



Prospective study of MSCT and MRI in pathological grading and assessment of tumor blood supply in pancreatic neuroendocrine tumors
-
摘要:
目的 研究多层螺旋CT(MSCT)与MRI对胰腺神经内分泌肿瘤病理分级和肿瘤血供评估的差异性。 方法 本研究为前瞻性研究,选取我院2019年1月~2022年6月进行诊断并治疗的胰腺神经内分泌肿瘤患者70例作为研究对象,其中G1级患者25例,G2级患者23例,G3级患者22例,富血供胰腺神经内分泌肿瘤患者29例,另选取同期进行健康体检的志愿者70例作为对照组,比较两组、不同肿瘤分级、肿瘤血供的MSCT指标以及MR指标之间的差异,研究MSCT与MRI对胰腺神经内分泌肿瘤病理分级和肿瘤血供评估的诊断意义。 结果 观察组患者的动脉期以及门脉期的CT绝对强化值低于对照组(P < 0.05);观察组患者的动脉期高信号、门脉期高信号低于对照组(P < 0.05);不同分级、不同血液供应患者的MSCT动脉期以及门脉期的CT绝对强化值、边缘、形状、囊变坏死、主胰管扩张以及远处转移情况之间的差异有统计学意义(P < 0.05);不同分级、不同血液供应患者的MRI动脉期高信号、门脉期高信号、边缘、形状、囊变坏死、主胰管扩张以及远处转移情况之间的差异有统计学意义(P < 0.05);MSCT、MRI联合诊断的特异性高于单独检测(P < 0.05)。 结论 MSCT与MRI对胰腺神经内分泌肿瘤病理分级和肿瘤血供评估具有积极的意义。 Abstract:Objective To investigate the difference between MSCT and MRI in the pathological grading and assessment of tumor blood supply in pancreatic neuroendocrine tumors. Methods In this prospective study, 70 patients with pancreatic neuroendocrine tumors diagnosed and treated in our hospital from January 2019 to June 2022 were selected as the research objects, including 25 patients with G1 grade, 23 patients with G2 grade, and 22 patients with G3 grade, as well as 29 patients with blood-rich pancreatic neuroendocrine tumors. Another 70 healthy volunteers who underwent physical examination at the same time were selected as the control group. The differences of MSCT and MR indexes between the two groups, patients with different tumor grades, and patients with different tumor blood supply were compared. The diagnostic significance of MSCT and MRI in the pathological grade and assessment of tumor blood supply in pancreatic neuroendocrine tumors were analyzed. Results The CT absolute enhancement values of arterial phase and portal phase in the observation group were significantly lower than those in the control group (P < 0.05). The high signal in arterial phase and portal phase in the observation group were significantly lower than those in the control group (P < 0.05). There were significant differences in CT absolute enhancement value, margin, shape, cystic degeneration and necrosis, main pancreatic duct dilatation and distant metastasis in arterial phase and portal phase of patients with different grades and blood supplies by MSCT (P < 0.05). There were significant differences in high signal in arterial phase and portal phase, margin, shape, cystic necrosis, main pancreatic duct dilatation and distant metastasis in patients with different grades and blood supplies by MRI (P < 0.05). The specificity of combination diagnosis of MSCT and MRI was significantly higher than that of single detection (P < 0.05). Conclusion MSCT and MRI have positive significance in pathological grading and assessment of tumor blood supply in pancreatic neuroendocrine tumors. -
Key words:
- Keywords: MSCT /
- MRI /
- pancreatic neuroendocrine neoplasms /
- pathological grade /
- tumor blood supply
-
表 1 两组患者的人口学以及临床资料比较
Table 1. Comparison of demographic and clinical data between the two groups (n=70)
组别 性别(男/女, n) 年龄(岁, Mean±SD) BMI(kg/m2, Mean±SD) 观察组 25/45 47.03±3.44 24.55±2.03 对照组 20/50 46.81±3.27 24.64±2.24 χ2/t 0.819 0.388 0.249 P 0.366 0.699 0.804  下载: 导出CSV
下载: 导出CSV
表 2 两组的动脉期以及门脉期的CT绝对强化值比较
Table 2. Comparison of CT absolute enhancement values in arterial phase and portal phase between the two groups (Hu, Mean±SD)
组别 动脉期CT绝对强化值 门脉期CT绝对强化值 观察组 41.42±11.21 93.81±11.12 对照组 67.12±11.27 124.48±11.09 t 13.527 16.339 P < 0.001 < 0.001
下载: 导出CSV
表 3 两组的动脉期高信号、门脉期高信号比较
Table 3. Comparison of arterial hyperintensity and portal hyperin-tensity between the two groups [n=70, n(%)]
组别 动脉期高信号 门脉期高信号 观察组 20(28.57) 17(24.29) 对照组 55(78.57) 52(74.29) χ2 35.182 35.012 P < 0.001 < 0.001
下载: 导出CSV
表 4 不同分级患者的MSCT指标比较
Table 4. Comparison of MSCT indexes of patients with different grades
组别 动脉期CT绝对强化值(Hu, Mean±SD) 门脉期CT绝对强化值(Hu, Mean±SD) 边缘(模糊)[n(%)] 形状(不规则)[n(%)] 囊变坏死[n(%)] 主胰管扩张[n(%)] 远处转移[n(%)] G1级(n=25) 45.22±3.69 102.36±3.81 0(0.00) 1(4.00) 1(4.00) 2(8.00) 0(0.00) G2级(n=23) 40.99±3.18 94.55±2.66 4(17.39) 5(21.74) 5(21.74) 7(30.43) 3(13.04) G3级(n=22) 37.55±3.36 83.32±2.95 9(40.91) 11(50.00) 7(31.82) 10(45.45) 5(22.73) F/χ2 15.023 16.023 12.981 13.591 6.22 8.489 6.062 P < 0.001 < 0.001 < 0.001 < 0.001 0.045 0.014 0.048
下载: 导出CSV
表 5 不同肿瘤分级患者的MRI指标比较
Table 5. Comparison of MRI indicators in patients with different tumor grades [n(%)]
组别 动脉期高信号 门脉期高信号 边缘(模糊) 形状(不规则) 囊变坏死 主胰管扩张 远处转移 G1级(n=25) 12(48.00) 11(44.00) 1(4.00) 0(0.00) 0(0.00) 1(4.00) 0(0.00) G2级(n=23) 5(21.74) 4(17.39) 4(17.39) 5(21.74) 6(26.09) 7(30.43) 2(8.70) G3级(n=22) 3(13.64) 2(9.09) 11(50.00) 12(54.55) 7(31.82) 11(50.00) 6(27.27) χ2 7.552 8.641 14.621 19.061 9.112 12.712 8.852 P 0.023 0.013 0.001 <0.001 0.011 0.002 0.012
下载: 导出CSV
表 6 不同血液供应患者的MSCT指标比较
Table 6. Comparison of MSCT indexes in patients with different blood supply
组别 动脉期CT绝对强化值(Hu, Mean±SD) 门脉期CT绝对强化值(Hu, Mean±SD) 边缘(模糊)[n(%)] 形状(不规则)[n(%)] 囊变坏死[n(%)] 主胰管扩张[n(%)] 远处转移[n(%)] 乏血组(n=41) 45.89±3.96 105.56±2.55 5(12.20) 4(9.76) 3(7.32) 7(17.07) 2(4.88) 富血组(n=29) 35.6±3.22 78.70±3.67 11(37.93) 12(41.38) 10(34.48) 12(41.38) 6(20.69) t/χ2 11.962 34.029 6.381 9.631 8.291 5.071 4.201 P <0.001 <0.001 0.012 0.002 0.004 0.024 0.041
下载: 导出CSV
表 7 不同血液供应患者的MRI指标比较
Table 7. Comparison of MRI parameters in patients with different blood supply
组别 动脉期高信号 门脉期高信号 边缘(模糊) 形状(不规则) 囊变坏死 主胰管扩张 远处转移 乏血组(n=41) 17(41.46) 13(31.71) 4(9.76) 5(12.20) 4(9.76) 6(14.63) 1(2.44) 富血组(n=29) 3(10.34) 3(10.34) 12(41.38) 11(37.93) 9(31.03) 13(44.83) 7(24.14) χ2 8.061 6.212 9.631 6.381 5.091 7.831 7.901 P 0.005 0.013 0.002 0.012 0.024 0.005 0.005
下载: 导出CSV
表 8 联合诊断效能分析
Table 8. Analysis of combined diagnostic efficiency
指标 诊断方法 真阳例数(n) 假阳例数(n) 真阴例数(n) 假阴例数(n) 准确率(%) 敏感度(%) 特异性(%) 阳性预测值(%) 阴性预测值(%) MSCT 11 11 37 11 68.57 50.00 77.08 50.00 77.08 疾病分级 MRI 9 12 36 13 64.29 40.91 75.00 42.86 73.47 联合检测 8 3 45 14 75.71 36.36 93.75 72.73 76.27 MSCT 22 11 30 7 74.29 75.86 73.17 66.67 81.08 肿瘤血供 MRI 21 12 29 8 71.43 72.41 70.73 63.64 78.38 联合检测 19 2 39 10 82.86 65.52 95.12 90.48 79.59
下载: 导出CSV
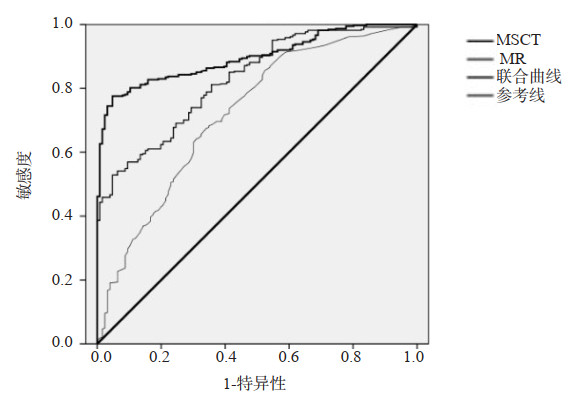
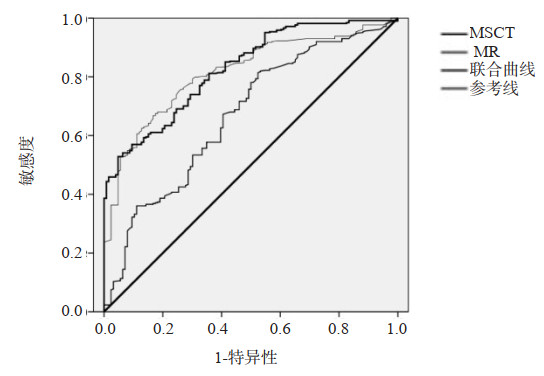
表 9 ROC曲线分析
Table 9. ROC curve analysis
指标 诊断方法 标准误 AUC AUC(95% CI) P MSCT 11.231 0.771 0.762~0.864 < 0.001 疾病分级 MRI 9.252 0.776 0.602~0.800 < 0.001 联合检测 3.222 0.803 0.755~0.852 < 0.001 MSCT 4.342 0.722 0.810~0.977 < 0.001 肿瘤血供 MRI 2.451 0.781 0.662~0.970 < 0.001 联合检测 0.027 0.878 0.762~0.899 < 0.001
下载: 导出CSV
-
[1] Li WX, et al. Pancreatic neuroendocrine neoplasms: CT spectral imaging in grading[J]. Acad Radiol, 2021, 28(2): 208-16. doi: 10.1016/j.acra.2020.01.033 [2] Majala S, Vesterinen T, Seppänen H, et al. Correlation of somatostatin receptor 1-5 expression, [68Ga]Ga-DOTANOC, 18FFDG PET/CT and clinical outcome in a prospective cohort of pancreatic neuroendocrine neoplasms[J]. Cancers, 2021, 14(1): 162. doi: 10.3390/cancers14010162 [3] Yu HP, et al. Differential diagnosis of nonhypervascular pancreatic neuroendocrine neoplasms from pancreaticductal adenocarcinomas, based on computed tomography radiological features and texture analysis[J]. Acad Radiol, 2020, 27(3): 332-41. doi: 10.1016/j.acra.2019.06.012 [4] Luo Y, Chen X, Chen J, et al. Preoperative prediction of pancreatic neuroendocrine neoplasms grading based on enhanced computed tomography imaging: validation of deep learning with a convolutional neural network[J]. Neuroendocrinology, 2020, 110 (5): 338-50. doi: 10.1159/000503291 [5] Yu F, Fu JJ, Zhang C, et al. Use of chromogranin A for monitoring patients with pancreatic neuroendocrine neoplasms[J]. Pancreas, 2021, 50(6): 882-9. doi: 10.1097/MPA.0000000000001852 [6] 王海彬, 段成洲, 崔振华. 多层螺旋CT与磁共振成像诊断胰腺神经内分泌肿瘤及其对病理分级的临床价值[J]. 安徽医药, 2020, 24(11): 2177-80. doi: 10.3969/j.issn.1009-6469.2020.11.015 [7] 熊焕煜, 万玲, 杨爽. 胰腺神经内分泌肿瘤多层螺旋计算机断层扫描、MRI影像学征象分析[J]. 癌症进展, 2022, 20(5): 497-500. https://www.cnki.com.cn/Article/CJFDTOTAL-AZJZ202205018.htm [8] 刘鸽, 宦怡, 高燕军, 等. 多层螺旋CT及MRI对胰腺神经内分泌肿瘤的诊断价值[J]. 实用放射学杂志, 2021, 37(7): 1103-7. https://www.cnki.com.cn/Article/CJFDTOTAL-YYSO202110015.htm [9] Tan HL, Teo RYA, Syn NL, et al. Minimally invasive versus open pancreatectomies for pancreatic neuroendocrine neoplasms: a propensity-score-matched study[J]. World J Surg, 2020, 44(9): 3043-51. doi: 10.1007/s00268-020-05582-3 [10] Grozinsky-Glasberg S, Lines KE, Avniel-Polak S, et al. Preclinical drug studies in MEN1-related neuroendocrine neoplasms (MEN1-NENs)[J]. Endocr Relat Cancer, 2020, 27(9): R345-5. [11] Muscogiuri G, Altieri B, Albertelli M, et al. Epidemiology of pancreatic neuroendocrine neoplasms: a gender perspective[J]. Endocrine, 2020, 69(2): 441-50. doi: 10.1007/s12020-020-02331-3 [12] Muscogiuri G. Pancreatic neuroendocrine neoplasms: does sex matter?[J]. Trends Endocrinol Metab, 2020, 31(9): 631-41. doi: 10.1016/j.tem.2020.02.010 [13] Al-Toubah T, Schell MJ, Cives M, et al. A phase Ⅱ study of ibrutinib in advanced neuroendocrine neoplasms[J]. Neuroendocrinology, 2020, 110(5): 377-83. doi: 10.1159/000502383 [14] Kann PH, Scheunemann A, Dorzweiler P, et al. Pancreatic neuroendocrine neoplasias in multiple endocrine neoplasia type 1 are predominantly located in the dorsal anlage: an endoscopic ultrasound study[J]. Pancreas, 2021, 50(8): 1169-72. doi: 10.1097/MPA.0000000000001890 [15] 章伟, 郏潜新, 蒋政焱, 等. CT灌注成像在胰腺浆液性囊腺瘤与良性神经内分泌肿瘤鉴别的价值[J]. 实用放射学杂志, 2020, 36(12): 1965-8. doi: 10.3969/j.issn.1002-1671.2020.12.020 [16] 李璐杰, 宋晨宇, 周小琦, 等. 胰腺神经内分泌肿瘤CT征象与SSTR2、VEGFR2及MGMT表达的关系[J]. 中山大学学报: 医学科学版, 2021, 42(6): 892-9. https://www.cnki.com.cn/Article/CJFDTOTAL-ZSYK202106011.htm [17] 田宁, 张洪涛, 贾茹, 等. 胰腺神经内分泌肿瘤: 动态增强CT与病理分级的相关性研究[J]. 军事医学, 2020, 44(11): 837-41. https://www.cnki.com.cn/Article/CJFDTOTAL-JSYX202011009.htm [18] 王雅杰, 崔文静, 陈晓, 等. 增强CT对乏血供胰腺神经内分泌肿瘤及肿块型胰腺炎的鉴别诊断价值[J]. 医学研究生学报, 2020, 33(7): 732-6. https://www.cnki.com.cn/Article/CJFDTOTAL-JLYB202007012.htm [19] 杨琰昭, 徐嘉旭, 李若坤, 等. 双层探测器光谱CT能谱图像在胰腺神经内分泌肿瘤检出中的应用价值[J]. 中华放射学杂志, 2020, 54(6): 534-8. [20] 魏然, 杨甜甜, 姬慧君, 等. 胰腺神经内分泌肿瘤31例CT表现与病理分级关联性分析[J]. 中华肿瘤防治杂志, 2020, 27(15): 1247-52. https://www.cnki.com.cn/Article/CJFDTOTAL-QLZL202015012.htm [21] 谭正武, 任克, 缪琪, 等. CT灌注和磁共振增强诊断CT三期增强阴性胰腺神经内分泌肿瘤的初步探讨[J]. 中国医学计算机成像杂志, 2017, 23(5): 483-9. https://www.cnki.com.cn/Article/CJFDTOTAL-YJTY201705025.htm -

 点击查看大图
点击查看大图
计量
- 文章访问数: 174
- HTML全文浏览量: 128
- PDF下载量: 8
- 被引次数: 0