



Evaluation of left ventricular work in patients with different rheumatic immunological diseases using pressure strain loop technique
-
摘要:
目的 应用压力-应变环技术评估不同风湿免疫病患者的左心室做功状况。 方法 前瞻性选择于2021年4月~2022年11月于扬州大学附属医院确诊的风湿免疫病患者171例,按照疾病类别分为系统性红斑狼疮组30例、强直性脊柱炎组33例、干燥综合征组35例、类风湿关节炎组43例、痛风组30例,病程均≤5年;另选取同期健体检者32例为对照组。所有参与者均行常规超声心动图采集图像, 线下ECHOPAC分析得出压力-应变环参数;分析各组之间常规参数及心肌做功之间的相关性,评估左室心肌做功状况。 结果 与对照组相比,风湿免疫疾病组的A值均增高、E/A比值均降低(P < 0.05);系统性红斑狼疮组及干燥综合征组的E值降低,差异有统计学意义(P < 0.05)。所有风湿免疫疾病组的整体无效做功高于对照组,整体做功效率低于对照组(P < 0.05);系统性红斑狼疮组及强直性脊柱炎组的整体纵向应变、整体做功指数、整体有效做功低于对照组,类风湿关节炎组的整体纵向应变、整体做功指数低于对照组,痛风组的整体做功指数低于对照组,差异有统计学意义(P < 0.05)。风湿免疫疾病组的整体纵向应变绝对值、左室射血分数、E/A比值与整体做功指数、整体有效做功、整体做功效率之间呈正相关关系,与整体无效做功呈负相关关系(P < 0.01)。 结论 压力-应变环能够有效评估风湿免疫病患者左心室心肌做功状况, 将更客观的为临床提供新的诊断依据。 Abstract:Objective To evaluate left ventricular work in patients with different rheumatic immune diseases using pressure-strain loop technique. Methods We prospectively selected 171 patients with rheumatic immune diseases diagnosed in the Affiliated Hospital of Yangzhou University from April 2021 to November 2022. The patients were divided into systemic lupus erythematosus group (n=30), ankylosing spondylitis group (n=33), Sjogren's syndrome group (n=35), rheumatoid arthritis group (n=43) and gout group (n=30). The course of disease was ≤ 5 years. Another 32 cases of physical examination during the same period were selected as the control group. All participants underwent conventional echocardiography to collect images, and obtained pressure strain loop parameters through offline ECHOPAC analysis. Statistical analysis of the correlation between routine parameters and myocardial work among groups was conducted to assess the left ventricular myocardial work status. Results Compared with the control group, the A peak of rheumatic immune disease groups increased and the E/A ratio decreased (P < 0.05). The E peak of systemic lupus erythematosus group and Sjogren's syndrome group decreased significantly (P < 0.05).The global wasted work of all rheumatic immune disease groups was higher, and the global work efficiency was lower (P < 0.05). The global longitudinal strain, global work index, and global constructive work in the systemic lupus erythematosus group and ankylosing spondylitis group and the global longitudinal strain, global work index, and global constructive work in the rheumatoid arthritis group and the global work index in the gout group were all decreased, with a statistically significant difference (P < 0.05). The absolute value of global longitudinal strain, left ventricular ejection fraction, and E/A ratio in the rheumatic immune disease group were positively correlated with global work index, global constructive work, and global work efficiency, while they were negatively correlated with global wasted work (P < 0.01). Conclusion The pressure strain loop can effectively assess the left ventricular myocardial work status in patients with rheumatic immune disease.It will objectively provide a more objective new diagnostic basis for clinical practice. -

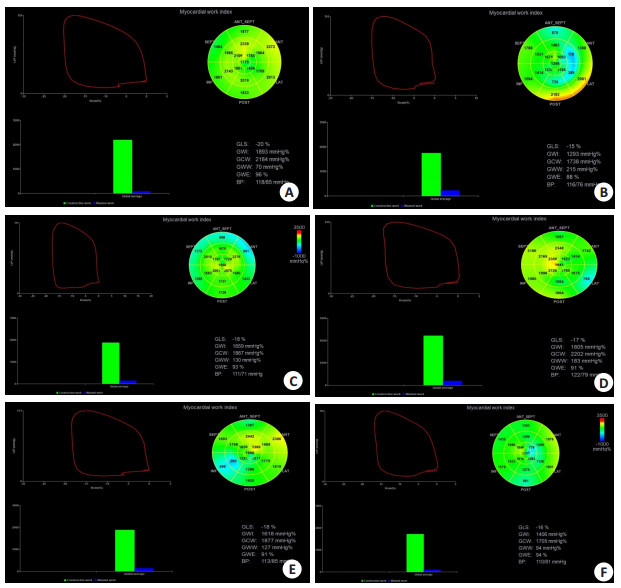
图 1 不同风湿免疫组的PSL参数的比较
Figure 1. PSL parameters comparison of different rheumatic immune disease groups. A: Control group (normal physical examination, female, 47 years old); B: Systemic lupus erythematosus group (female, 45 years old, disease duration: 4 years); C: Sjogren's syndrome group (female, 48 years old, disease duration: 3 years and 5 months); D: Ankylosing spondylitis group (male, 46 years old, disease duration: 4 years and 2 months); E: Gout patient group (male, 52 years, disease duration : 4 years); F: Rheumatoid arthritis group (female, 48 years old, disease duration: 3 years). Compared with the control group, GWW of all rheumatic immune groups increased, GWE decreased, and PSL area decreased.
表 1 风湿病组与对照组的一般资料比较
Table 1. Comparison of general clinical data between rheumatic group and control group (Mean±SD)
Characteristic Male/Female(n) Age (year) Systolic pressure (mmHg) Diastolic pressure (mmHg) Rheumatology group(n=171) Systemic lupus erythematosus group(n=30) 1/29 45.2±15.1 114.2±8.37 76.3±4.9 Sjogren's syndrome group(n=35) 5/30 47.4±11.34 115.6±7.2 76.8±3.8 Ankylosing spondylitis group(n=33) 25/8 44.4±14.2 116.2±7.8 76.0±6.1 Rheumatoid arthritis group(n=43) 4/39 51.6±10.2 116.6±8.8 77.0±6.3 Gout group(n=30) 28/2 50.1±10.4 113.1±6.2 75.6±4.5 Control group(n=32) 5/27 46.5±12.2 113.6±6.6 75.9±4.5 F - 2.216 1.354 0.437 P - 0.054 0.243 0.822  下载: 导出CSV
下载: 导出CSV
表 2 风湿病组与对照组常规超声心动图参数比较
Table 2. Comparison of routine echocardiographic parameters between rheumatic group and control group (Mean±SD)
Characteristic Diastolic interventricular septal thickness(mm) Left ventricular end-diastolic diameter(mm) Left ventricular end-systole diameter(mm) Ejection fraction(%) Fractional shortening(%) E peak(cm/s) A peak(cm/s) E/A ratio Rheumatology group(n=171) Systemic lupus erythematosus group(n=30) 8.3±1.5 48.5±3.3 29.4±3.0 69.1±5.6 38.4±3.6 58.6±1.7* 74.5±14.5* 0.8±0.2* Sjogren's syndrome group(n=35) 7.6±1.3 48.2±2.6 29.0±2.1 69.5±5.1 39.1±4.3 64.4±14.0* 72.0±17.1* 0.9±0.3* Ankylosing spondylitis group(n=33) 8.4±1.3 49.1±2.5 30.5±2.1 67.5±4.0 39.8±3.4 65.4±16.6 71.0±14.5* 1.0±0.5* Rheumatoid arthritis group(n=43) 7.7±1.3 48.5±3.0 29.5±2.5 68.3±4.1 38.4±3.4 66.6±14.5 71.3±15.9* 0.9±0.2* Gout group(n=30) 7.9±1.4 49.1±2.5 29.7±1.9 68.2±3.8 38.5±3.6 67.2±14.8 70.0±15.8* 1.0±0.3* Control group(n=32) 8.0±1.4 49.2±3.0 29.6±2.5 68.6±4.5 38.8±3.7 72.4±14.4 61.0±14.0 1.2±0.3 t 2.020 1.900 1.399 0.944 0.669 2.948 2.972 5.672 P 0.077 0.096 0.226 0.453 0.647 0.014 0.013 < 0.001 *P < 0.05 vs control group. E peak: early diastolic peak velocity of mitral valve orifice; A peak: late diastolic peak velocity of mitral valve orifice; E/A: The ratio of early diastolic peak flow velocity to late diastolic peak flow velocity of the mitral valve.
下载: 导出CSV
表 3 风湿病组与对照组的左心室PSL参数比较
Table 3. Comparison of left ventricular PSL parameters between rheumatic group and control group (Mean±SD)
Characte GLS(%) GW(mmHg%) GCW(mmHg%) GWW(mmH GWE(%) Rheumatology group(n=171) Systemic lupus erythematosus group(n=30) -17.5±1.6* 1542.5±168.8* 1916.1±145.3* 115.7±53.7* 93.2±2.8* Sjogren's syndrome group(n=35) -18.4±1.7 1656.6±173.2 2026.5±180.7 116.4±49.5* 93.5±2.1* Ankylosing spondylitis group(n=33) -17.5±1.8* 1553.4±197.3* 1908.5±194.6* 116.7±60.0* 93.4±3.1* Rheumatoid arthritis group(n=43) -17.7±1.5* 1586.8±160.6* 2000.4±225.0 137.1±61.1* 92.6±2.5* Gout group(n=30) -18.1±1.6 1595.8±165.6* 1983.8±184.9 130.5±70.1* 91.6±7.7* Control group(n=32) -18.6±1.2 1833.31±196.14 2006.0±170.3 60.96±16.65 95.6±1.6 t1 3.065 3.098 2.228 3.780 4.079 P1 < 0.05 < 0.05 < 0.05 < 0.05 < 0.05 t2 0.469 0.559 0.478 4.161 4.397 P2 0.641 0.578 0.635 < 0.05 < 0.05 t3 2.756 2.706 2.146 3.580 3.489 P3 < 0.05 < 0.05 < 0.05 < 0.05 < 0.05 t4 2.900 2.370 0.118 5.343 5.728 P4 < 0.05 < 0.05 0.907 < 0.05 < 0.05 t5 1.552 2.003 0.508 4.180 2.832 P5 0.125 < 0.05 0.613 < 0.05 < 0.05 *P<0.05 vs Control group. t1, P1: Systemic lupus erythematosus group vs Control group; t2, P2: Sjogren's syndrome group vs Control group; t3, P3: Ankylosing spondylitis group vs Control group; t4, P4: Rheumatoid arthritis group vs Control group; t5, P5: Gout group vs Control group; GLS: Global longitudinal strain; GWI: Global work index; GCW: Global constructive work; GWW: Global wasted work; GWE: Global work efficiency.
下载: 导出CSV
表 4 相关性分析
Table 4. Correlation analysis
Characteristic GWI GCW GWW GWE r P r P r P r P GLS absolute value 0.713 < 0.01 0.585 < 0.01 -0.450 < 0.01 0.350 < 0.01 Ejection fraction 0.809 < 0.01 0.550 < 0.01 -0.345 < 0.01 0.278 < 0.01 E/A ratio 0.381 < 0.01 0.341 < 0.01 -0.290 < 0.01 0.247 < 0.01
下载: 导出CSV
表 5 重复性检验结果
Table 5. Repeatability test results
Characteristic Intra physician Inter physician ICC 95% CI ICC 95% CI GLS 0.981 0.945-0.994 0.890 0.705-0.962 GWI 0.928 0.800-0.975 0.884 0.690-0.959 GCW 0.954 0.869-0.984 0.962 0.795-0.975 GWW 0.989 0.967-0.996 0.971 0.916-0.990 GWE 0.958 0.879-0.986 0.947 0.850-0.982 ICC: Intraclass correlation coefficient.
下载: 导出CSV
-
[1] 高晶月, 刘维, 王爱华, 等. 细胞焦亡在风湿免疫类疾病中作用机制的研究进展[J]. 中国临床保健杂志, 2022, 25(4): 562-567. https://www.cnki.com.cn/Article/CJFDTOTAL-LZBJ202204030.htm [2] Malemud CJ. The role of the JAK/STAT signal pathway in rheumatoid arthritis[J]. Ther Adv Musculoskelet Dis, 2018, 10(5): 117-127. [3] Veale DJ, McGonagle D, McInnes IB, et al. The rationale for Janus kinase inhibitors for the treatment of spondyloarthritis [J]. Rheumatology (Oxford), 2019, 58(2): 197-205. doi: 10.1093/rheumatology/key070 [4] Li Y, Higgs RE, Hoffman RW, et al. A Bayesian gene networkreveals insight into the JAK-STAT pathway in systemic lupus erythematosus[J]. PLoS One, 2019, 14(12): e0225651. doi: 10.1371/journal.pone.0225651 [5] Charras A, Arvaniti P, Le Dantec C, et al. JAK Inhibitors Suppress Innate Epigenetic Reprogramming: a Promise for Patients with Sjö gren's Syndrome[J]. Clin Rev Allergy Immunol, 2020, 58(2): 182-193. doi: 10.1007/s12016-019-08743-y [6] Temmoku J, Fujita Y, Matsuoka N, et al. Uric acid-mediated inflammasome activation in IL-6 primed innate immune cells is regulated by baricitinib[J]. Mod Rheumatol, 2021, 31(1): 270-275. doi: 10.1080/14397595.2020.1740410 [7] 孙立娟, 肖丞炜, 陈晓雪, 等. 压力-应变环评估代谢综合征患者早期左室心肌做功[J]. 中华超声影像学杂志, 2022, 31(5): 414-9. [8] Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging[J]. Eur Heart J Cardiovasc Imaging, 2015, 16(3): 233-271. doi: 10.1093/ehjci/jev014 [9] Prasad M, Hermann J, Gabriel SE, et al. Cardiorheumatology: cardiac involvement in systemic rheumatic disease[J]. Nat Rev Cardiol, 2015, 12(3): 168-176. doi: 10.1038/nrcardio.2014.206 [10] Lo Gullo A, Rodríguez-Carrio J, Gallizzi R, et al. Speckle tracking echocardiography as a new diagnostic tool for an assessment of cardiovascular disease in rheumatic patients[J]. Prog Cardiovasc Dis, 2020, 63(3): 327-340. doi: 10.1016/j.pcad.2020.03.005 [11] Cioffi G, Viapiana O, Ognibeni F, et al. Prognostic Role of Subclinical Left Ventricular Systolic Dysfunction Evaluated by Speckle-tracking Echocardiography in Rheumatoid Arthritis[J]. J Am Soc Echocardiogr, 2017, 30(6): 602-611. doi: 10.1016/j.echo.2017.02.001 [12] Atzeni F, Gianturco L, Colombo C, et al. Can speckle tracking echocardiography detect subclinical left ventricular dysfunction in patients with primary Sjögren's syndrome? [J]. Clin Exp Rheumatol, 2017, 35(1): 173. [13] Fine NM, Crowson CS, Lin G, et al. Evaluation of myocardial function in patients with rheumatoid arthritis using strain imaging by speckle-- tracking echocardiography[J]. Ann Rheum Dis, 2014, 73(10): 1833-9. doi: 10.1136/annrheumdis-2013-203314 [14] Zhong XF, Chen LX, Peng GJ, et al. Early assessment of subclinical myocardial injury in systemic lupus erythematosus by two-dimensional longitudinal layer speckle tracking imaging[J]. Quant Imaging Med Surg, 2022, 12(5): 2947-2960. doi: 10.21037/qims-21-805 [15] Emren SV, Gerç ik O, Ö zdemir E, et al. Evaluation of subclinical myocardial dysfunction using speckle tracking echocardiography in patients with radiographic and non-radiographic axial spondyloarthritis[J]. Eur J Rheumatol, 2019, 7(1): 9-15. [16] Russell K, Eriksen M, Aaberge L, et al. A novel clinical method for quantification of regional left ventricular pressure-strain loop area: a non-invasive index of myocardial work[J]. Eur Heart J, 2012, 33(6): 724-33. doi: 10.1093/eurheartj/ehs016 [17] Olsen FJ, Skaarup KG, Lassen MCH, et al. Normal Values for Myocardial Work Indices Derived From Pressure-Strain Loop Analyses: From the CCHS[J]. Circ Cardiovasc Imaging, 2022, 15(5): e013712. [18] Sugimoto T, Robinet S, Dulgheru R, et al. Echocardiographic reference ranges for normal left atrial function parameters: results from the EACVI NORRE study[J]. Eur Heart J Cardiovasc Imaging, 2018, 19(6): 630-8. doi: 10.1093/ehjci/jey018 [19] Edwards NFA, Scalia GM, Shiino K, et al. Global Myocardial Work Is Superior to Global Longitudinal Strain to Predict Significant Coronary Artery Disease in Patients With Normal Left Ventricular Function and Wall Motion[J]. J Am Soc Echocardiogr, 2020, 33(2): 257. doi: 10.1016/j.echo.2019.12.001 [20] Misra DP, Hauge EM, Crowson CS, et al. Atherosclerotic Cardiovascular Risk Stratification in the Rheumatic Diseases: An integrative, Multiparametric Approach[J]. Rheum Dis Clin North Am, 2023, 49(1): 19-43. doi: 10.1016/j.rdc.2022.07.004 [21] 施依璐, 铁宁, 段莎莎, 等. 无创压力-应变环技术评估系统性红斑狼疮患者心室收缩功能[J]. 中华超声影像学杂志, 2022, 31(10): 852-8. [22] 任梅, 尹立雪, 朱静, 等. 类风湿关节炎左心室收缩功能的超声压力-应变环评价[J]. 中国临床医学影像杂志, 2022, 33(10): 704-9. https://www.cnki.com.cn/Article/CJFDTOTAL-LYYX202210005.htm [23] 李思靓, 袁建军, 朱好辉, 等. 左心室无创压力-应变环评估强直性脊柱炎患者左心室收缩功能[J]. 中国医学影像技术, 2021, 37(3): 370-4. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYXX202103016.htm -

 点击查看大图
点击查看大图
计量
- 文章访问数: 90
- HTML全文浏览量: 66
- PDF下载量: 12
- 被引次数: 0