



Correlation between 18F-NaF uptake and fibrous cap rupture in carotid plaque
-
摘要:
目的 探究斑块的18F-NaF摄取与斑块的纤维帽破裂(FCR)间的相关性,以及18F-NaF摄取阳性与FCR是否存在相关性。 方法 选取我院神经外科在1年内收治的确诊颈动脉分叉处粥样硬化的患者共31例,行高分辨磁共振血管壁成像检查(HR-VWI)并用MR-VPD软件对斑块FCR情况进行分析,并于检查后1周内行18F-NaF PET/CT检查。根据18F-NaF在颈动脉的摄取程度,将患者分为18F-NaF摄取阳性组和18F-NaF摄取阴性组,分析组间斑块FCR的差异。 结果 31例患者中,双侧颈动脉分叉处均有斑块的患者为23例,其余8例为单侧颈动脉斑块,共收集54枚斑块。在54条动脉粥样硬化的颈动脉中,18F-NaF显影阳性的颈动脉为33条,18F-NaF显影阴性的颈动脉为21条,颈动脉显像阳性率为61.11%,阴性率为38.89%。18F-NaF阳性组存在FCR的斑块数量占比为58%,18F-NaF阴性组存在斑块FCR占比为19%,两组间斑块FCR情况的差异有统计学意义,18F-NaF摄取阳性的斑块FCR的占比较18F-NaF摄取阴性的斑块更多(t=2.034,P=0.045)。 结论 18F-NaF摄取阳性的斑块较18F-NaF摄取阴性的斑块FCR几率更大,18F-NaF摄取在一定程度上反映了斑块FCR情况,进而评估斑块易损性。 -
关键词:
- 动脉粥样硬化斑块 /
- 18F-NaF PET/CT /
- HR-VWI /
- 纤维帽
Abstract:Objective To investigate the correlation between 18F-NaF uptake of plaques and fibrous cap rupture (FCR) of plaques, and the correlation between 18F-NaF uptake positivity and FCR. Methods Thirty-one patients with confirmed atherosclerosis at the carotid bifurcation who were admitted to our hospital within a year of diagnosis were selected. The patients underwent high-resolution magnetic resonance vessel wall imaging with MR-VPD software. The plaque FCR conditions was analyzed. The 18F-NaF PET / CT was performed with in 1 week after high-resolution magnetic resonance vessel wall imaging examination. Based on the extent of 18F-NaF uptake in carotid arteries, patients were divided into 18F-NaF uptake positive and 18F-NaF uptake negative groups. Differences of plaque FCR between groups were analyzed. Results There were 23 patients with both plaques in bilateral carotid bifurcations out of 31 patients and the remaining 8 patients with unilateral carotid plaques were included in this study. Fifty-four plaques were collected. Among 54 atherosclerotic carotid arteries, 33 carotid arteries were positive by 18F-NaF imaging and 21 carotid arteries were negative by 18F-NaF imaging, showing 61.11% positive and 38.89% negative carotid artery images. The proportion of plaques with FCR present was 58% in the 18F-NaF positive group and 19% in the 18F-NaF negative group. The difference in the FCR situation of plaques between the two groups was statistically significant, with a higher proportion of plaques positive for 18F-NaF uptake having FCR than plaques negative for 18F-NaF uptake.(t=2.034, P=0.045). Conclusion Plaques positive for 18F-NaF uptake has greater odds of FCR than plaques negative for 18F-NaF uptake. 18F-NaF uptake to some extent reflects plaques with FCR, which in turn assesses plaque vulnerability. -

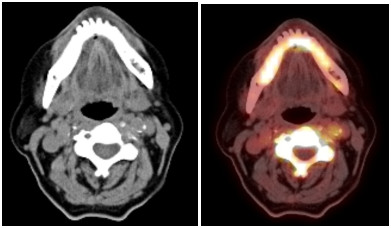
图 1 18F-NaF摄取阳性PET/CT图像
Figure 1. PET/CT images with positive 18F-NaF uptake.
The loca-tions of the cross markers in the figure is carotid plaque positive for 18F-NaF uptake.

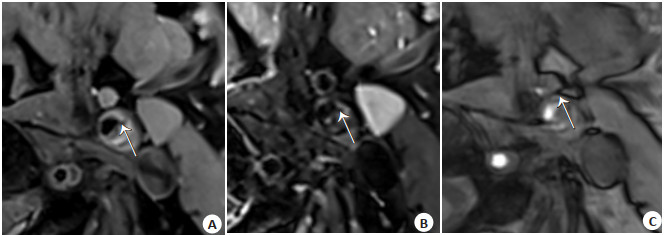
图 2 斑块FCR的HR-VWI图像
Figure 2. HR-VWI image of plaque FCR.
A: Plaque surface niche in T1WI represents FCR (white arrow); B: Plaque surface niche in T2WI represents FCR (white arrow); C: A defective hypointense band on the plaque surface with blood flow signal into the niche on the 3D TOF sequence indicating the presence of FCR (white arrow).

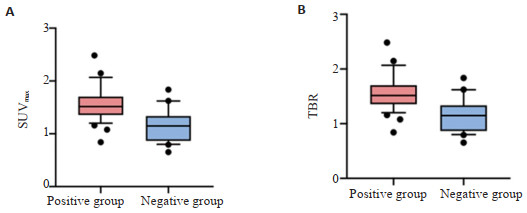
图 3 18F-NaF PET/CT显像阳性与阴性颈动脉SUVmax及TBR的比较
Figure 3. Comparison of positive and negative carotid SUVmax and TBR in 18F-NaF PET/CT imaging.
A: SUVmax was higher in the 18F-NaF positive group than in the negative group, P < 0.05; B: TBR was higher in the 18F-NaF positive group than in the negative group, P < 0.05.
表 1 患者的一般资料
Table 1. Clinical baseline data of patients
Clinical details of the patients Numerical value Stature(cm, Mean±SD) 170±5.05 Age(year, Mean±SD) 64.44±7.17 Weight(kg, Mean±SD) 74.03±13.56 Gender [male, n(%)] 29 (93.55) Excessive drinking [yes, n(%)] 16 (51.61) Smoke [yes, n(%)] 21 (67.74) Diabetes mellitus [yes, n(%)] 7 (22.58) Systolic pressure (mmHg, Mean±SD) 152.69±32.70 Diastolic pressure (mmHg, Mean±SD) 94.09±13.54 BMI(kg/m2, Mean±SD) 25.55±4.18 Clinical symptoms [yes, n(%)] 27 (87.10)  下载: 导出CSV
下载: 导出CSV
表 2 18F-NaF PET/CT显像阳性与阴性颈动脉斑块FCR情况统计表
Table 2. Statistical table of positive and negative carotid plaque FCR on 18F-NaF PET/CT imaging
Subgroup FCR Without FCR Total Proportion of FCR t P 18F-NaF positive group 21 11 33 58% 2.034 0.045 18F-NaF negative group 4 17 21 19%
下载: 导出CSV
-
[1] 刘青, 李伟粟. 初发脑梗死患者颈动脉斑块磁共振成像特征与再发危险性关系的研究进展[J]. 实用医技杂志, 2022, 29(6): 654-7. doi: 10.19522/j.cnki.1671-5098.2022.06.029 [2] Li S, Wei J, Huang R, et al. High-risk features of basilar artery atherosclerotic plaque[J]. Front Neurol, 2022, 13: 1019036. doi: 10.3389/fneur.2022.1019036 [3] Naghavi M, Libby P, Falk E, et al. From vulnerable plaque to vulnerable patient: a call for new definitions and risk assessment strategies: part[IJ]. Circulation, 2003, 108(14): 1664-72. [4] Naghavi M, Libby P, Falk E, et al. From vulnerable plaque to vulnerable patient: a call for new definitions and risk assessment strategies: part Ⅱ[J]. Circulation, 2003, 108(15): 1772-8. doi: 10.1161/01.CIR.0000087481.55887.C9 [5] 王晓曦, 侯慧卿, 刘艳宁, 等. 颈动脉不稳定斑块的影像学评估与组织病理学的对比研究[J]. 中国超声医学杂志, 2022, 38(12): 1337-40. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGCY202212005.htm [6] 谭玉婷, 黄磊, 张怡婵, 等. 多模态影像学评估颈动脉粥样硬化易损斑块药物治疗进展[J]. 中国医学影像技术, 2023, 39(1): 117-21. doi: 10.13929/j.issn.1003-3289.2023.01.027 [7] 王丹妮, 李康. 颈动脉斑块易损性与缺血性卒中关系的影像学评价研究进展[J]. 影像研究与医学应用, 2022, 6(24): 11-3. https://www.cnki.com.cn/Article/CJFDTOTAL-YXYY202224004.htm [8] 李依明, 郑吟诗, 林光耀, 等. 颈动脉超声和能谱CT以及MR高分辨率管壁成像诊断颈动脉斑块稳定性的临床价值[J]. 中华全科医学, 2022, 20(10): 1737-41, 1780. https://www.cnki.com.cn/Article/CJFDTOTAL-SYQY202210028.htm [9] 李挺, 李康. 颈动脉斑块的易损性特征与缺血性卒中相关性的MRI研究进展[J]. 现代医用影像学, 2022, 31(12): 2207-10. https://www.cnki.com.cn/Article/CJFDTOTAL-XDYY202212007.htm [10] 中华医学会神经病学分会, 中华医学会神经病学分会脑血管病学组, 彭斌, 等. 中国急性缺血性脑卒中诊治指南2018[J]. 中华神经科杂志, 2018, 51(9): 666-82. https://www.cnki.com.cn/Article/CJFDTOTAL-XDJB201911024.htm [11] Vengrenyuk Y, Carlier S, Xanthos S, et al. A hypothesis for vulnerable plaque rupture due to stress-induced debonding around cellular microcalcifications in thin fibrous caps[J]. Proc Natl Acad Sci USA, 2006, 103(40): 14678-83. [12] Hutcheson JD, Goettsch C, Bertazzo S, et al. Genesis and growth of extracellular-vesicle-derived microcalcification in atherosclerotic plaques[J]. Nat Mater, 2016, 15(3): 335-43. [13] 高飞, 欧阳雪晖, 王慧杰. 18F-FDG及18F-NaF正电子发射断层扫描在颈动脉粥样硬化斑块成像中的研究进展[J]. 分子影像学杂志, 2023, 46(1): 181-7. doi: 10.12122/j.issn.1674-4500.2023.01.35 [14] Mechtouff L, Sigovan M, Douek P, et al. Simultaneous assessment of microcalcifications and morphological criteria of vulnerability in carotid artery plaque using hybrid 18F-NaF PET/MRI[J]. J Nucl Cardiol, 2022, 29(3): 1064-74. [15] De Azevedo D, Geers J, Gheysens O, et al. 18F-sodium fluoride PET/CT in assessing valvular heart and atherosclerotic diseases[J]. Semin Nucl Med, 2023, 53(2): 241-57. [16] 李莉. 18F-NaF PET-CT识别动脉粥样硬化不稳定斑块临床研究[D]. 太原: 山西医科大学, 2017. [17] Huang R, Chen H, Li C, et al. Increased proximal wall shear stress of basilar artery plaques associated with ruptured fibrous cap[J]. Brain Sci, 2022, 12(10): 1397. [18] Gupta A, Baradaran H, Schweitzer AD. Carotid plaque MRI and stroke risk: a systematic review and meta-analysis[J]. J Vasc Surg, 2014, 59(4): 1175. [19] Hatsukami TS, Ross R, Polissar NL, et al. Visualization of fibrous cap thickness and rupture in human atherosclerotic carotid plaque in vivo with high-resolution magnetic resonance imaging[J]. Circulation, 2000, 102(9): 959-64. [20] 开慧华, 沈栋, 潘昌杰. 冠脉CTA定量参数预测薄纤维帽粥样硬化斑块易损性的可行性[J]. 放射学实践, 2021, 36(8): 1000-4. https://www.cnki.com.cn/Article/CJFDTOTAL-FSXS202108015.htm [21] Barrett HE, van der Heiden K, Farrell E, et al. Calcifications in atherosclerotic plaques and impact on plaque biomechanics[J]. J Biomech, 2019, 87: 1-12. http://www.xueshufan.com/publication/2921536015 [22] Wurster Thomas H, Ulf L, Abdelwahed Youssef S, et al. Simultaneous[18F]fluoride and gadobutrol enhanced coronary positron emission tomography/magnetic resonance imaging for in vivo plaque characterization[J]. Eur Heart J Cardiovasc Imaging, 2022, 23(10): 1391-8. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 102
- HTML全文浏览量: 55
- PDF下载量: 3
- 被引次数: 0