



99mTc-DTPA肾动态显像结合尿N-乙酰-D-氨基葡萄糖苷酶可较好诊断中老年原发性高血压患者的早期肾损害
doi: 10.12122/j.issn.1674-4500.2023.05.08
99mTc-DTPA renal dynamic imaging combined with urinary N-acetyl-D-glucosaminidase can effectively diagnose early renal damage in middle-aged and elderly patients with essential hypertension
-
摘要:
目的 探讨99锝-二乙三胺五醋酸(99mTc-DTPA)肾动态显像方法与尿N-乙酰-D-氨基葡萄糖苷酶(尿NAG)检测在中老年原发性高血压早期肾损害中的临床意义。 方法 选取80例中老年原发性高血压患者为观察组,年龄63.0±8.6岁,按血压水平分为高血压1级组(H1组)、高血压2级组(H2组)、高血压3级组(H3组);根据患者尿微量白蛋白/尿肌酐水平分为正常白蛋白尿组(NA组)53例,微量白蛋白尿组(MA组)27例;同时选取20例中老年健康体检者为对照组(NC组),年龄61.1±9.6岁。所有入选者均行肾动态显像,计算肾小球滤过率(GFR)、高峰时间(tp)、半排时间(t1/2),留取随机清洁中段尿液检查尿NAG,空腹抽血测血胱抑素C(Cys-C)和血肌酐。上述指标按高血压级别进行组间比较,同时将NA、MA与对照组进行组间比较。 结果 高血压各组与对照组相比,GFR均降低,tp、t1/2延长,尿NAG升高;高血压组间比较,随着血压水平的升高,GFR降低,tp、t1/2延长,尿NAG、Cys-C升高(P<0.05);H2、H3组Cys-C较对照组升高(P<0.05)。H1组Cys-C与对照组比较差异无统计学意义(P > 0.05)。高血压患者NA、MA组与对照组比较,NA与MA组GFR降低,tp、t1/2延长,尿NAG及Cys-C升高(P<0.05)。NA、MA组血肌酐与对照组比较差异无统计学意义(P > 0.05)。MA与NA组比较,MA组较NA组GFR降低,tp、t1/2延长,尿NAG及Cys-C升高(P<0.05),两组间血肌酐差异无统计学意义(t=0.885,P > 0.05)。高血压组GFR与尿NAG呈负相关(t=-0.39,P<0.01)。 结论 肾动态显像及尿NAG对原发性高血压患者早期肾损害具有较好诊断价值。 -
关键词:
- 高血压 /
- 早期肾损害 /
- 肾动态显像 /
- 肾小球滤过率 /
- 尿N-乙酰-D-氨基葡萄糖苷酶
Abstract:Objective To explore the clinical significance of 99mTc-DTPA renal dynamic imaging and urinary N-acetyl-β-D-glucosamine (NAG) in the early stage of renal damage in middle-aged and elderly patients with essential hypertension. Methods Eighty middle-aged and elderly patients with essential hypertension were selected as the observation group, with an average age of 63.0±8.6 years old. They were divided into grade 1 hypertension group (H1 group), grade 2 hypertension group (H2 group) and grade 3 hypertension group (H3 group) according to blood pressure level. According to urinary albumin / creatinine ratio, patients were divided into normal albuminuria group (NA group, n=53) and microalbuminuria group (MA group, n=27). At the same time, 20 middle-aged and elderly healthy subjects were selected as the control group (NC group), with an average age of 61±9.6 years old. Renal dynamic imaging was performed in all patients. Glomerular filtration rate (GFR), peak time (tp) and half excretion time (t1/2) were calculated. Urinary NAG was detected by random clean midstream urine. Fasting blood samples were taken to measure serum cystatin C (Cys-C) and serum creatinine. The above indexes were compared between groups according to the grade of hypertension, and NA, MA and control groups were compared at the same time. Results Compared with the control group, GFR was decreased, tp and t1/2 were prolonged, and urinary NAG was increased in hypertension groups.Compared with the hypertension group, with the increase of blood pressure, GFR decreased, tp, t1/2prolonged, urinary NAG and Cys-C increased (P<0.05). Cys-C in H2 and H3 groups was higher than that in control group (P<0.05). There was no significant difference in Cys-C between H1 group and control group (P > 0.05). Comparison of NA and MA groups with control group in patients with hypertension, GFR decreased, peak time and half excretion time prolonged, urinary NAG and Cys-C increased in NA and MA group (P<0.05). There was no significant difference in serum creatinine between the NA and MA groups and the control group (P > 0.05). Compared with NA group, GFR in MA group was lower, tp and t1/2 were longer, urinary NAG and Cys-C were higher in MA group than in NA group, but there was no significant difference in serum creatinine between the two groups (t=0.885, P > 0.05). There was a negative correlation between GFR and urinary NAG in hypertension group (r=-0.39, P<0.01). Conclusion Renal dynamic imaging combined with urinary NAG has good value in the diagnosis of early renal damage in patients with essential hypertension. -

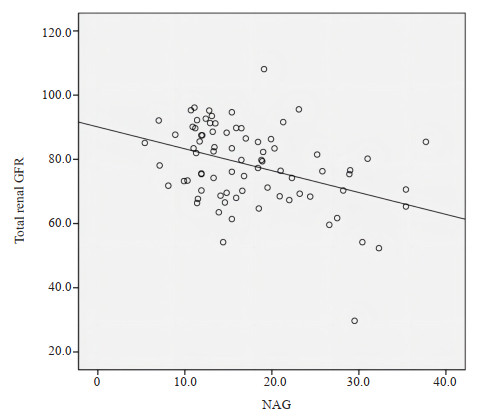
图 1 99mTc-DTPA肾脏动态成像
Figure 1. 99mTc-DTPA renal dynamic imaging. GFR: Glomerular filtration rate.

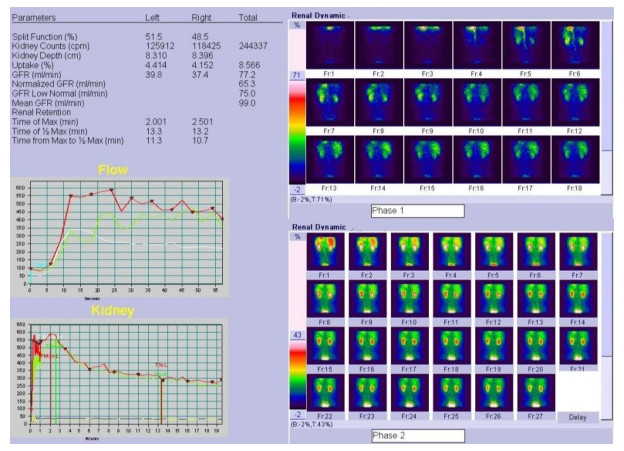
图 2 高血压组肾动态显像总肾GFR与尿NAG的关系
Figure 2. The relationship between total renal GFR and urinary NAG in hypertension group.
表 1 高血压各组与对照组一般资料的比较
Table 1. Comparison of general data between hypertension group and control group (Mean±SD)
Groups Gender (Male/Female, n) Age(year) BMI(kg/m2) TC(mmol/L) TG(mmol/L) LDL(mmol/L) FBG(mmol/L) Control group (n=20) 10/10 61.62±9.17 24.05±1.70 4.38±1.54 1.44±0.42 2.67±0.48 4.87±0.71 H1 group (n=18) 8/10 60.51±7.50 25.18±2.11 4.75±1.36 1.51±0.56 2.85±0.61 4.69±0.81 H2 group (n=32) 16/16 62.01±9.76 24.67±2.26 4.87±1.64 1.37±0.65 2.90±0.79 5.1±0.68 H3 group (n=30) 15/15 63.01±8.90 25.30±2.71 4.68±0.71 1.54±0.62 2.76±0.81 4.78±0.47 TC: Total cholesterol; TG: Triglyceride; LCL: Low-density lipoprotein; FBG: Fasting blood glucose.  下载: 导出CSV
下载: 导出CSV
表 2 不同高血压分级组与对照组总GFR、tp、t1/2、尿NAG、Cys-C、Scr比较
Table 2. Comparison of total GFR, tp, t1/2, urinary NAG, Cys-C and Scr between different hypertension grading groups and control group (Mean±SD)
Group Total GFR (mL/min) tp (min) t1/2 (min) Urinary NAG (U/L) Cys-C (mg/L) Scr (μmol/L) Control group (n=20) 93.16±7.59 3.01±0.50 6.82±0.62 9.28±1.80 0.73±0.11 68.05±9.91 H1 group (n=18) 87.51±7.42* 3.32±0.39* 7.70±1.49* 12.77±4.4# 0.70±0.18 72.06±14.70 H2 group (n=32) 79.13±11.53# 3.71±0.5# 8.93±1.52# 16.82±6.6# 0.92±0.17# 67.69±9.91 H3 group (n=30) 72.19±12.45# 4.22±0.9# 10.07±2.0# 20.33±6.5# 1.11±0.32# 71.33±16.73 F 10.758 9.971 10.775 8.525 16.773 0.621 t < 0.001 0.003 < 0.001 0.010 0.003 0.540 GFR: Glomerular filtration rate; tp: Peak time; t1/2: Half excretion time; NAG: N-acetyl-β-D-glucosamine; Cys-C: Serum cystatin C; Scr: Serum creatinine. *P<0.05 vs control group; #P<0.01 vs control group.
下载: 导出CSV
表 3 NA、MA、对照组的总GFR、tp、t1/2、尿NAG、Cys-C、Scr比较
Table 3. Comparison of total GFR, tp, t1/2, urinary NAG, Cys-C, Scr among NA group, MA group and control group (Mean±SD)
Groups Total GFR (mL/min) tp(min) t1/2 (min) Urinary NAG(U/L) Cys-c(mg/L) Scr(μmol/L) Control group (n=20) 93.16±7.59 3.01±0.50 6.82±0.62 9.28±1.80 0.73±0.11 68.05±9.91 NA group (n=53) 81.13±10.50* 3.63±0.71* 8.65±1.64* 16.13±6.29* 0.87±0.25* 68.94±13.49 MA group (n=27) 73.07±14.30* 4.17±0.78* 9.93±2.20* 19.36±7.21* 1.08±0.30* 72.19±18.88 t -2.862 3.121 2.679 2.068 3.411 0.885 P 0.005 0.003 0.011 0.042 0.001 0.379 *P<0.05 vs control group. NA: Normal albuminuria; MA: Microalbuminuria.
下载: 导出CSV
-
[1] 中国高血压防治指南修订委员会. 中国高血压防治指南2010[J]. 中华高血压杂志, 2011, 19(8): 701-43. doi: 10.16439/j.cnki.1673-7245.2011.08.009 [2] Otsuka T, Kato K, Kachi Y, et al. Serum cystatin C, creatinine-based estimated glomerular filtration rate, and the risk of incident hypertension in middle-aged men[J]. Am J Hypertens, 2014, 27(4): 596-602. doi: 10.1093/ajh/hpt164 [3] Orsal E, Seven B, Subasi ID, et al. Vesicoureteral reflux in a nonfunctioning kidney detected by 99mTc-DTPA study[J]. Jpn J Radiol, 2013, 31(12): 823-5. doi: 10.1007/s11604-013-0259-8 [4] De Miguel C, Speed JS, Kasztan M, et al. Endothelin-1 and the kidney: new perspectives and recent findings[J]. Curr Opin Nephrol Hypertens, 2016, 25(1): 35-41. doi: 10.1097/MNH.0000000000000185 [5] Li H, Liu LT, Zhao WM, et al. Effect of traditional and integrative regimens on quality of life and early renal impairment in elderly patients with isolated systolic hypertension[J]. Chin J Integr Med, 2010, 16(3): 216-21. doi: 10.1007/s11655-010-0216-y [6] 罗镜才. 血清胱抑素C在高血压患者肾功能评价中的应用[J]. 中国医学工程, 2016, 24(7): 108-9. doi: 10.19338/j.issn.1672-2019.2016.07.049 [7] 傅兰君, 陈红波, 史佳丽, 等. MDRD计算肾小球滤过率与核素测量清除率在不同肾脏病中的比较[J]. 实用医学杂志, 2016, 32(10): 1634-6. doi: 10.3969/j.issn.1006-5725.2016.10.024 [8] Chen JX, Tang H, Huang H, et al. Development and validation of new glomerular filtration rate predicting models for Chinese patients with type 2 diabetes[J]. J Transl Med, 2015, 13: 317. doi: 10.1186/s12967-015-0674-y [9] 李繁, 莫慧, 张宁, 等. 99mTc-DTPA肾动态显像在痛风性肾病早期诊断中的意义[J]. 广东医学院学报, 2016, 34(4): 397-9. doi: 10.3969/j.issn.1005-4057.2016.04.017 [10] 项希桥. SPECT肾动态显像评估肾功能的临床价值[J]. 实用临床医药杂志, 2017, 21(5): 212-4. https://www.cnki.com.cn/Article/CJFDTOTAL-XYZL201705074.htm [11] Hashimoto J, Ito S. Aortic blood flow reversal determines renal function[J]. Hypertension, 2015, 66(1): 61-7. doi: 10.1161/HYPERTENSIONAHA.115.05236 [12] Hanratty R, Chonchol M, Havranek EP, et al. Relationship between blood pressure and incident chronic kidney disease in hypertensive patients[[J]. Clin J Am Soc Nephrol, 2011, 6(11): 2605-11. doi: 10.2215/CJN.02240311 [13] 阮志芹, 李华. 原发性高血压和肾功能减退的相关性[J]. 中华高血压杂志, 2017, 25(1): 22-6. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGGZ201701009.htm [14] Pathania M. Quantitative micro-albuminuria assessment from random voided urinary albumin: creatinine ratio'versus "24 hours urinary albumin concentration" for screening of diabetic nephropathy[J]. J Clin Diagn Res, 2013, 12(7): 2828-31. [15] Wu HY, Peng YS, Chiang CK, et al. Diagnostic performance of random urine samples using albumin concentration vs ratio of albumin to creatinine for microalbuminuria screening in patients with diabetes mellitus[J]. JAMA Intern Med, 2014, 174(7): 1108. doi: 10.1001/jamainternmed.2014.1363 [16] 阿不都热合满·买买提, 居热提·阿扎提, 买买提江·阿布都热西提, 等. 核素肾动态显像在高血压肾病中的应用价值[J]. 中国基层医药, 2017, 24(11): 1620-2. doi: 10.3760/cma.j.issn.1008-6706.2017.11.006 [17] Mihajlov R, Stoeva D, Pencheva B, et al. Albuminuria and glomerular filtration in patients with essential hypertension[J]. Clin Lab, 2015, 61(7/2015): 677-85. [18] 邓时素, 欧三桃, 李俊峰, 等. 动态动脉硬化指数与超声造影评估早期高血压肾损伤[J]. 实用医学杂志, 2016, 32(23): 3894-7. doi: 10.3969/j.issn.1006-5725.2016.23.025 [19] Peralta CA, Norris KC, Li SY, et al. Blood pressure components and end-stage renal disease in persons with chronic kidney disease: the Kidney Early Evaluation Program (KEEP)[J]. Arch Intern Med, 2012, 172(1): 41-7. doi: 10.1001/archinternmed.2011.619 [20] Bouvet BR, Paparella CV, Arriaga SMM, et al. Evaluation of urinary N-acetyl-beta-D-glucosaminidase as a marker of early renal damage in patients with type 2 diabetes mellitus[J]. Arq Bras Endocrinol Metab, 2014, 58(8): 798-801. doi: 10.1590/0004-2730000003010 [21] 别立莉. AFU、NAG和β2-MG联合检测对高血压早期肾损伤诊断价值的研究[J]. 中国实用医药, 2016, 11(9): 61-3. https://www.cnki.com.cn/Article/CJFDTOTAL-ZSSA201609036.htm [22] Yano Y, Fujimoto S, Kramer H, et al. Long-term blood pressure variability, new-onset diabetes mellitus, and new-onset chronic kidney disease in the Japanese general population[J]. Hypertension, 2015, 66(1): 30-6. doi: 10.1161/HYPERTENSIONAHA.115.05472 [23] 王建国, 魏斌. 99mTc-DTPA肾动态显像对高血压患者肾损害的诊断价值[J]. 现代医用影像学, 2018, 27(6): 1888-9. https://www.cnki.com.cn/Article/CJFDTOTAL-XDYY201806021.htm [24] 刘红, 岳华, 赵红娟, 等. 尿NAG、mALB、β2-MG、α1-MG检测对早期肾损害的诊断价值[J]. 西部医学, 2011, 23(2): 239-41. doi: 10.3969/j.issn.1672-3511.2011.02.014 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 92
- HTML全文浏览量: 51
- PDF下载量: 9
- 被引次数: 0