



Value of medical thoracoscopy and CT-guided needle biopsy in the diagnosis of malignant pleural effusion
-
摘要:
目的 探讨内科胸腔镜与CT引导下穿刺活检诊断恶性胸腔积液的价值。 方法 选择2019年1月~2022年2月我院收治的104例不明原因胸腔积液患者,其中49例接受局麻下内科胸腔镜活检作为胸腔镜组,55例接受CT引导下胸腔病变经皮穿刺活检作为CT引导组。统计两组患者经不同诊断方式活检次数、一次活检成功率和取材成功率,比较两种方案诊断恶性胸腔积液的准确率,观察内科胸腔镜及胸部CT扫描病变征象,并对比两组患者对检查的耐受性和并发症发生率。 结果 胸腔镜组一次成功率和取材成功率均高于CT引导组(P < 0.05)。两种方式诊断恶性胸腔积液及病理类型(恶性间皮瘤、肺腺癌、肺鳞癌、肺小细胞癌、乳腺癌、结核)的准确率差异均无统计学意义(P > 0.05)。49例行内科胸腔镜扫描的患者中有36例可见胸膜粘连(73.47%),2例可见胸膜增厚(4.08%),44例可见结节样病变(89.80%)。55例行胸部CT扫描的患者中有34例可见胸膜粘连(61.82%),3例可见胸膜增厚(5.45%),51例可见结节样病变(92.73%)。两组手术耐受性和并发症总发生率差异均无统计学意义(P > 0.05)。 结论 内科胸腔镜与CT引导下穿刺活检诊断恶性胸腔积液的价值相当,术后并发症和舒适度无差异,但内科胸腔镜活检方案活检及取材成功率更高,临床推广价值更大。 Abstract:Objective To explore the value of medical thoracoscopy and CT-guided needle biopsy in the diagnosis of malignant pleural effusion. Methods A total of 104 patients with unexplained pleural effusion who were treated in the hospital were selected from January 2019 to February 2022. Among the patients, 49 cases who received medical thoracoscopy biopsy under local anesthesia were included in thoracoscopy group, and 55 cases who underwent CT-guided percutaneous puncture biopsy of thoracic lesions were inclded in CT-guided group. The number of biopsies, success rate of one-time biopsy and success rate of material sampling in the two groups of patients by different diagnostic methods were counted, and the accuracy rates of the two methods for diagnosing malignant pleural effusion were compared. The lesion signs under medical thoracoscopy and chest CT scan were observed, and the tolerance of examination and incidence rates of complications were compared between the two groups. Results The one-time success rate and success rate of material sampling in thoracoscopy group were higher than those in CT-guided group (P < 0.05). There were no significant differences in the accuracy rates of the two methods in the diagnosis of malignant pleural effusion and pathological types (malignant mesothelioma, lung adenocarcinoma, lung squamous cancer, lung small cell carcinoma, breast cancer, tuberculosis) (P > 0.05). Among the 49 patients who underwent medical thoracoscopy, pleural adhesion was seen in 36 cases (73.47%), pleural thickening was seen in 2 cases (4.08%) and nodular lesion was seen in 44 cases (89.80%). Among the 55 patients receiving chest CT scan, 34 cases (61.82%) of pleural adhesion, 3 cases (5.45%) of pleural thickening and 51 cases (92.73%) of nodular lesion were seen. The differences in surgical tolerance and total incidence rate of complications between the two groups were not significant (P > 0.05). Conclusion The value of medical thoracoscopy and CT- guided needle biopsy in the diagnosis of malignant pleural effusion is comparable. There are no differences in postoperative complications and comfort. Medical thoracoscopy has higher success rates of biopsy and material sampling and greater clinical promotion value. -
Key words:
- medical thoracoscopy /
- computed tomography /
- needle biopsy /
- malignant pleural effusion /
- diagnosis
-

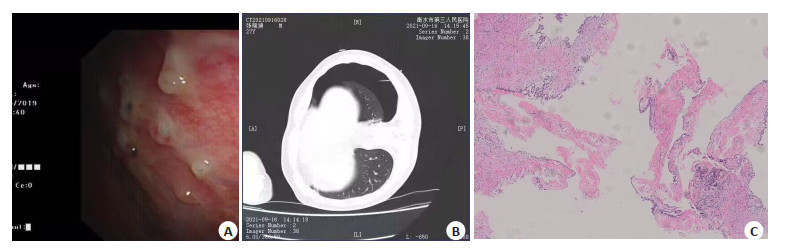
图 1 恶性胸腔积液典型病例图像
Figure 1. Images of a typical case of malignant pleural effusion. Pleural biopsy revealed chronic inflammation of proliferative fibrous tissue with epithelioid cell hyperplasia; Pleural biopsy combined with immunohistochemistry considered the possibility of mesothelioma consistent with the origin of mesothelial cell. A: Chest CT showed a large pleural effusion on the left side with atelectasis; B: Thoracoscopic parietal pleura with scattered nodular neoorganisms locally fused into patches, with rough surface and easy biopsy; C: Immunohistochemical staining showed Ki-67(+20%), P53(+), CK5/6(+), TTF-1(-), Calretinin(+), WT-1(+), CK7 (+).
表 1 两种诊断方式活检次数及取材成功率比较
Table 1. Comparison of number of biopsies and success rate of material sampling between the two diagnostic methods
Diagnostic method Cases of biopsies (n) Success rate of one-time biopsy [n(%)] Success rate of material sampling [n(%)] Medical thoracoscopy biopsy (n=49) 50 48(97.96) 49(100.00) CT-guided needle biopsy (n=55) 60 50(90.91) 50(90.91) χ2 4.502 4.680 P 0.034 0.031  下载: 导出CSV
下载: 导出CSV
表 2 两种诊断方式病理结果比较
Table 2. Comparison of pathological results between the two diagnostic methods (n)
Diagnostic method Gold standard Malignant pleural effusion Non-malignant pleural effusion Total Medical thoracoscopy Malignant pleural effusion 47 1 48 Non-malignant pleural effusion 2 1 3 Total 49 2 51 CT-guided biopsy Malignant pleural effusion 45 4 49 Non-malignant pleural effusion 5 1 6 Total 50 5 55
下载: 导出CSV
表 3 两种诊断方式准确率比较
Table 3. Comparison of accuracy rate between the two diagnostic methods
Method Sensitivity (%) Specificity (%) Accuracy rate (%) Positive predictive value (%) Negative predictive value (%) Kappa value Medical thoracoscopy 95.92 50.00 94.12 97.92 33.33 0.370 CT-guided biopsy 90.00 20.00 83.64 91.84 16.67 0.092
下载: 导出CSV
表 4 两种诊断方式病理类型比较
Table 4. Comparison of pathological types between the two diagnostic methods [n(%)]
Pathological type Medical thoracoscopy(n=49) CT-guided biopsy(n=50) χ2 P Malignant mesothelioma 5/5(100.00) 2/2(100.00) - - Lung adenocarcinoma 34/35(97.14) 28/34(82.35) 0.380 0.538 Lung squamous cancer 3/4(75.00) 5/6(83.33) 0.104 0.747 Lung small cell carcinoma 1/1(100.00) 1/2(50.00) 0.750 0.386 Breast cancer 2/2(100.00) 1/1(100.00) - - Tuberculosis 1/2(50.00) 4/5(80.00) 0.630 0.427
下载: 导出CSV
表 5 内科胸腔镜及胸部CT扫描影像学特征
Table 5. Imaging characteristics of medical thoracoscopy and chest CT scan [n(%)]
Imaging examination Pleural adhesion Pleural thickening Nodular lesion Medical thoracoscopy (n=49) 36(73.47) 2(4.08) 44(89.80) Chest CT scan (n=55) 34(61.82) 3(5.45) 51(92.73)
下载: 导出CSV
表 6 两种诊断方式并发症发生率比较
Table 6. Comparison of incidence rates of complications between the two diagnostic methods [n(%)]
Group Surgical tolerance Complications Intraoperative mild pain Postoperative wound pain postoperative chest pain Total incidence rate Postoperative fever Surgical infection Pneumothorax Pleural reaction Total incidence rate Thoracoscopy (n=49) 1(2.01) 0(0) 0(0) 1(2.04) 1(2.04) 0(0) 1(2.04) 1(2.04) 3(6.12) CT-guided (n=55) 2(3.64) 2(3.64) 1(1.82) 5(9.09) 1(1.82) 1(1.82) 1(1.82) 2(3.64) 5(9.09) χ2 2.369 0.322 P 0.124 0.571
下载: 导出CSV
-
[1] Huang ZY, Shao MM, Zhang JC, et al. Single-cell analysis of diverse immune phenotypes in malignant pleural effusion[J]. Nat Commun, 2021, 12(1): 6690. doi: 10.1038/s41467-021-27026-9 [2] Walker SP, Bintcliffe O, Keenan E, et al. Randomised trial of indwelling pleural catheters for refractory transudative pleural effusions[J]. Eur Respir J, 2022, 59(2): 2101362. doi: 10.1183/13993003.01362-2021 [3] 何司琪, 张言斌. 胸膜活检术联合胸水结核T淋巴细胞斑点试验对结核性胸腔积液的诊断价值[J]. 临床肺科杂志, 2021, 26(3): 428-31. https://www.cnki.com.cn/Article/CJFDTOTAL-LCFK202103024.htm [4] 付鹏, 龙发, 胡斯育, 等. 经内科胸腔镜冷冻胸膜活检对不明原因胸腔积液诊断的有效性及安全性研究[J]. 临床肺科杂志, 2021, 26(5): 649-53. https://www.cnki.com.cn/Article/CJFDTOTAL-LCFK202105001.htm [5] 中国恶性胸腔积液诊断与治疗专家共识组. 恶性胸腔积液诊断与治疗专家共识[J]. 中华内科杂志, 2014, 53(3): 252-6. https://www.cnki.com.cn/Article/CJFDTOTAL-SYNK201408009.htm [6] Zhou Z, Li HQ, Hu DQ, et al. Clinical efficacy of bevacizumab combined with cisplatin in the treatment of malignant pleural effusion and ascites caused by lung cancer: a randomized trial[J]. Ann Palliat Med, 2021, 10(10): 10575-83. doi: 10.21037/apm-21-2623 [7] 贾敬周, 祁敏现, 巴玉峰, 等. 胸腔镜检联合细胞学快速现场评估在不明胸腔积液诊断中的临床研究[J]. 中国临床医生杂志, 2020, 48(1): 69-71. https://www.cnki.com.cn/Article/CJFDTOTAL-ZLYS202001021.htm [8] 李磊, 倪正义, 汤中文, 等. 三种活检方法对不明原因的渗出性胸腔积液的诊断价值[J]. 临床与病理杂志, 2017, 37(8): 1623-8. https://www.cnki.com.cn/Article/CJFDTOTAL-WYSB201708013.htm [9] Psallidas I, Hassan M, Yousuf A, et al. Role of thoracic ultrasonography in pleurodesis pathways for malignant pleural effusions (SIMPLE): an open-label, randomised controlled trial[J]. Lancet Respir Med, 2022, 10(2): 139-48. [10] 熊天波, 宁燕, 陈瑜莉, 等. 超声联合胸腔镜在胸腔积液良恶性诊断中的价值[J]. 分子影像学杂志, 2021, 44(3): 512-5. doi: 10.12122/j.issn.1674-4500.2021.03.19 [11] 阳苑, 胡明明, 鲁葆华, 等. 恶性胸膜间皮瘤合并肺结核/结核性胸腔积液的临床特征分析[J]. 国际呼吸杂志, 2021, 41(2): 133-7. [12] 常俊琦, 乔英. 胸部CT胸膜区病变征象在鉴别良恶性胸腔积液中的价值[J]. 现代肿瘤医学, 2022, 30(9): 1648-52. https://www.cnki.com.cn/Article/CJFDTOTAL-SXZL202209023.htm [13] 朱新程, 王炯. 内科胸腔镜对不明原因胸腔积液诊断价值及恶性胸腔积液镜下表型特征[J]. 临床肺科杂志, 2019, 24(3): 491-4. https://www.cnki.com.cn/Article/CJFDTOTAL-LCFK201903028.htm [14] 赵凡杰, 候飞飞, 樊芳芳, 等. 结核性与恶性胸腔积液内科胸腔镜下特征比较及诊断相关因素分析[J]. 国际呼吸杂志, 2020, 40(9): 651-5. [15] 周小伟, 曾茄, 万志渝, 等. 全胸腔镜肺叶切除术患者术前CT检查结果与中转开胸的关系: 871例肺部占位性病变患者前瞻性研究[J]. 分子影像学杂志, 2021, 44(1): 47-52. doi: 10.12122/j.issn.1674-4500.2021.01.09 [16] 沈德培, 吕莉萍, 李晔. 可曲式内科胸腔镜在结核性胸腔积液及恶性胸腔积液鉴别诊断中的应用及镜下特点分析[J]. 临床肺科杂志, 2022, 27(8): 1153-7. https://www.cnki.com.cn/Article/CJFDTOTAL-LCFK202208005.htm [17] 冉燕, 张建勇, 赵建军. 内科胸腔镜胸膜活检联合GeneXpert MTB/ RIF对结核性胸膜炎的诊断价值研究[J]. 中国呼吸与危重监护杂志, 2020, 19(1): 12-5. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGHW202001003.htm -

 点击查看大图
点击查看大图
计量
- 文章访问数: 81
- HTML全文浏览量: 46
- PDF下载量: 5
- 被引次数: 0