



Standardized uptake value in quantitative SPECT/CT can diagnose metastatic bone tumors
-
摘要:
目的 探讨基于最大期望值重建算法定量SPECT/CT中的标准化摄取值(SUV)在转移性骨肿瘤中的诊断价值。 方法 回顾性分析2022年3~5月在广西医科大学附属第一医院核医学科行定量SPECT/CT骨扫描的75例患者,共勾画87个骨高代谢病灶的SUV,同时勾画骨代谢正常患者的脊柱SUV作为对照组(43个脊柱椎体)。测定良性病灶、恶性病灶、对照组的最大标准化摄取值(SUVmax)、平均标准化摄取值(SUVmean)、最小标准化摄取值(SUVmin)。组间比较采用非参数检验,使用ROC曲线获得最佳阈值。 结果 以病理和/或6~12月及以上的影像学随访为判断的最终标准,诊断骨转移组病灶48个,良性病变组病灶39个,骨转移组SUV分别为SUVmax 30.15(20.75,45.43)g/mL、SUVmean 16.65(11.75,23.10)g/mL、SUVmin 11.6(8.40,15.27)g/mL,良性病变组SUV分别为SUVmax 13.5(10.4,17.5)g/mL、SUVmean 8.22(5.89,9.56)g/mL、SUVmin 5.83(2.63,6.89)g/mL,对照组SUV分别为SUVmax 7.47±1.99 g/mL、SUVmean 3.74±0.68 g/mL、SUVmin 1.06±0.46 g/mL,骨转移组SUV高于良性病变组和对照组(P<0.001);ROC曲线分析显示,SUVmax、SUVmean、SUVmin曲线下的面积分别为0.876、0.912、0.901,SUVmax截断值为26.6 g/mL时,其特异性为100%,敏感度为64.6%,当SUVmin值取8.1 g/mL时,其敏感度、特异性分别为81.2%与89.7%,SUVmean截断值为11.5 g/mL,敏感度、特异性分别为77.1%、92.3%;联合定量SPECT/CT骨融合显像+SUVmean值诊断的检出率大于常规SPECT/CT骨融合图像(χ2=11.576,P=0.001),两者的诊断符合率分别为75.86%、94.25%。 结论 定量SPECT/CT中的SUV在骨良恶性病灶的鉴别诊断中具有一定的临床应用价值,补充了对肿瘤骨转移灶和骨良性病灶的定性分析;定量SPECT/CT骨融合显像+SUVmean在诊断肿瘤骨转移的准确性高于常规SPECT/CT骨融合显像。 Abstract:Objective To investigate the diagnostic value of standardized uptake value (SUV) of quantitative SPECT/CT based on the maximum expectation reconstruction algorithm in metastatic bone tumors. Methods A total of 75 patients who underwent quantitative SPECT/CT bone scanning in the Department of Nuclear Medicine of our hospital from March to May 2022 were retrospectively analyzed. The SUV of 87 bone hypermetabolism lesions was delineated, and the SUV of the spine of patients with normal bone metabolism was delineated as the control group (43 spinal vertebrae). The maximum standardized uptake value (SUVmax), mean standardized uptake value (SUVmean) and minimum standardized uptake value (SUVmin) of benign lesions, malignant lesions and control group were measured. A non-parametric test was used for comparison between groups, and ROC curve was used to obtain the best threshold value. Results According to pathology and/or imaging follow-up of 6 to 12 months or more, 48 lesions were diagnosed as bone metastasis and 39 lesions as benign lesions. SUVmax 30.15(20.75, 45.43) g/mL, SUVmean 16.65(11.75, 23.10) g/mL, SUVmin 11.6(8.40, 15.27) g/mL in the bone metastasis group, and SUVmax 13.5(10.4, 15.27) g/mL, SUVmean 8.22(5.89, 9.56) g/mL, SUVmin 5.83(2.63, 6.89) g/mL in the benign group, while the SUVmax 7.47±1.99 g/mL, SUVmean 3.74 ± 0.68 g/mL, SUVmin 1.06 ± 0.46 g/mL in the control group, respectively. The SUV of the bone metastasis group was significantly higher than that of the benign lesion group and the control group (P < 0.001). ROC curve analysis showed that the area under the curve of SUVmax, SUVmean and SUVmin were 0.876, 0.912 and 0.901, respectively. When the cut-off value of SUVmax was 26.6 g/mL, the specificity was 100% and the sensitivity was 64.6%. When the cut-off value of SUVmin was 8.1 g/mL, the sensitivity and specificity were 81.2% and 89.7%, respectively. The cutoff value of SUVmean was 11.5 g/mL, sensitivity and specificity were 77.1% and 92.3%, respectively. The detection rate of combined quantitative SPECT/CT bone fusion imaging and SUVmean value was higher than that of conventional SPECT/CT bone fusion imaging (χ2=11.576, P=0.001), and the diagnostic coincidence rate was 75.86% and 94.25%, respectively. Conclusion The SUV of quantitative SPECT/CT has a certain clinical application value in the differential diagnosis of benign and malignant bone lesions, which complements the qualitative analysis of bone metastases and benign bone lesions. Quantitative SPECT/CT bone fusion imaging +SUVmean is more accurate than conventional SPECT/CT bone fusion imaging in the diagnosis of tumor bone metastasis. -
Key words:
- quantitative /
- SPECT/CT /
- standardized uptake value /
- metastatic bone tumor /
- bone fusion imaging
-

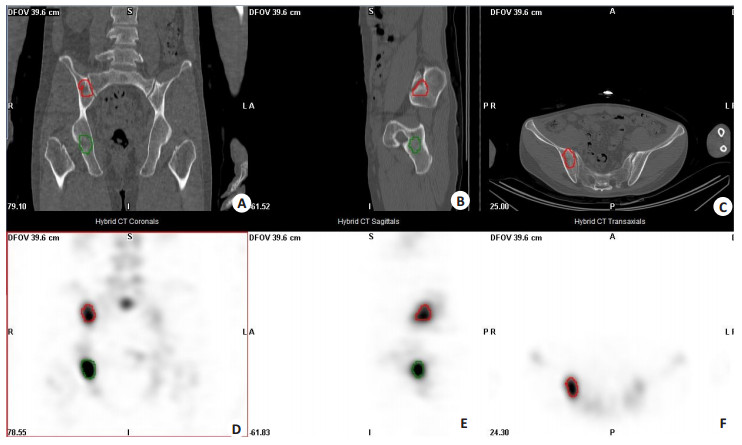
图 1 骨高代谢病变SUV勾画
Figure 1. Delineation of SUV of bone hypermetabolic lesions. A 41-year-old male patient presented with a right neck mass for more than 2 months. 99mTc-MDP whole-body bone scan revealed abnormal concentration lesions in the right ilium and the right ischium, and SPECT/CT scan showed fuzzy boundaries, irregular low-density shadow and high radionuclide uptake in the right ilium and the right ischium. The images were post-processed by workstation software (Q.Valumetrix MI Evolution for Bone), and the lesions were precisely located in the coronal, sagittal and transverse planes. The right iliac lesion (red line) and the right ischial lesion (green line) are delineated on CT (A-C) and SPECT (D-F) images, respectively. A: CT coronal plane; B: CT sagittal plane; C: CT transverse plane; D: SPECT coronal plane; E: SPECT sagittal plane; F: For SPECT cross-sectional images, the SUVmax, SUVmean, SUVmin of the right iliac lesions were 18.8, 11.7, 8.84, respectively, and the SUVmax, SUVmean, SUVmin of the right ischial lesions were 30.2, 15.8, 8.84, respectively

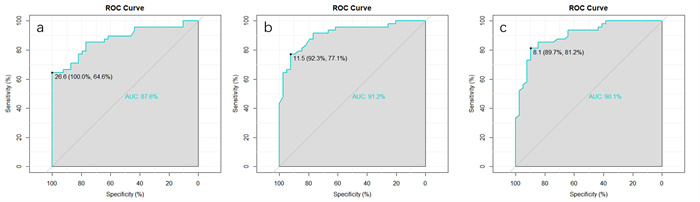
图 2 ROC曲线分析
Figure 2. ROC curve analysis. A: Diagnostic efficiency of SUVmax for bone; B: Diagnostic efficiency of SUVmean for bone; C: Diagnostic efficiency of SUVmin for bone.
表 1 SUV水平在骨转移组、良性病变组、对照组总体比较
Table 1. Comparison of SUV between the bone metastasis group, the benign lesion group and the control group
Group SUVmax SUVmean SUVmin Bone metastasis group [n=48, M(P25, P75)] 30.15(20.75, 45.43) 16.65(11.75, 23.1) 11.6(8.4, 15.27) Benig lesion group [n=39, M(P25, P75)] 13.5(10.4, 17.5) 8.22(5.89, 9.56) 5.83(2.63, 6.89) Control group (n=43, Mean±SD) 7.47±1.99 3.74±0.68 1.06±0.46 H 84.906 96.198 100.430 P <0.001 <0.001 <0.001 SUV: Standardized uptake value.  下载: 导出CSV
下载: 导出CSV
表 2 骨转移组、良性病变组中的SUV值ROC曲线分析
Table 2. ROC curve analysis of SUV value in bone metastasis group and benign lesion group
SUV value Cut off value AUC(95% CI) Sensibility (%) Specificity (%) SUVmax 26.6 0.876(0.803-0.948) 64.6 100.0 SUVmean 11.5 0.912(0.852-0.973) 77.1 92.3 SUVmin 8.1 0.901(0.838-0.965) 81.2 89.7
下载: 导出CSV
表 3 初次诊断以及随访后最终诊断
Table 3. Initial diagnosis and final diagnosis after follow-up (n)
Diagnostic results Number of lesions First diagnosis Final follow-up results Bone metastases 40 48 Benign lesion 26 39 Unascertainable 21 Total 87 87 Conventional SPECT/CT fusion imaging diagnosis for the first time.
下载: 导出CSV
表 4 常规SPECT/CT融合图像与定量SPECT/CT融合图像+SUVmean诊断比较
Table 4. Diagnostic comparison between conventional SPECT/CT fusion images and quantitative SPECT/CT fusion images +SUVmean (%)
Diagnostic method Clarify a diagnosis No definite diagnosis The overall diagnostic coincidence rate Bone metastases Benign lesion Conventional SPECT/CT fusion images 45.98(40/87) 29.88(26/87) 24.14(21/87) 75.86(66/87) Quantitative SPECT/CT fusion images +SUVmean 50.0247/87) 40.23(35/87) 5.75(5/87) 94.25(82/87) χ2 11.576 P 0.001
下载: 导出CSV
-
[1] 时红萍, 张秋宁, 刘国庆, 等. 唑来膦酸联合放射治疗治疗恶性肿瘤骨转移的Meta分析[J]. 中国循证医学杂志, 2013, 13(7): 858-67. https://www.cnki.com.cn/Article/CJFDTOTAL-ZZXZ201307016.htm [2] Coleman RE, Lipton A, Roodman GD, et al. Metastasis and bone loss: advancing treatment and prevention[J]. Cancer Treat Rev, 2010, 36(8): 615-20. doi: 10.1016/j.ctrv.2010.04.003 [3] 赵辉, 安建平, 徐晓红, 等. 放射性核素骨显像联合PSA、fPSA、fPSA/tPSA评价前列腺癌骨转移[J]. 放射免疫学杂志, 2011, 24(2): 176-8. doi: 10.3969/j.issn.1008-9810.2011.02.029 [4] Shie P, Cardarelli R, Brandon D, et al. Meta-analysis: comparison of F-18 fluorodeoxyglucose-positron emission tomography and bone scintigraphy in the detection of bone metastases in patients with breast cancer[J]. Clin Nucl Med, 2008, 33(2): 97-101. doi: 10.1097/RLU.0b013e31815f23b7 [5] Caglar M, Kupik O, Karabulut E, et al. Detection of bone metastases in breast cancer patients in the PET/CT era: do we still need the bone scan?[J]. Revista Española De Med Nucl E Imagen Mol, 2016, 35(1): 3-11. doi: 10.1016/j.remn.2015.08.006 [6] Chen XL, Li Q, Cao L, et al. Diagnostic role of (99)Tc(m)-MDP SPECT/CT combined SPECT/MRI Multi modality imaging for early and atypical bone metastases[J]. Int J Clin Exp Med, 2014, 7 (12): 5336-41. [7] 杜芬, 罗小毛, 刘明, 等. 定量SPECT/CT(SUVmax)在骨良恶性病灶中的鉴别诊断及增益价值[J]. 分子影像学杂志, 2021, 44(3): 435-40. doi: 10.12122/j.issn.1674-4500.2021.03.04 [8] 龚成鹏, 李坤, 胡佳, 等. 锝-99m定量SPECT/CT临床应用进展[J]. 华中科技大学学报: 医学版, 2021, 50(2): 247-50, 265. https://www.cnki.com.cn/Article/CJFDTOTAL-TJYX202102022.htm [9] Shcherbinin S, Celler A, Belhocine T, et al. Accuracy of quantitative reconstructions in SPECT/CT imaging[J]. Phys Med Biol, 2008, 53 (17): 4595-604. doi: 10.1088/0031-9155/53/17/009 [10] Zeintl J, Vija AH, Yahil A, et al. Quantitative accuracy of clinical 99mTc SPECT/CT using ordered-subset expectation maximization with 3-dimensional resolution recovery, attenuation, and scatter correction[J]. J Nucl Med, 2010, 51(6): 921-8. doi: 10.2967/jnumed.109.071571 [11] Mairal E, Imbert L, Marie PY, et al. Three-phase bone quantitativeSPECT of navicular bones with a high-sensitivity whole-body CZT-camera in a Müeller-Weiss syndrome[J]. Eur J Nucl Med Mol Imaging, 2022, 49(9): 3295-6. doi: 10.1007/s00259-022-05733-9 [12] 翟威豪, 何薇. 定量99mTc-MDP SPECT/CT在老年骨质疏松性压缩骨折中的诊断价值[J]. 分子影像学杂志, 2022, 45(4): 542-5. doi: 10.12122/j.issn.1674-4500.2022.04.13 [13] 邹成富. CT联合全身骨显像在骨转移瘤中的诊断效果分析[J]. 现代医学与健康研究电子杂志, 2018(17): 83-4. https://www.cnki.com.cn/Article/CJFDTOTAL-XYJD201817053.htm [14] 许阿磊, 徐慧琴, 汪会, 等. 精准定量SPECT/CT在乳腺癌骨转移诊断和疗效评价中的应用[J]. 肿瘤影像学, 2020, 29(2): 169-74. https://www.cnki.com.cn/Article/CJFDTOTAL-YXYX202002020.htm [15] 李中恩, 程爱萍. CT联合全身骨显像在骨转移瘤中的诊断价值[J]. 中国药物与临床, 2019, 19(14): 2372-3. https://www.cnki.com.cn/Article/CJFDTOTAL-YWLC201914017.htm [16] Schaap J, de Groot JAH, Nieman K, et al. Added value of hybrid myocardial perfusion SPECT and CT coronary angiography in the diagnosis of coronary artery disease[J]. Eur Heart J Cardiovasc Imaging, 2014, 15(11): 1281-8. doi: 10.1093/ehjci/jeu135 [17] 代迪, 郝吉庆. 30例消化道肿瘤骨转移患者的定量SPECT/CT显像分析[J]. 现代肿瘤医学, 2021, 29(19): 3415-9. https://www.cnki.com.cn/Article/CJFDTOTAL-SXZL202119019.htm [18] Tanaka K, Norikane T, Mitamura K, et al. Quantitative 99mTc-MDP SPECT/CT correlated with 18F-NaF PET/CT for bone metastases in patients with prostate cancer[J]. EJNMMI physics, 2022, 9(1): 83. doi: 10.1186/s40658-022-00513-8 [19] Arvola S, Jambor I, Kuisma A, et al. Comparison of standardized uptake values between 99mTC-HDP SPECT/CT and 18F-NaF PET/CT in bone metastases of breast and prostate cancer[J]. EJNMMI Res, 2019, 9(1): 1-9. doi: 10.1186/s13550-018-0470-9 [20] Beck M, Sanders JC, Ritt P, et al. Longitudinal analysis of bone metabolism using SPECT/CT and 99mTc-diphosphono-propanedicarboxylic acid: comparison of visual and quantitative analysis[J]. EJNMMI Res, 2016, 6(1): 60. doi: 10.1186/s13550-016-0217-4 [21] Suh MS, Lee WW, Kim YK, et al. Maximum standardized uptake value of 99m hydroxymethylene diphosphonate SPECT/CT for the evaluation of temporomandibular joint disorder[J]. Radiology, 2016, 280(3): 890-6. doi: 10.1148/radiol.2016152294 [22] Umeda T, Koizumi M, Fukai S, et al. Evaluation of bone metastatic burden by bone SPECT/CT in metastatic prostate cancer patients: defining threshold value for total bone uptake and assessment in radium-223 treated patients[J]. Ann Nucl Med, 2018, 32(2): 105-13. [23] 曾丽妹, 张昊, 吴家文, 等. 肿瘤患者SPECT/CT骨显像中SUV定量对骨关节炎与骨转移的诊断价值[J]. 中国骨与关节杂志, 2022, 11 (2): 152-7. https://www.cnki.com.cn/Article/CJFDTOTAL-GZGL202202015.htm [24] 王海岩, 赵军, 孟庆元, 等. SPECT/CT融合骨显像中SUVmax测定对肿瘤患者肋骨转移灶的诊断价值[J]. 肿瘤影像学, 2017, 26(5): 318-21. https://www.cnki.com.cn/Article/CJFDTOTAL-YXYX201705002.htm [25] Ryoo HG, Lee WW, Kim JY, et al. Minimum standardized uptake value from quantitative bone single-photon emission computed tomography/computed tomography for evaluation of femoral head viability in patients with femoral neck fracture[J]. Nucl Med Mol Imaging, 2019, 53(4): 287-95. [26] Flavian T, Mario J, Niklaus S, et al. Quantitative bone SPECT/CT: high specificity for identification of prostate cancer bone metastases[J]. BMC Musculoskelet Disord, 2019, 20(1): 619. [27] 黄克敏, 冯彦林, 梁伟棠, 等. 不同重建算法及有序子集最大期望值法重建参数对SPECT/CT定量计算结果的影响[J]. 中国医学影像技术, 2018, 34(1): 103-8. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYXX201801040.htm -

 点击查看大图
点击查看大图
计量
- 文章访问数: 206
- HTML全文浏览量: 62
- PDF下载量: 17
- 被引次数: 0