



Clinical effect of high- intensity focused ultrasound ablation on adenomyosis and its influence on serum CA125 of patients
-
摘要:
目的 探讨高强度聚焦超声(HIFU)消融子宫腺肌病的疗效及对患者血清糖类抗原125(CA125)的影响。 方法 选取2020年12月~2021年12月本院收治的73例子宫腺肌病患者,均行HIFU治疗。根据患者术后情况对HIFU治疗进行有效性评价。比较患者术前及术后1、3、6月的痛经评分、经量评分,测量子宫及腺肌病灶的体积及患者血清CA125水平变化。术后随访6月,记录不良反应和复发情况。 结果 73例子宫腺肌病患者中,治疗显效患者22例(30.14%),治疗有效47例(64.38%),总有效率为94.52%。患者术后1、3、6月的痛经评分、经量评分、病灶体积和子宫体积均低于术前(P < 0.05)。术后1、3、6月随访中,患者痛经评分、经量评分和病灶体积的差异均有统计学意义(P < 0.05),但患者的子宫体积变化无统计学意义(P > 0.05)。术后1、3、6月随访中,患者血清CA125水平逐渐降低,趋于正常(P < 0.05)。患者术后IgA、IgM、补体C3、C4和Th17/Treg比值均低于术前,IgG水平高于术前(P < 0.05)。术后随访6月,患者不良反应总发生率为10.96%,2例(2.74%)患者复发。 结论 HIFU消融治疗可有效缓解子宫腺肌病患者痛经等临床症状、缩小病灶体积,同时不良反应率和复发率较低,是一种安全有效的治疗方法。在使用HIFU治疗时可检测患者CA125水平变化,为判定子宫腺肌病患者疗效评价提供参考。 Abstract:Objective To investigate the efficacy of high-intensity focused ultrasound (HIFU) in ablation of adenomyosis, and its influence on serum CA125. Methods From December 2020 to December 2021, 73 patients with adenomyosis were treated with HIFU. The effectiveness of HIFU treatment according to the postoperative condition of patients was evaluated. The dysmenorrhea score and menstrual flow score were compared before operation and 1, 3, 6 months after operation. The volume of uterine and glandular muscle lesions was measured, and the change of serum CA125 level was observed. All patients were followed up for 6 months, and the occurrence and recurrence of adverse reactions were recorded. Results Among the 73 patients of adenomyosis, 22 patients (30.14%) were markedly effective and 47 patients (64.38%) were effective, with a total effective rate of 94.52%. After 1, 3 and 6 months, the dysmenorrhea score, menstrual flow score, lesion volume and uterus volume were lower than those before operation (P < 0.05). After 1, 3 and 6 months follow-up, there were statistical differences in dysmenorrhea score, menstrual flow score and lesion volume (P < 0.05), but there was no statistical difference in uterine volume (P > 0.05), and the level of serum CA125 gradually decreased and became normal (P < 0.05). After operation, IgA, IgM, complement C3, C4 and Th17/Treg ratio were lower than those before operation, but IgG level was higher than that before operation (P < 0.05). After 6 months of follow- up, the total incidence of adverse reactions was 10.96%, and 2 patients (2.74%) recurred. Conclusion HIFU ablation can effectively relieve the clinical symptoms such as dysmenorrhea in patients with adenomyosis, reduce the volume of the lesion, and reduce the adverse reaction rate and recurrence rate. It is a safe and effective method to treat adenomyosis. When HIFU is used, the change of CA125 level can be detected, which can provide reference for evaluating the curative effect of patients with adenomyosis. -
Key words:
- adenomyosis of uterus /
- high-intensity focused ultrasound /
- CA125 /
- efficacy evaluation
-

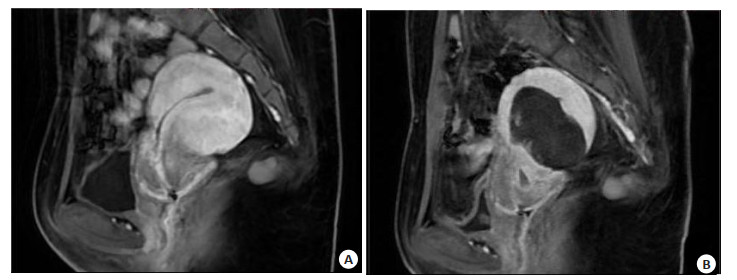
图 1 患者HIFU治疗前后对比图
Figure 1. Comparison of patients before and after HIFU treatment. A: MRI examination before HIFU showed that the patient's lesion was located in the anterior wall of uterus, showing low signal intensity on T2WI; B: MRI examination after HIFU showed a slightly high signal on T2WI of the patient's focus, and no obvious enhancement was found in the enhanced scan.
表 1 患者一般资料
Table 1. General data of patients (n=73)
Index Value Age (years, Mean±SD) 37.15±5.28 Focus volume (cm3, Mean±SD) 37.92±6.87 Number of lesions [n(%)] Single shot 67(91.78) Multiple shots 6(8.22) Uterine position [n(%)] Front 58(79.45) Middle 4(5.48) Back 11(15.07) Location of focus [n(%)] Antetheca 9(12.33) Paries posterior 51(69.86) Palace bottom 13(18.81) Uterine volume (cm3, Mean±SD) 183.29±30.27 Dysmenorrhea score (point, Mean±SD) 8.14±1.96 Menstrual volume score(point, Mean±SD) 4.31±0.95 Total energy of HIFU treatment (kJ, Mean±SD) 297.82±26.79 HIFU: High-intensity focused ultrasound.  下载: 导出CSV
下载: 导出CSV
表 2 患者手术前后痛经、经量评分比较
Table 2. Comparison of dysmenorrhea and menstrual volume scores before and after operation (score, n=73, Mean±SD)
Time Dysmenorrhea score Menstrual volume score Preoperative 8.14±1.96 4.31±0.95 1 month after operation 6.43±1.49a 3.54±0.71a 3 months after operation 4.81±1.14ab 3.02±0.53ab 6months after operation 2.27±0.57abc 2.21±0.39abc aP < 0.05 vs preoperative; bP < 0.05 vs 1 month after operation; cP < 0.05 vs 3 months after operation.
下载: 导出CSV
表 3 患者手术前后病灶体积和子宫体积变化
Table 3. Changes of focus volume and uterine volume before and after operation (cm3, n=73, Mean±SD)
Time Focus volume Uterine volume Preoperative 37.92±6.87 183.29±30.27 1 month after operation 28.51±4.92a 171.82±25.36a 3 months after operation 22.34±3.07ab 165.27±23.38a 6 months after operation 18.93±2.24abc 161.73±22.19a aP < 0.05 vs preoperative; bP < 0.05 vs 1 month after operation; cP < 0.05 vs 3 months after operation.
下载: 导出CSV
表 4 患者手术前后免疫功能比较
Table 4. Comparison of immune function of patients before and after operation (n=73, Mean±SD)
Time IgA(g/L) IgG(g/L) IgM(g/L) C3(mg/dL) C4(mg/dL) Th17/treg Preoperative 3.71±0.59 11.83±1.27 1.52±0.37 105.84±5.91 25.08±3.89 0.42±0.04 Postoperative 3.04±0.41 14.69±1.41 1.05±0.21 91.57±4.46 19.94±3.50 0.36±0.07 t 7.968 12.877 9.439 16.467 8.392 6.359 P < 0.001 < 0.001 < 0.001 < 0.001 < 0.001 < 0.001
下载: 导出CSV
-
[1] Szubert M, Koziróg E, Olszak O, et al. Adenomyosis and infertility-review of medical and surgical approaches[J]. Int J Environ Res Public Health, 2021, 18(3): 1235. doi: 10.3390/ijerph18031235 [2] Upson K, Missmer SA. Epidemiology of adenomyosis[J]. Semin Reprod Med, 2020, 38(2/03): 89-107. doi: 10.1055/s-0040-1718920 [3] Van den Bosch T, Van Schoubroeck D. Ultrasound diagnosis of endometriosis and adenomyosis: state of the art[J]. Best Pract Res Clin Obstet Gynaecol, 2018, 51: 16-24. doi: 10.1016/j.bpobgyn.2018.01.013 [4] Pontis A, D'Alterio MN, Pirarba S, et al. Adenomyosis: a systematic review of medical treatment[J]. Gynecol Endocrinol, 2016, 32(9): 696-700. doi: 10.1080/09513590.2016.1197200 [5] 巫小燕. 腹腔镜治疗子宫内膜异位症的疗效及预后影响因素分析[J]. 川北医学院学报, 2018, 33(2): 217-9. https://www.cnki.com.cn/Article/CJFDTOTAL-NOTH201802019.htm [6] Lacheta J. Uterine adenomyosis: pathogenesis, diagnostics, symp-tomatology and treatment[J]. Ceska Gynekol, 2019, 84(3): 240-6. [7] Quadri SA, Waqas M, Khan I, et al. High-intensity focused ultrasound: past, present, and future in neurosurgery[J]. Neurosurg Focus, 2018, 44(2): E16. doi: 10.3171/2017.11.FOCUS17610 [8] Bachu VS, Kedda J, Suk I, et al. High-intensity focused ultrasound: a review of mechanisms and clinical applications[J]. Ann Biomed Eng, 2021, 49(9): 1975-91. doi: 10.1007/s10439-021-02833-9 [9] Chen Q, Li YW, Wang S, et al. Clinical manifestations of adenomyosis patients with or without pain symptoms[J]. J Pain Res, 2019, 12: 3127-33. doi: 10.2147/JPR.S212117 [10] 徐玲玲, 陈炳香, 陈媛媛, 等. 血清人附睾蛋白4、CA125与阴道超声联合诊断对子宫腺肌病的预测价值分析[J]. 生殖医学杂志, 2021, 30 (1): 94-8. https://www.cnki.com.cn/Article/CJFDTOTAL-SZYX202101018.htm [11] Hirata T, Izumi G, Takamura M, et al. Efficacy of dienogest in the treatment of symptomatic adenomyosis: a pilot study[J]. Gynecol Endocrinol, 2014, 30(10): 726-9. doi: 10.3109/09513590.2014.926882 [12] 李乐萍, 周夫群. 高强度聚焦超声对子宫腺肌病有效性安全性及生活质量的影响[J]. 中国妇幼保健, 2021, 36(12): 2905-8. https://www.cnki.com.cn/Article/CJFDTOTAL-ZFYB202112070.htm [13] Harada T, Khine YM, Kaponis A, et al. The impact of adenomyosis on women's fertility[J]. Obstet Gynecol Surv, 2016, 71(9): 557-68. doi: 10.1097/OGX.0000000000000346 [14] Antero MF, Ayhan A, Segars J, et al. Pathology and pathogenesis of adenomyosis[J]. Semin Reprod Med, 2020, 38(2/03): 108-18. doi: 10.1055/s-0040-1718922 [15] 艾星子·艾里, 郭铮宇, 张晓霏. 子宫腺肌病高强度聚焦超声消融治疗研究进展[J]. 山东大学学报: 医学版, 2022, 60(7): 36-42. https://www.cnki.com.cn/Article/CJFDTOTAL-SDYB202207006.htm [16] Osada H. Uterine adenomyosis and adenomyoma: the surgical approach[J]. Fertil Steril, 2018, 109(3): 406-17. doi: 10.1016/j.fertnstert.2018.01.032 [17] Duc NM, Keserci B. Emerging clinical applications of high-intensity focused ultrasound[J]. Diagn Interv Radiol, 2019, 25(5): 398-409. doi: 10.5152/dir.2019.18556 [18] Zhang L, Rao FW, Setzen R. High intensity focused ultrasound for the treatment of adenomyosis: selection criteria, efficacy, safety and fertility[J]. Acta Obstet Gynecol Scand, 2017, 96(6): 707-14. doi: 10.1111/aogs.13159 [19] 蒋静, 周洪贵, 陈燕, 等. 高强度聚焦超声联合促性腺激素释放激素激动剂治疗子宫腺肌症的前瞻性研究[J]. 重庆医学, 2019, 48(10): 1705-8. https://www.cnki.com.cn/Article/CJFDTOTAL-CQYX201910020.htm [20] 胡红, 许芙蓉, 但汉丽, 等. 超声造影评价高强度聚焦超声消融治疗子宫肌瘤疗效的价值[J]. 川北医学院学报, 2019, 34(3): 363-6, 374. https://www.cnki.com.cn/Article/CJFDTOTAL-NOTH201903011.htm [21] Zhai JY, Vannuccini S, Petraglia F, et al. Adenomyosis: mecha-nisms and pathogenesis[J]. Semin Reprod Med, 2020, 38(2/03): 129-43. doi: 10.1055/s-0040-1716687 [22] 冯磊明, 郝世辉. 子宫血流超声参数与高强度聚焦超声消融子宫腺肌病疗效的相关性[J]. 广东医学, 2022, 43(4): 487-91. https://www.cnki.com.cn/Article/CJFDTOTAL-GAYX202204018.htm [23] Zhou Y, Ji X, Niu J, et al. Ultrasound-guided high-intensity focused ultrasound for devascularization of uterine fibroid: a feasibility study[J]. Ultrasound Med Biol, 2021, 47(9): 2622-35. doi: 10.1016/j.ultrasmedbio.2021.05.012 [24] Bourdon M, Santulli P, Marcellin L, et al. Physiopathologie de l' adénomyose: une énigme non résolue[J]. Gynécologie Obstétrique Fertil Sénologie, 2022, 50(2): 182-8. doi: 10.1016/j.gofs.2021.10.005 [25] 张培荣, 槐中美, 廖子龙, 等. 免疫调节细胞Th17/Treg及程序性死亡配体1在子宫腺肌病中的意义[J]. 中国计划生育学杂志, 2019, 27 (6): 768-71. https://www.cnki.com.cn/Article/CJFDTOTAL-JHSY201906023.htm [26] Bourdon M, Santulli P, Chouzenoux S, et al. The disease phenotype of adenomyosis-affected women correlates with specific serum cytokine profiles[J]. Reproductive Sci, 2019, 26(2): 198-206. [27] Zhang M, Cheng S, Jin Y, et al. Roles of CA125 in diagnosis, prediction, and oncogenesis of ovarian cancer[J]. Biochim Biophys Acta BBA Rev Cancer, 2021, 1875(2): 188503. [28] 江烨伶. 血清STIP-1、CA125a和CA125b诊断子宫腺肌病的临床价值[J]. 检验医学与临床, 2021, 18(8): 1097-100. https://www.cnki.com.cn/Article/CJFDTOTAL-JYYL202108019.htm [29] Jiang CX, Liu C, Guo J, et al. CA125 modified by PLT and NLR improves the predictive accuracy of adenomyosis-derived pelvic dense adhesion[J]. Medicine, 2017, 96(19): e6880. [30] 杨进军, 鲁辛健, 王晓燕, 等. 磁共振动态增强扫描与弥散加权成像结合血清Ca125对高强度聚焦超声治疗子宫腺肌病的疗效评价[J]. 中华保健医学杂志, 2022, 24(4): 325-8. https://www.cnki.com.cn/Article/CJFDTOTAL-JFJB202204020.htm [31] Tang Y, Yang MT, Xiang RM, et al. Preoperative CA125 as a risk factor for symptom recurrence of adenomyosis after ultrasound-guided high-intensity focused ultrasound ablation surgery[J]. Int J Hyperth, 2022, 39(1): 1164-9. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 93
- HTML全文浏览量: 108
- PDF下载量: 5
- 被引次数: 0