



Construction of a model for predicting the risk of lower extremity deep venous thrombosis secondary to atypical left common iliac vein compression by baseline enhanced CT combined with clinical data
-
摘要:
目的 探讨基于基线增强CT联合临床资料的非典型左髂总静脉(LCIV)受压患者诊治期间下肢深静脉血栓的发生率及风险预测模型构建。 方法 回顾性分析2017年6月~2022年10月南方医科大学顺德医院首次诊治为非典型LCIV的患者共137例,且诊治期间均未接受药物或物理等措施预防下肢深静脉血栓(DVT)形成。通过随访是否发生下肢深静脉血栓分为无DVT组(n=41)和DVT组(n=96),比较两组之间的基线CT征象及临床资料的差异,采用二元Logistic回归单因素及多因素分析筛选出独立危险因素,采用ROC曲线分析各危险因素的预测效能。 结果 非典型LCIV继发DVT的发生率为70%(96/137)。单因素二元Logistic回归分析显示,LCIV最小短径、右髂总静脉最小短径、LCIV受压比例、下腰椎前曲角、下肢症状、D-二聚体及纤维蛋白降解产物(FDP)为非典型LCIV继发DVT的危险因素(P<0.05)。多因素Logistic回归分析显示,FDP(OR=1.05,95% CI:1.01~1.1,P=0.002)、下肢症状(OR=12.59,95% CI:2.78~57.12,P<0.001)及LCIV受压比例(OR=1.05,95% CI:1.01~1.09,P= 0.02)为独立危险因素。ROC曲线分析显示FDP、下肢症状、LCIV受压比例的ROC曲线下面积分别为0.879、0.826及0.827。联合预测模型曲线下面积为0.921,其敏感度和特异性分别为95.79%及78.05%。 结论 非典型LCIV继发DVT发生率较高,FDP、下肢症状、LCIV受压比例为其发生的独立危险预测因素,联合3个独立危险因素的预测模型具有较高的预测效能,为非典型LCIV继发DVT患者提供个性化风险评估。 -
关键词:
- 非典型左髂总静脉受压 /
- 深静脉血栓 /
- 增强CT /
- 风险模型
Abstract:Objective To explore the incidence and risk prediction model of lower extremity deep venous thrombosis in patients with atypical left common iliac vein compression based on baseline enhanced CT combined with clinical data. Methods A total of 137 patients with atypical left common iliac vein (LCIV) compression diagnosed for the first time in Shunde Hospital of Southern Medical University from June 2017 to October 2022 were retrospectively analyzed. These patients did not receive any medication or physical measures to prevent the formation of DVT during the diagnosis and treatment period. Based on the occurrence of lower limb DVT during follow-up, the patients were divided into the non-DVT group (n=41) and the DVT group (n=96). The statistical differences in baseline CT findings and clinical data between the two groups were compared, and independent risk factors were selected through univariate and multivariate logistic regression analysis. The predictive efficacy of each risk factor was analyzed using ROC curve analysis. Results The incidence of DVT secondary to atypical LCIV was 70% (96/137). Univariate binary logistic regression analysis showed that LCIV minimum short diameter, right common iliac vein minimum short diameter, LCIV compression ratio, lower lumbar anterior flexion angle, symptoms of lower limb, D-dimer and fibrin degradation product (FDP) were risk factors for DVT secondary to atypical LCIV (P<0.05). Multivariate Logistic regression analysis showed that FDP (OR=1.05, 95% CI=1.01- 1.1, P=0.002), symptom of lower limb (OR=12.59, 95% CI: 2.78- 57.12, P<0.001) and LCIV compression ratio (OR=1.05, 95% CI: 1.01-1.09, P=0.02) were independent risk factors. ROC curve analysis showed that the AUC of FDP, symptom of lower limb and LCIV compression ratio were 0.879, 0.826 and 0.827, respectively. The AUC of the combined prediction model was 0.921, and the sensitivity and specificity were 95.79% and 78.05%, respectively. Conclusion The incidence of secondary DVT with atypical LCIV is high. FDP, symptom of lower limb, LCIV compression ratio are independent risk predicators for their occurrence. The prediction model combined with the three independent risk factors has high predictive efficacy, providing personalized risk assessment for patients with secondary DVT with atypical LCIV. -

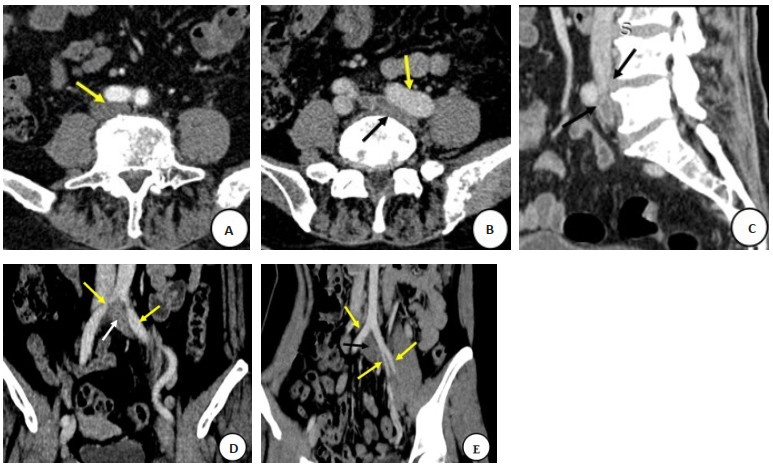
图 1 非典型LCIV患者CT图像判读
Figure 1. CT image interpretation of atypical LCIV patients. A-B: Two compression points showed LCIV stenosis, one caused by RCIA (A yellow arrow), the other secondary to left iliac artery aneurysmal dilation (B yellow arrow), and the left common iliac vein (B black arrow); C: The CT image of sagittal reconstruction showed LCIV narrowing due to L4/5 intervertebral disc herniation and lumbar bone hyperplasia (black arrow); D: The CT image of coronal reconstruction showed two narrow compression positions of LCIV, located near the junction of the inferior vena cava and the middle of the left common iliac vein (yellow arrow), and the left common iliac vein (white arrow); E: The CT images of coronal reconstruction showed that LCIV was compressed and dissected by the right common iliac artery, left internal and external iliac arteries (yellow arrow), and left common iliac vein (black arrow), respectively.

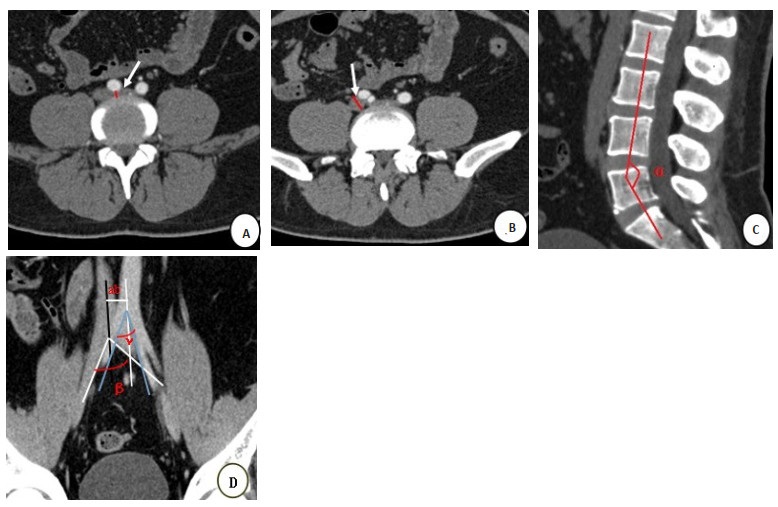
图 2 CT定量参数测量示意图
Figure 2. CT quantitative parameter measurement schematic diagram. A: LCIV minimum short diameter measurement layer (white arrow); B: RCIV minimum short diameter measurement layer (white arrow); C: Lower lumbar anterior flexion angle (α); D: Angle of bifurcation of inferior vena cava(β), abdominal aortic bifurcation angle (γ), and the distance between the bifurcation planes of the inferior vena cava and the abdominal aorta (ab, mm).

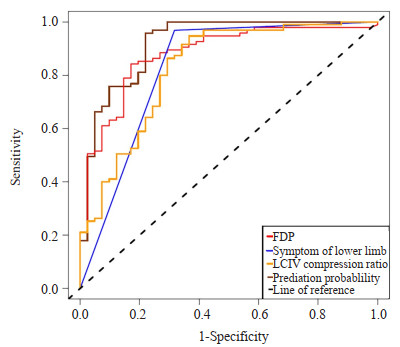
图 3 各独立危险因素及联合预测概率的ROC曲线比较
Figure 3. ROC curve comparison of independent risk factors and joint prediction probability.
表 1 两组间非典型LCIV患者影像及临床资料比较
Table 1. Comparison of imaging and clinical data of atypical LCIV patients between the two groups (Mean±SD)
Index Non-DVT group (n=41) DVT group (n=96) t/c2 P Gender (Female/Male, n) 25/16 63/33 0.228 0.632 Age (years) 59.4±17.9 58.1±17.00 0.399 0.691 Symptom of lower limb (No/Yes, n) 28/13 3/93 69.043 < 0.001 D-Dimer (μg/mL) 5.43±17.3 30.3±36.8 -5.379 < 0.001 FDP (μg/mL) 7.96±12.0 51.74±64.6 -6.358 < 0.001 TT (s) 18.5±3.68 18.7±7.61 -0.198 0.843 APTT (s) 32.4±9.22 31.81±7.67 0.42 0.676 FIB (mg/dL) 4.05±3.75 4.03±3.79 0.019 0.985 INR 1.08±0.354 1.09±0.399 -0.188 0.851 Thrombotic triggering factors (No/Yes, n) 18/23 44/52 0.021 0.884 LCIV minimum short diameter (mm) 5.83±2.07 3.76±1.95 5.47 < 0.001 RCIV minimum short diameter (mm) 12.1±3.18 14.5±9.57 -2.181 0.031 LCIV compression ratio (%) 49.0±18.4 72.3±13.8 -7.286 < 0.001 IVC bifurcation angle (°) 66.4±17.2 66.5±17.5 -0.02 0.984 AA bifurcation angle (°) 47.2±12.6 48.1±13.1 -0.383 0.703 IVC-AA bifurcation plane spacing (mm) 16.5±5.06 16.1±5.68 0.402 0.688 Lower lumbar anterior flexion angle (°) 144.0±9.99 140.0±7.71 2.44 0.017 FDP: Fibrin degradation products; TT: Thrombin time; APTT: Activated partial thromboplastin time; FIB: Fibrinogen; INR: International normalized ratio; LCIV: Left common iliac vein; RCIV: Right common iliac vein; IVC: Inferior vena cava; AA: Abdominal aorta; IVC-AA: Inferior vena cava to abdominal aorta.  下载: 导出CSV
下载: 导出CSV
表 2 非典型LCIV患者继发左下肢DVT单因素的Logistic回归分析
Table 2. Logistic regression analysis of single factor of atypical LCIV with secondary left lower limb DVT patients
Variable Univariate analysis OR 95% CI P Gender 0.82 0.38-1.74 0.60 Age 1 0.97-1.02 0.68 Symptom of lower limb 66.77 17.76-251.06 < 0.001 D-Dimer 1.11 1.05-1.17 < 0.001 FDP 1.11 1.06-1.17 < 0.001 TT 1 0.95-1.07 0.88 APTT 0.99 0.95-1.03 0.65 FIB 1 0.91-1.1 0.99 INR 1.1 0.4-2.98 0.86 Thrombotic triggering factors 0.92 0.44-1.93 0.84 LCIV minimum short diameter 0.62 0.51-0.76 < 0.001 RCIV minimum short diameter 1.16 1.03-1.3 0.02 LCIV compression ratio 1.09 1.06-1.12 < 0.001 IVC bifurcation angle 1 0.98-1.02 0.98 AA bifurcation angle 1.01 0.98-1.03 0.70 IVC-AA bifurcation plane spacing 0.99 0.92-1.06 0.70 Lower lumbar anterior flexion angle 0.94 0.9-0.99 0.01
下载: 导出CSV
表 3 非典型LCIV患者继发左下肢DVT多因素的Logistic回归分析
Table 3. Logistic regression analysis of multiple factors of atypical LCIV with secondary left lower limb DVT patients
Variable Multivariate analysis OR 95% CI P FDP 1.05 1.01-1.1 0.02 Symptom of lower limb 12.59 2.78-57.12 < 0.001 LCIV compression ratio 1.05 1.01-1.09 0.02
下载: 导出CSV
表 4 各独立危险因素及联合预测概率的ROC预测效能
Table 4. ROC prediction efficiency of independent risk factors and joint prediction probabilities
Index Youden index AUC (95% CI) Sensitivity(%) Specificity(%) Cut-off P FDP 0.671 0.879 (0.816-0.943) 84.21 82.93 10.90 < 0.001 LCIV compression ratio 0.827 0.827 (0.745-0.909) 94.74 63.41 48.73% < 0.001 Symptom of lower limb 0.651 0.826 (0.751, 0.900) 96.84 68.29 - < 0.001 Predicted Probability 0.738 0.921 (0.866-0.976) 95.79 78.05 - < 0.001
下载: 导出CSV
-
[1] Cockett FB, Lea Thomas M. The iliac compression syndrome[J]. Br J Surg, 2005, 52(10): 816-21. doi: 10.1002/bjs.1800521028 [2] May R, Thurner J. The cause of the predominantly sinistral occurrence of thrombosis of the pelvic veins[J]. Angiology, 1957, 8(5): 419-27. doi: 10.1177/000331975700800505 [3] Poyyamoli S, Mehta P, Cherian M, et al. May-Thurner syndrome[J]. Cardiovasc Diagn Ther, 2021, 11(5): 1104-11. doi: 10.21037/cdt.2020.03.07 [4] 蔡昊, 李开龙, 庞云峰, 等. May-Thurner综合征的影像学诊断进展[J]. 血管与腔内血管外科杂志, 2022, 8(10): 1212-6. doi: 10.19418/j.cnki.issn2096-0646.2022.10.14 [5] 黄天安, 金泳海, 梁黎, 等. 下肢深静脉血栓形成后综合征风险列线图预测模型建立[J]. 介入放射学杂志, 2022, 31(1): 35-8. https://www.cnki.com.cn/Article/CJFDTOTAL-JRFS202201009.htm [6] Tewoldemedhin B, Tewoldemedhin NK, Ahmed S, et al. A curious presentation of may-thurner syndrome with isolated iliofemoral deep vein thrombosis[J]. Cureus, 2022, 14(2): e22124. [7] Sun Y, Song S. Nonnegligible causes of symptoms of acute lower extremities 3 cases of May-Thurner syndrome with deep vein thrombosis[J]. Thromb J, 2021, 19(1): 25. doi: 10.1186/s12959-021-00278-7 [8] 欧阳裕锋, 胡秋根, 岑玉坚, 等. 双能量CT直接增强法在双下肢静脉成像中的优势[J]. 分子影像学杂志, 2019, 42(1): 5-9. doi: 10.12122/j.issn.1674-4500.2019.01.02 [9] Kim JH, Lee SK, Kim EH, et al. Acute left iliofemoral vein thrombosis: comparison between simple and bony May-Thurner syndrome in CT venography[J]. Vascular, 2022. doi: 10.1177/17085381221111010. [10] 李宏甫. 多层螺旋CT诊断髂静脉受压综合征的临床价值[J]. 医学理论与实践, 2021, 34(15): 2676-8. doi: 10.19381/j.issn.1001-7585.2021.15.058 [11] Harbin MM, Lutsey PL. May-Thurner syndrome: history of understanding and need for defining population prevalence[J]. J Thromb Haemost, 2020, 18(3): 534-42. doi: 10.1111/jth.14707 [12] Li JY, Chen HB, Chen WJ, et al. Novel typing of iliac vein compression in asymptomatic individuals evaluated by contrast enhanced CT[J]. Surg Radiol Anat, 2021, 43: 1149-57. doi: 10.1007/s00276-021-02678-w [13] 章杰. 双重型左髂总静脉受压与左下肢深静脉血栓的关系[D]. 大连: 大连医科大学, 2019. [14] Nayak SB, Vasudeva SK. Variant formation of left common iliac vein by the confluence of four veins[J]. Morphologie, 2022, 106(354): 203-5. doi: 10.1016/j.morpho.2021.05.116 [15] Park JY, Park KM, Cho SG, et al. Atypical iliac vein compression in patients with symptomatic May-Thurner syndrome[J]. Diagn Interv Radiol, 2021, 27(3): 372-7. doi: 10.5152/dir.2021.20183 [16] 江旭东. 髂静脉狭窄与下肢深静脉血栓形成关系的血流动力学研究[D]. 苏州: 苏州大学, 2021. [17] 蒋俊, 杨帆. 介入治疗在左髂静脉受压综合征并发左下肢深静脉血栓形成中的疗效观察[J]. 血栓与止血学, 2022, 28(3): 1024-6. doi: 10.3969/j.issn.1009-6213.2022.03.301 [18] 黄渌, 李文文, 崔佳森. 髂静脉压迫综合征继发下肢静脉溃疡治疗的临床研究[J]. 血管与腔内血管外科杂志, 2022, 8(1): 51-4, 60. https://www.cnki.com.cn/Article/CJFDTOTAL-XGQW202201013.htm [19] 刘劲燕, 郭璐. 静脉血栓栓塞症的发病机制及早期诊断标志物的研究进展[J]. 实用医院临床杂志, 2019, 16(3): 266-9. doi: 10.3969/j.issn.1672-6170.2019.03.083 [20] Nazzal M, El-Fedaly M, Kazan V, et al. Incidence and clinical significance of iliac vein compression[J]. Vascular, 2015, 23(4): 337-43. doi: 10.1177/1708538114551194 [21] 左香燚, 李欢欢, 姚国庆, 等. 无下肢静脉疾病症状人群及下肢静脉曲张患者髂静脉狭窄及相关因素分析: 历史性队列研究[J]. 中国普外基础与临床杂志, 2023, 30(3): 315-9. https://www.cnki.com.cn/Article/CJFDTOTAL-ZPWL202303011.htm [22] Lopes DF, Zerati AE, De Luccia N. Imaging signs of may-thurner syndrome in asymptomatic patients: computed tomography angiography analysis of kidney donors[J]. Ann Vasc Surg, 2023, 88: 25-31. doi: 10.1016/j.avsg.2022.07.003 [23] 朱桥华. 左髂总静脉受压继发下肢深静脉血栓相关的影像解剖、风险预测模型及无滤器腔内治疗方法学研究[D]. 广州: 南方医科大学, 2022. [24] Kim MS, Park HS, Hong HP, et al. Risk factors for stent occlusion after catheter-directed thrombolysis and iliac vein stenting in the treatment of May-Thurner syndrome with iliofemoral deep vein thrombosis: a retrospective cohort study[J]. Quant Imaging Med Surg, 2022, 12(12): 5420-32. doi: 10.21037/qims-22-515 [25] Costa LMG, Tachibana A, da Silva Magao F, et al. Magnetic resonance imaging evaluation of left common iliac vein compression in patients with and without symptoms of venous disease[J]. Circ J, 2020, 84(5): 763-8. doi: 10.1253/circj.CJ-19-0913 [26] Zhang WL, Chen CL, Su GD, et al. Three-dimensional in vivo anatomical study of female iliac vein variations[J]. J Investig Surg, 2022, 35(9): 1679-85. doi: 10.1080/08941939.2022.2095469 [27] Bałabuszek K, Toborek M, Pietura R. Comprehensive overview of the venous disorder known as pelvic congestion syndrome[J]. Ann Med, 2022, 54(1): 22-36. doi: 10.1080/07853890.2021.2014556 [28] Salahuddin T, Armstrong EJ. Intervention for iliofemoral deep vein thrombosis and may-thurner syndrome[J]. Interv Cardiol Clin, 2020, 9(2): 243-54. [29] Chen F, Huang JG, Liu X, et al. Left iliac vein involvement is a protective factor against symptomatic pulmonary embolism in lower left extremity deep vein thrombosis[J]. J Vasc Surg Venous Lymphatic Disord, 2022, 10(6): 1272-8. [30] Shi YD, Yuan YC, Gong MF, et al. The association between iliac vein compression degree and characteristics of first diagnosed left lower extremity deep vein thrombosis[J]. Front Cardiovasc Med, 2022, 9: 1073586. [31] Zhu QH, Yang L, Zhu HY, et al. Prevalence of left iliac vein compression in an asymptomatic population and patients with left iliofemoral deep vein thrombosis: a multicenter cross-sectional study in Southern China[J]. Phlebology, 2022, 37(8): 602-9. [32] Fereydooni A, Stern JR. Contemporary treatment of may-thurner syndrome[J]. J Cardiovasc Surg (Torino), 2021, 62(5): 447-55. [33] 侯瑞鸿, 母建奎, 孙梦月, 等. MSCTV对下肢静脉血栓性疾病的诊断价值[J]. 河北医科大学学报, 2020, 41(10): 1195-9. https://www.cnki.com.cn/Article/CJFDTOTAL-HBYX202010017.htm [34] 李嘉颖, 孙志超. MSCT对无下肢症状患者髂静脉压迫特征和分型的临床研究[C]. 中国中西医结合学会医学影像专业委员会第十七次全国学术大会暨甘肃省中西医结合学会医学影像专业委员会第六届学术年会, 中国兰州, 2019. [35] Umakanth S, Karnik SA, Kashyap AR, et al. May-Thurner syndrome: an unusual cause of unprovoked deep vein thrombosis of the left lower limb[J]. BMJ Case Rep, 2022, 15(1): e244103. [36] 陶黎, 朱嵬, 张晓宇, 等. NCE-MRA在评价髂静脉受压分型中的应用价值[J]. 血管与腔内血管外科杂志, 2022, 8(1): 17-21. https://www.cnki.com.cn/Article/CJFDTOTAL-XGQW202201005.htm -

 点击查看大图
点击查看大图
计量
- 文章访问数: 120
- HTML全文浏览量: 46
- PDF下载量: 2
- 被引次数: 0