



Quantitative myocardial contrast echocardiography can evaluate degree of coronary artery stenosis
-
摘要:
目的 探讨超声造影定量分析与冠状动脉狭窄程度的相关性,评价其对冠心病狭窄程度的预测价值。 方法 连续性纳入我院门诊怀疑冠心病的患者35例,接受心肌声学造影检查后行冠状动脉造影和/或冠状动脉CT血管成像,按冠状动脉造影和/或冠状动脉CT血管成像结果将其分为冠心病组(冠脉狭窄≥75%,n=20)和对照组(冠脉狭窄<75%,n=15),比较两组的临床指标和二维超声;另按冠脉支数测量超声造影定量参数,绘制ROC曲线评价造影参数预测冠状动脉狭窄≥75%的敏感度和特异性。 结果 与对照组相比,冠心组高血压、吸烟史比率更高(50.00% vs 13.33 %、65.00% vs 26.67%,P<0.05),二维超声提示节段性室壁运动异常发生率高(90.00% vs 46.67%,P<0.05)。超声造影结果示,两组间心肌峰值强度、曲线下面积的差异均有统计学意义(P<0.001)。ROC曲线分析显示,心肌峰值强度、曲线下面积预测冠脉狭窄程度≥75%的预警值为5.91 dB(敏感度、特异性分别为97.8%、95.2%)和28.94 dB sec(敏感度、特异性分别为66.7%、74.8%)。 结论 超声造影定量分析无创、简便,适合长期随访,可较为准确地评估心肌缺血,有助于临床判断冠脉狭窄程度和指导后续治疗。 -
关键词:
- 冠心病 /
- 心肌声学造影 /
- 冠脉造影 /
- 冠状动脉CT血管成像
Abstract:Objective To explore the correlation between quantitative myocardial contrast echocardiography (MCE) and the degree of coronary artery stenosis, and evaluate its predictive value on the the degree of coronary artery stenosis. Methods A total of 35 patients with suspected coronary heart disease were continuously enrolled in our hospital. All patients underwent MCE, coronary angiography and/or coronary CT angiography. According to coronary angiography and/or coronary CT angiography results, the patients were divided into two groups: coronary artery disease group (coronary artery stenosis ≥75%, n=20) and control group (coronary artery stenosis <75%, n=15). Clinical indicators and two-dimensional ultrasound were compared between two groups. In addition, quantitative parameters of MCE were measured according to the number of coronary arteries, and ROC curve evaluate the sensitivity and specificity of MCE parameters in predicting coronary artery stenosis ≥75%. Results The proportion of hypertension and smoking history were higher in the coronary group than that in the control group (50.00% vs 13.33%, 65.00% vs 26.67%, P<0.05), and two-dimensional ultrasound showed a high incidence of segmental wall motion abnormalities (90.00% vs 46.67%, P<0.05). Contrast-enhanced ultrasound showed that there were significant differences in peak myocardial intensity and area under the curve between the two groups (P<0.001). ROC curve analysis showed that peak myocardial intensity and area under the curve had a predictive value of 5.91 dB (sensitivity and specificity were 97.8% and 95.2%) and 28.94 dB sec (sensitivity and specificity were 66.7% and 74.8%) in predicting the degree of coronary artery stenosis ≥75%. Conclusion Contrast-enhanced ultrasound quantitative analysis is non-invasive, simple and suitable for long-term follow-up. It can accurately evaluate myocardial ischemia and is helpful for clinical judgement coronary artery stenosis degree and guidance for subsequent treatment. -

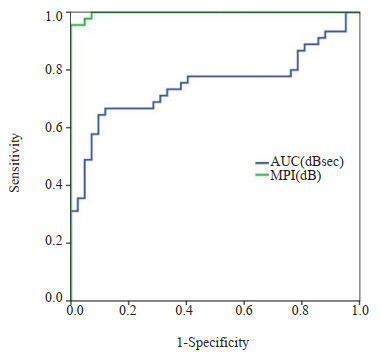
图 1 冠心组(A~C)、对照组(D~F)MCE造影、定量分析及CTA图
Figure 1. MCE imaging, quantitative analysis and CTA of coronary group (A-C) and control group (D-F). A: MCE showed normal posterior septal perfusion; B: The perfusion was acceptable by contrast quantitative curve (AUC 57.09 dB sec, MPI 10.12 dB); C: CTA confirmed that RCA stenosis was mild (25%-49%); D: MCE showed significantly reduced posterior wall perfusion; E: Reduced perfusion was evaluated by contrast quantitative curve (AUC 24.17 dB sec, MPI 4.26 dB); F: CTA confirmed that LCX stenosis was severe (75%-99%). MCE: Myocardial contrast echocardiography; RCA: Right coronary artery; LCX: Left circumflex branch.

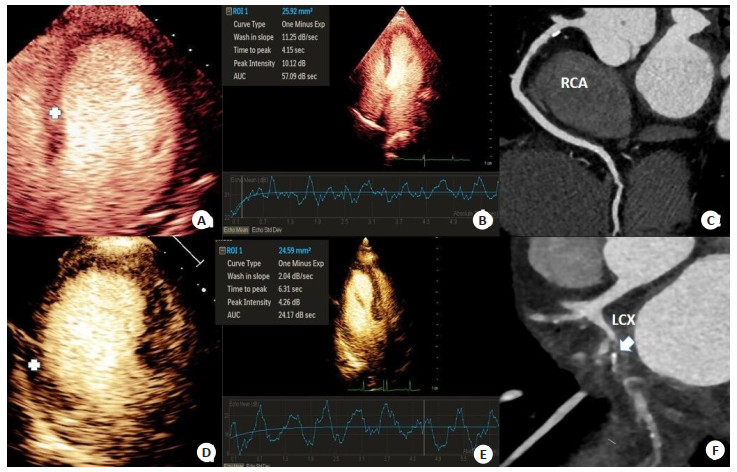
图 2 造影参数MPI、AUC预测冠脉狭窄程度≥75%的ROC曲线
Figure 2. ROC curve of MPI and AUC predicting coronary stenosis ≥75%.
表 1 两组人群的一般资料及二维超声特征比较
Table 1. Comparison of general data and two-dimensional ultrasonic characteristics between the two groups (Mean±SD)
Index Control group(n=15) Coronary artery disease group(n=20) χ2/t P General data Age (year) 49.7±13.4 60.0±11.4 -2.45 0.020 Gender [Male, n(%)] 9(60.00) 18(90.00) 4.37 0.036 Height(m) 1.68±0.07 1.69±0.07 -0.38 0.709 Weight(kg) 68.07±9.38 71.70±8.41 -1.21 0.237 BMI (kg/m2) 23.97±2.96 25.06±3.14 -1.04 0.305 Smoke [Yes, n(%)] 4(26.67) 13(65.00) 5.04 0.025 Blood glucos(mmol/L) 4.93±1.32 5.83±1.62 -1.76 0.090 Hypertension [Yes, n(%)] 2(13.33) 10(50.00) 5.12 0.024 Two dimensional echocardio-gram LVEDV (mL) 106.93±35.48 121.65±39.61 -1.14 0.264 LVESV (mL) 50.67±24.42 62.90±29.32 -1.31 0.199 LVEF (%) 54.20±6.06 50.15±7.18 1.76 0.087 FS (%) 27.93±4.38 25.10±4.91 1.77 0.086 LALR(mm) 39.60±4.42 41.60±4.33 -1.34 0.189 SWMA [n(%)] 7(46.67) 18(90.00) 5.91 0.008 LVEDV: Left ventricular end-diastolic volume; LVESV: Left ventricular end-systolic volume; LVEF: Left ventricular ejection fraction; FS: Short axis shortening rate; LALR: Left atria left-right diameter; SWMA: Segmental wall motion abnormality.  下载: 导出CSV
下载: 导出CSV
表 2 两组人群冠脉支配区域室壁的超声造影特征比较
Table 2. Comparison of contrast-enhanced ultrasound features of the ventricular wall of the coronary artery domination area between the two groups (Mean±SD)
Quantitative parameters of MCE Control group(n=45) Coronary artery disease group(n=42) t/U P AUC(dB sec) 34.31±11.43 25.02±8.04 4.36 < 0.001 MPI(dB) 9.69±1.52 3.61±1.57 18.32 < 0.001 Perfusion rate(dB/sec) 2.41±1.18 2.07±0.94 1.49 0.139 Time to peak (sec) 1.29 1.54 872.5 0.538 AUC: Area under the curve; MPI: Peak myocardial intensity.
下载: 导出CSV
-
[1] 胡盛寿, 高润霖, 刘力生, 等. 《中国心血管病报告2018》概要[J]. 中国循环杂志, 2019, 34(3): 209-20. doi: 10.3969/j.issn.1000-3614.2019.03.001 [2] Wetmore JB, Tang FM, Sharma A, et al. The association of chronic kidney disease with the use of renin-angiotensin system inhibitors after acute myocardial infarction[J]. Am Heart J, 2015, 170(4): 735-43. doi: 10.1016/j.ahj.2015.07.019 [3] 中国医师协会急诊医师分会, 国家卫健委能力建设与继续教育中心急诊学专家委员会, 中国医疗保健国际交流促进会急诊急救分会. 急性冠脉综合征急诊快速诊治指南(2019)[J]. 临床急诊杂志, 2019, 20(4): 253-62. doi: 10.13201/j.issn.1009-5918.2019.04.001 [4] 罗江, 祝唯, 苗涵. 冠脉CT血管成像斑块定量参数预测冠心病患者心肌缺血事件的临床价值[J]. 分子影像学杂志, 2023, 46(2): 347-51. doi: 10.12122/j.issn.1674-4500.2023.02.30 [5] 李文玲, 翟晓辉, 于学文, 等. 国内外64层螺旋CT诊断冠心病研究差异的荟萃分析[J]. 中华心血管病杂志, 2011, 39(6): 553-8. doi: 10.3760/cma.j.issn.0253-3758.2011.06.016 [6] 李爱英, 张世新, 吕铁钢. 64层螺旋CT冠状动脉血管成像在冠心病诊断中的应用价值[J]. 中华临床医师杂志: 电子版, 2013, 7(15): 189-90. https://www.cnki.com.cn/Article/CJFDTOTAL-ZLYD201315116.htm [7] 何其舟, 余飞, 付亚军, 等. 双源CT自适应前瞻性心电门控自由心率冠状动脉成像对图像质量及辐射剂量的影响[J]. 放射学实践, 2017, 32(5): 488-93. https://www.cnki.com.cn/Article/CJFDTOTAL-FSXS201705016.htm [8] 刘佳楠, 孙宇佳, 安换换, 等. 负荷心肌超声造影测定冠状动脉血流储备的临床应用[J]. 中国临床医学影像杂志, 2020, 31(3): 180-3, 187. https://www.cnki.com.cn/Article/CJFDTOTAL-LYYX202003011.htm [9] 黄艳, 丁明岩, 栾波, 等. 心肌声学造影评价冠状动脉慢性完全闭塞病变患者介入治疗的早期疗效[J]. 临床超声医学杂志, 2020, 22(5): 326-30. doi: 10.3969/j.issn.1008-6978.2020.05.003 [10] Zhang JC, Ma MW, Li HJ, et al. Early diagnosis of coronary microvascular dysfunction by myocardial contrast stress echocardiography[J]. Math Biosci Eng, 2023, 20(5): 7845-58. doi: 10.3934/mbe.2023339 [11] 方杰, 李春梅, 林薿, 等. 心肌造影多巴酚丁胺负荷超声心动图定量评价冠心病患者心肌灌注的临床研究[J]. 心血管病学进展, 2021, 42(8): 742-7. https://www.cnki.com.cn/Article/CJFDTOTAL-XXGB202108019.htm [12] Malakar AK, Choudhury D, Halder B, et al. A review on coronary artery disease, its risk factors, and therapeutics[J]. J Cell Physiol, 2019, 234(10): 16812-23. doi: 10.1002/jcp.28350 [13] 邵江, 牟华明, 李俊. 128层螺旋CT冠状动脉成像在冠心病诊断中的应用价值[J]. 中国循证心血管医学杂志, 2014, 6(1): 34-6. https://www.cnki.com.cn/Article/CJFDTOTAL-PZXX201401013.htm [14] Rizvi A, Han D, Danad I, et al. Diagnostic performance of hybrid cardiac imaging methods for assessment of obstructive coronary artery disease compared with stand-alone coronary computed tomography angiography: a meta-analysis[J]. JACC Cardiovasc Imaging, 2018, 11(4): 589-99. [15] 杨兴军, 杨辉, 郭欣, 等. 冠状动脉慢性完全闭塞病变微循环临床研究进展[J]. 心脏杂志, 2019, 31(4): 474-8. https://www.cnki.com.cn/Article/CJFDTOTAL-XGNZ201904023.htm [16] 张运, 尹立雪, 邓又斌, 等. 中国心血管超声造影检查专家共识[J]. 中华超声影像学杂志, 2016, 25(4): 277-93. https://www.cnki.com.cn/Article/CJFDTOTAL-ZHCD201509002.htm [17] 赵莹, 王浩. 2017 EACVI临床实践建议解读: 心脏超声造影检查[J]. 中国超声医学杂志, 2018, 34(5): 463-5. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGCY201805025.htm [18] Porter T, Mulvagh S, Abdelmoneim S, et al. Clinical applications of ultrasonic enhancing agents in echocardiography: 2018 American society of echocardiography guidelines update[J]. J Am Soc Echocardiogr, 2018, 31(3): 241-74. [19] Bhatia VK, Senior R. Contrast echocardiography: evidence for clinical use[J]. J Am Soc Echocardiogr, 2008, 21(5): 409-16. [20] Shentu WH, Deng YB, Huang RQ, et al. Evaluation of myocardial viability after myocardial infarction with intravenous real-time myocardial contrast echocardiography[J]. J Huazhong Univ Sci Technol (Med Sci), 2008, 28(3): 291-4. [21] 韩炫, 朱文晖, 陈文娟. 心肌声学造影和二维斑点追踪技术评估冠心病患者心肌灌注与收缩功能[J]. 中南大学学报: 医学版, 2021, 46(11): 1233-40. https://www.cnki.com.cn/Article/CJFDTOTAL-HNYD202111009.htm [22] Lin YJ, Guan X, Ren K, et al. Low-dose dobutamine stress myocardial contrast echocardiography for the evaluation of myocardial microcirculation and prediction of overall cardiac function recovery[J]. Exp Ther Med, 2020, 20(2): 1315-20. [23] 张源祥, 邱银汝, 梁志尧, 等. 多巴酚丁胺负荷超声造影诊断冠心病的初步研究[J]. 中华医学超声杂志: 电子版, 2020, 17(4): 327-34. https://www.cnki.com.cn/Article/CJFDTOTAL-ZHCD202004010.htm [24] 张源祥, 邱银汝, 梁志尧, 等. 三磷酸腺苷和多巴酚丁胺负荷超声造影在冠心病诊断中的对比研究[J]. 中华医学超声杂志: 电子版, 2020, 17(4): 335-40. https://www.cnki.com.cn/Article/CJFDTOTAL-ZHCD202004011.htm [25] Lyu WY, Qin C, Wang XT, et al. The application of myocardial contrast echocardiography in assessing microcirculation perfusion in patients with acute myocardial infarction after PCI[J]. BMC cardiovascular disorders, 2022, 22 (1): 233. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 102
- HTML全文浏览量: 85
- PDF下载量: 9
- 被引次数: 0