, and linear or patchy high-density shadows with blurred boundaries.Children aged 1-3 years old had the highest incidence of severe COVID-19 infection (22.5%), and they were more likely to have convulsions than those aged 0-1 year.Compared with mild cases, severe cases had lower cycle threshold value of SARS-CoV-2 N gene, lower lymphocyte count, higher neutrophil-to-lymphocyte ratio and higher serum amyloid A level.Among children aged 3-6 years, compared with those who received 0 or 1 dose of the vaccine, children who received 2 doses of the vaccine had a lower risk of fever lasting more than 2 d (OR=0.373, 95%CI: 0.152-0.912, P=0.029), a lower risk of diarrhea (OR=0.298, 95% CI: 0.096-0.922, P=0.030), a shorter time for nucleic acid negative conversion (OR=0.359, 95% CI: 0.149-0.867, P=0.021), and a lower incidence of severe cases (OR=0.237, 95%CI: 0.061-0.922, P=0.040). Conclusion Fever and cough are the main symptoms of children with family clustering SARS-CoV-2 Omicron variant infection, and chest CT can show pulmonary inflammatory changes.Children aged 1-3 years old are more likely to have convulsions than those aged 0-1 year.The neutrophil-to-lymphocyte ratio and serum amyloid A levels are helpful in predicting the severity of infection.Vaccination can reduce the risk of severe infection in children aged 3-6 years, decrease the viral load and shorten nucleic acid negative conversion time. -
Key words:
- COVID-19 /
- Omicron variant /
- family cluster infection /
- child /
- clinical feature
-

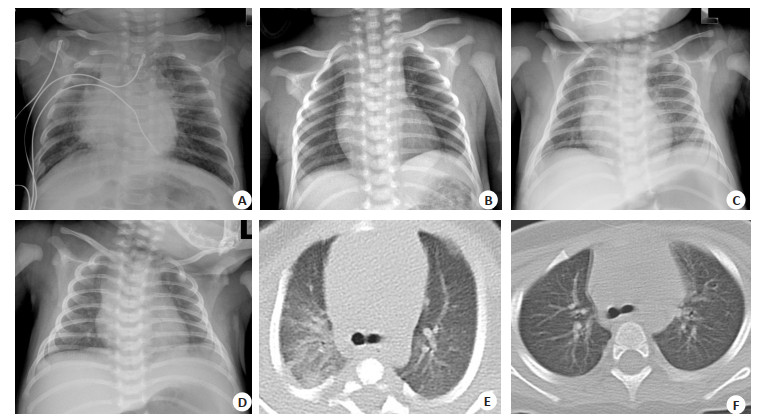
图 1 Omicron变异株感染患者治疗前及治疗后影像学结果
Figure 1. Imaging results of patients with Omicron variant infection before and after treatment. A, C, E: The characteristics of chest X-ray or chest CT before treatment; B, D, F: The characteristics of chest X-ray or chest CT after treatment.
表 1 不同年龄组奥密克戎变异株感染患儿的临床特征
Table 1. Clinical characteristics of children infected with SARS-CoV-2 Omicron variant in different age groups
Index All patients
(n=241)0-1 year old
(n=76)1-3 years old
(n=80)3-6 years old
(n=85)χ2/H/F/Fisher P Gender[n(%)] 0.498 0.779 Male 138(57.3) 41(53.9) 47(58.7) 50(58.8) Female 103(42.7) 35(46.1) 33(41.3) 35(41.2) Time of diagnosis [d, M(P25, P75)] 2.0(1.0, 3.0) 2.0(1.0, 2.75) 2.0(1.0, 3.0) 2.0(1.0, 3.0) 1.711 0.425 Nuclecapsid Protein gene [M(P25, P75)] 29.53(26.21, 31.96) 29.66(25.52, 31.48) 29.08(25.08, 31.06) 30.41(27.25, 33.14)ab 6.021 0.045 ORFla gene (Mean±SD) 29.59 ± 3.67 29.17 ± 3.46 29.38 ± 3.68 30.17 ± 3.80 1.715 0.182 Time of nucleic acid negative conversion [d, M(P25, P75)] 6.0(5.0, 7.0) 6.0(5.0, 7.0) 6.0(5.0, 8.0) 5.0(4.0, 7.0)ab 14.750 < 0.001 Time of hospitalization [d, M(P25, P75)] 6.0(8.0, 11.5) 6.0(9.0, 12.0) 6.0(8.0, 12.0) 8.0(7.0, 10.5) 0.091 0.956 Clinical classification [n(%)] 6.309 0.043 Mild group 203(84.2) 70(92.1) 62(77.5)a 71(83.5) Severe group 38(15.8) 6(7.9) 18(22.5)a 14(16.5) Symptoms Fever [n(%)] 235(97.5) 74(97.4) 79(98.8) 82(96.5) 0.948 0.781 Fever peak [℃, M(P25, P75)] 39.0(38.6, 40.0) 39.0(38.5, 39.93) 39.5(38.9, 40.0)a 39.0(38.6, 39.8) 7.964 0.019 Time of fever [d, M(P25, P75)] 2.0(3.0, 3.0) 2.0(3.0, 3.0) 2.0(3.0, 3.0) 2.0(3.0, 3.0)ab 12.053 0.002 Convulsive seizure [n(%)] 37(15.4) 5(6.6) 18(22.5)a 14(16.5) 7.728 0.021 Cough [n(%)] 131(54.4) 45(59.2) 34(42.5 52(61.2)b 6.848 0.033 Hoarseness/sore throat [n(%)] 31(12.9) 1(1.3) 9(11.9)a 21(24.7)a 21.434 < 0.001 Snivel [n(%)] 62(25.7) 25(32.9) 20(25.0) 17(20.0) 3.525 0.172 Diarrhea [n(%)] 72(29.9) 31(40.8) 24(30.0) 17(20.0)a 8.279 0.016 Vomiting [n(%)] 23(9.5) 7(9.2) 11(13.8) 5(5.9) 2.969 0.227 Rash attack [n(%)] 29(12.0) 16(21.1) 8(10.0) 5(5.9)b 9.191 0.010 aP < 0.05 vs 0-1 year old;bP < 0.05 vs 1-3 years old.  下载: 导出CSV
下载: 导出CSV
表 2 奥密克戎变异株感染患者轻重型的单因素分析
Table 2. Single factor analysis of the severity of patients infected with the Omicron variant
Clinical information Mild group (n=203) Severe group (n=38) χ2/t/Z/Fisher P Gender [n(%)] 0.007 0.931 Male 116(57.1) 22(57.9) Female 87(42.9) 16(42.1) Nuclecapsid protein gene (Mean±SD) 29.31 ± 3.95 27.66 ± 4.12 2.338 0.020 ORFla gene [M(P25, P75)] 30.26(27.33, 32.44) 28.37(24.98, 30.91) -2.409 0.016 Laboratory examination White blood cell count [×109/L, M(P25, P75)] 6.65(5.08, 8.39) 6.07(4.88, 8.55) -0.671 0.502 Lymphocyte count [×109/L, M(P25, P75)] 2.53(1.64, 4.12) 1.51(0.88, 2.52) -3.896 < 0.001 Lymphocyte percentage [%, M(P25, P75)] 46.1(29.0, 61.2) 31.0(18.9, 41.1) -3.390 < 0.001 Neutrophil count [×109/L, M(P25, P75)] 2.31(1.35, 3.80) 3.35(2.30, 5.93) -2.651 0.008 Neutrophil percentage [%, M(P25, P75)] 36.5(25.0, 55.1) 56.1(42.8, 70.2) -3.724 < 0.001 Lymphocytopenia [ < 1×109/L, n(%)] 9(7.5) 10(31.3) 13.029 < 0.001 Neutropenia [ < 1.5×109/L, n(%)] 33(27.5) 4(12.5) - 0.105 Neutrophil-lymphocyte ratio [M(P25, P75)] 0.82(0.40, 1.87) 1.92(1.04, 4.36) -3.941 < 0.001 Platelet count [×109/L, M(P25, P75)] 247.5(201.3, 314.8) 229.5(190.3, 279.5) -1.652 0.099 Hypersensitive C-reactive protein [mg/L, M(P25, P75)] 1.48(0.80, 7.00) 2.46(0.83, 6.22) -0.525 0.599 Serum amyloid A [mg/L, M(P25, P75)] 16.80(4.80, 45.80) 70.64(25.04, 133.82) -3.447 < 0.001 Vaccination [n(%)] - 0.156 0 or 1 dose 165(81.3) 35(92.1) 2 doses 38(18.7) 3(7.9)
下载: 导出CSV
表 3 疫苗接种对3~6岁奥密克戎变异株感染患儿临床特征及转归的影响
Table 3. Effects of vaccination on clinical characteristics and outcomes of children aged 3-6 years old with Omicron variant infection [n(%)]
Index 0 or 1 dose(n=44) 2 doses (n=41) OR(95% CI) χ2/Fisher P Clinical classification 0.237(0.061-0.922) - Mild group 33(75.0) 38(92.7) Severe group 11(25.0) 3(7.3) Nucleic acid negative conversion ≤5 d 18(40.9) 27(65.9) 0.359(0.149-0.867) 5.301 0.021 Time of hospitalization ≤7 d 19(43.2) 14(34.1) 1.466(0.609-3.530) 0.730 0.393 Fever 44(100.0) 38(92.7) - - 0.108 Time of fever ≤2 d 16(36.4) 23(60.5) 0.373(0.152-0.912) 4.773 0.029 Cough 26(59.1) 26(63.4) 1.200(0.500-2.878) 0.167 0.683 Diarrhea 14(31.8) 5(12.2) 0.298(0.096-0.922) 4.709 0.030
下载: 导出CSV
-
[1] Zhang XT, Wu SJ, Wu BL, et al. SARS-CoV-2 Omicron strain exhibits potent capabilities for immune evasion and viral entrance[J]. Signal Transduct Target Ther, 2021, 6(1): 430. doi: 10.1038/s41392-021-00852-5 [2] Ao YY, Li JJ, Wei ZQ, et al. Clinical and virological characteristics of SARS-CoV-2 Omicron BA. 2.2 variant outbreaks during April to May, 2022, Shanghai, China[J]. J Infect, 2022, 85(5): 573-607. [3] 卞相丽, 国志, 张坤, 等. 上海380例家庭聚集性感染Omicron变异株的儿童及其家属临床特征分析[J]. 中国当代儿科杂志, 2022, 24(10): 1085-91. doi: 10.7499/j.issn.1008-8830.2205179 [4] Wang L, Berger NA, Kaelber DC, et al. Incidence rates and clinical outcomes of SARS-CoV-2 infection with the Omicron and delta variants in children younger than 5 years in the US[J]. JAMA Pediatr, 2022, 176(8): 811-3. doi: 10.1001/jamapediatrics.2022.0945 [5] Paul LA, Daneman N, Schwartz KL, et al. Association of age and pediatric household transmission of SARS-CoV-2 infection[J]. JAMA Pediatr, 2021, 175(11): 1151-8. doi: 10.1001/jamapediatrics.2021.2770 [6] Khan FL, Nguyen JL, Singh TG, et al. Estimated BNT162b2 vaccine effectiveness against infection with delta and Omicron variants among US children 5 to 11 years of age[J]. JAMA Netw Open, 2022, 5(12). [7] 李宇, 张哲, 杜溪乔, 等. 新冠病毒变异株奥密克戎的变异特点及对免疫学特性的影响[J]. 国际免疫学杂志, 2022, 45(1): 1-4. [8] Price AM, Olson SM, Newhams MM, et al. BNT162b2 protection against the Omicron variant in children and adolescents[J]. N Engl J Med, 2022, 386(20): 1899-909. doi: 10.1056/NEJMoa2202826 [9] 中华人民共和国国家卫生健康委员会. 新型冠状病毒感染诊疗方案(试行第十版)[J]. 中华临床感染病杂志, 2023, 16(1): 1-9. https://www.cnki.com.cn/Article/CJFDTOTAL-JZYL202304001.htm [10] Wang ZL, Ma WL, Zheng X, et al. Household transmission of SARS-CoV-2[J]. J Infect, 2020, 81(1): 179-82. doi: 10.1016/j.jinf.2020.03.040 [11] 中国国家卫生健康委员会. 新型冠状病毒肺炎诊疗方案(试行第九版)[J]. 国际流行病学传染病学杂志, 2022, 49(2): 73-80. https://www.cnki.com.cn/Article/CJFDTOTAL-GAYX202307005.htm [12] 何洋, 唐军, 张萌, 等. 儿童COVID-19的临床特征: 一项关于SARS、MERS及COVID-19的系统评价[J]. 中国当代儿科杂志, 2020, 22(8): 844-53. https://www.cnki.com.cn/Article/CJFDTOTAL-DDKZ202008008.htm [13] Wang JY, Li TN, Zhou CL, et al. Clinical and immunological features of convalescent pediatric patients infected with the SARS-CoV-2 Omicron variant in Tianjin, China[J]. Virol Sin, 2022, 37(6): 850-9. doi: 10.1016/j.virs.2022.10.009 [14] Shen N, Wu YF, Chen YW, et al. Clinical characteristics of pediatric cases infected with the SARS-CoV-2 Omicron variant in a tertiary children's medical center in Shanghai, China[J]. World J Pediatr, 2023, 19(1): 87-95. doi: 10.1007/s12519-022-00621-6 [15] 祁正红, 贝泽锋, 滕淑, 等. 杭州市19例新型冠状病毒Omicron变异株感染儿童的临床特征[J]. 中国当代儿科杂志, 2022, 24(10): 1092-7. doi: 10.7499/j.issn.1008-8830.2205122 [16] Pulliam JRC, van Schalkwyk C, Govender N, et al. Increased risk of SARS-CoV-2 reinfection associated with emergence of Omicron in South Africa[J]. Science, 2022, 376(6593): 4947. [17] Lu XX, Zhang LQ, Du H, et al. SARS-CoV-2 infection in children[J]. N Engl J Med, 2020, 382(17): 1663-5. [18] 徐晶, 孔祥莓, 万思贝, 等. 2022年上海疫情期间312例儿童新型冠状病毒肺炎感染者早期临床特征分析[J]. 中国小儿急救医学, 2022, 29(10): 784-9. [19] Brandal LT, MacDonald E, Veneti L, et al. Outbreak caused by the SARS-CoV-2 Omicron variant in Norway, November to December 2021[J]. Euro Surveill, 2021, 26(50): 2101147. [20] 陈如平, 包剑锋, 许远, 等. Omicron变异株感染的新型冠状病毒肺炎患儿临床特征分析[J]. 中华临床感染病杂志, 2022, 15(3): 200-6. https://www.cnki.com.cn/Article/CJFDTOTAL-DDKZ202207004.htm [21] 宁会彬, 李贵珍, 翟文化, 等. 129例新型冠状病毒肺炎患者的血常规特点及其变化与临床分型的关系分析[J]. 上海预防医学, 2020, 32(12): 1016-20. https://www.cnki.com.cn/Article/CJFDTOTAL-SHYI202012011.htm [22] Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China[J]. Lancet, 2020, 395(10223): 497-506. [23] He SJ, Fang YH, Yang J, et al. Association between immunity and viral shedding duration in non-severe SARS-CoV-2 Omicron variant-infected patients[J]. Front Public Health, 2022, 10: 1032957. [24] Liu Q, Dai YP, Feng M, et al. Associations between serum amyloid A, interleukin-6, and COVID‐19: a cross-sectional study[J]. J Clin Lab Anal, 2020, 34(10): e23527. [25] Qin RD, He L, Yang ZW, et al. Identification of parameters representative of immune dysfunction in patients with severe and fatal COVID-19 infection: a systematic review and meta-analysis[J]. Clin Rev Allergy Immunol, 2023, 64(1): 33-65. [26] 王雪琳, 翟嘉, 邹映雪. 新型冠状病毒Omicron变异株感染患儿的临床特征及免疫效应分析[J]. 中华儿科杂志, 2022, 60(7): 671-5. [27] Li MS, Liu QQ, Wu D, et al. Association of COVID-19 vaccination and clinical severity of patients infected with delta or Omicron variants-China, may 21, 2021-February 28, 2022[J]. China CDC Wkly, 2022, 4(14): 293-7. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 55
- HTML全文浏览量: 39
- PDF下载量: 2
- 被引次数: 0