



Early predictive value of penumbra CT perfusion imaging parameters on prognosis of patients with acute ischemic stroke after thrombolytic therapy
-
摘要:
目的 研究急性缺血性脑卒中(AIS)患者溶栓治疗后CT灌注成像参数变化及其对预后的早期预测价值。 方法 选取2019年3月~2022年3月我院90例AIS患者临床资料为样本开展回顾性研究,均于随访3月时采用改良Rankin量表(mRS)评分并根据结果分组,以mRS≤2分为预后良好组(n=31),>2分为预后不良组(n=59),比较两组溶栓治疗后半暗带CT灌注成像参数脑血容量(CBV)、脑血流量(CBF)、平均通过时间(MTT)和达峰时间(TTP),并以健侧为对照计算各参数相对值rCBF、rCBV、rMTT和rTTP,分析各参数对AIS患者预后的预测价值。 结果 溶栓治疗后预后不良组AIS患者半暗带CBF、CBV、rCBF和rCBV均低于预后良好组(P < 0.05),MTT和TTP均高于预后良好组(P < 0.05),两组rMTT和rTTP比较未见差异, 无统计学意义(P>0.05);CBF、CBV、MTT和TTP预测AIS患者预后的曲线下面积(AUC)分别为0.701、0.662和0.698,4项参数联合预测的AUC为0.817,敏感度为93.55%,特异性为64.41%;rCBF和rCBV预测AIS患者预后的AUC分别为0.724和0.798,两项参数联合预测的AUC为0.812,敏感度为96.77%,特异性为57.63%。 结论 CT灌注成像可对AIS患者半暗带血流灌注水平进行定量分析,检测溶栓治疗后CBF、CBV、MTT和TTP等参数及其与健侧镜像区脑组织相对值可为早期评估患者预后提供参考。 -
关键词:
- 急性缺血性脑卒中 /
- 预后 /
- CT灌注成像 /
- 改良Rankin量表 /
- 半暗带
Abstract:Objective To explore the changes in CT perfusion imaging parameters in patients with acute ischemic stroke (AIS) after thrombolytic therapy and their early predictive value on prognosis. Methods The clinical data of 90 patients with AIS in the hospital were enrolled from March 2019 to March 2022 for retrospective analysis. All patients were followed up for 3 months with modified Rankin scale (mRS) score and grouped according to the results. Patients with MRS≤2 points were assigned to good prognosis group (n=31), and patients with score >2 points were classified into poor prognosis group (n=59). The penumbra CT perfusion imaging parameters including cerebral blood flow (CBF), cerebral blood volume (CBV), mean transit time (MTT) and time to peak (TTP) were compared between the two groups after thrombolytic therapy. The healthy side was used as the control to calculate the relative values of rCBF, rCBV, rMTT and rTTP, and the predictive value of each parameter on the prognosis of AIS patients was analyzed. Results After thrombolytic therapy, the CBF, CBV, rCBF and rCBV in penumbra in poor prognosis group were significantly lower than those in good prognosis group (P < 0.05).The MTT and TTP were significantly longer than those in good prognosis group (P < 0.05), but there were no statistical differences in rMTT and rTTP between the two groups (P>0.05). The AUCs of CBF, CBV, MTT and TTP in predicting the prognosis of AIS patients were 0.701, 0.662 and 0.698 respectively. The AUC, sensitivity and specificity of the combined prediction of the four parameters were 0.817, 93.55% and 64.41%. The AUCs of rCBF and rCBV in predicting the prognosis of AIS patients were 0.724 and 0.798 respectively. The AUC, sensitivity and specificity of the combined prediction of the two parameters were 0.812, 96.77% and 57.63%. Conclusion CT perfusion imaging can quantitatively analyze the blood perfusion level in the penumbra of AIS patients, and the detection of CBF, CBV, MTT and TTP parameters after thrombolytic therapy and their relative values in brain tissue in the mirror region of the healthy side can provide a reference for early assessment of prognosis of patients. -
Key words:
- acute ischemic stroke /
- prognosis /
- CT perfusion imaging /
- modified Rankin scale /
- penumbra
-

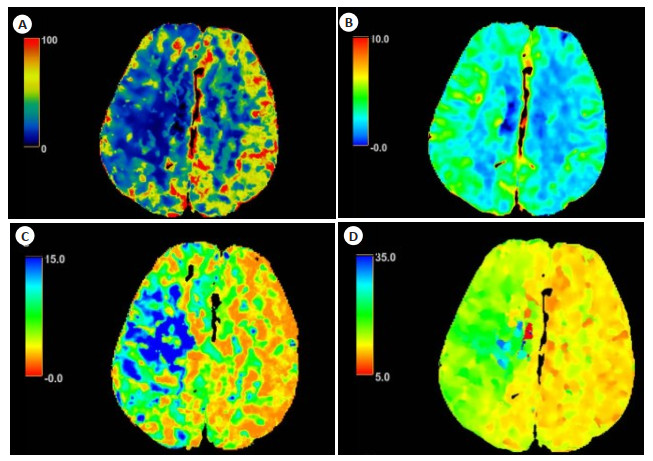
图 1 AIS患者CBF、CBV、MTT和TTP伪彩图
患者女性, 75岁, 右侧大脑中动脉区急性脑梗死. CTP图像显示CBF(A)和CBV(B)与对侧相比明显降低, MTT(C)和TTP(D)与对侧相比明显升高.
Figure 1. Pseudo-color images of CBF, CBV, MTT and TTP of AIS patients.

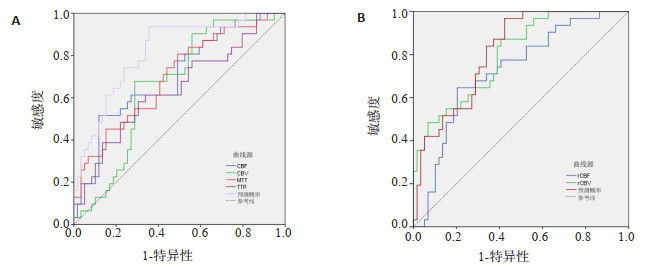
图 2 溶栓治疗后半暗带CTP参数评估AIS患者预后的ROC曲线
A: CBF、CBV和MTT评估AIS患者预后的ROC曲线; B: rCBF和rCBV评估AIS患者预后的ROC曲线.
Figure 2. ROC curves of penumbra CTP parameters after thrombolytic therapy in evaluating the prognosis of AIS patients.
表 1 不同预后AIS患者溶栓治疗后半暗带CBF、CBV、MTT和TTP比较
Table 1. Comparison of penumbra CBF, CBV, MTT and TTP in AIS patients with different prognosis status after thrombolytic therapy (Mean±SD)
组别 CBF(mL· 100g-1· min-1) CBV(mL/100g) MTT(s) TTP(s) 预后不良组(n=31) 50.39±7.12 2.04±0.67 4.89±1.24 21.67±5.31 预后良好组(n=59) 56.01±7.24 2.49±0.73 4.16±1.07 19.28±4.52 t 3.537 2.936 2.017 2.132 P 0.001 0.004 0.047 0.036 CBF: 脑血流量; CBV: 脑血容量; MTT: 平均通过时间; TTP: 达峰时间.  下载: 导出CSV
下载: 导出CSV
表 2 不同预后AIS患者溶栓治疗后半暗带rCBF、rCBV、rMTT和rTTP比较
Table 2. Comparison of penumbra rCBF, rCBV, rMTT and rTTP in AIS patients with different prognosis status after thrombolytic therapy (Mean±SD)
分组 rCBF rCBV rMTT rTTP 预后不良组(n=31) 0.47±0.13 0.62±0.16 2.40±0.65 1.36±0.42 预后良好组(n=59) 0.64±0.18 0.79±0.21 2.19±0.57 1.23±0.34 t 2.827 2.476 1.582 0.977 P 0.006 0.016 0.117 0.331
下载: 导出CSV
表 3 CBF、CBV和MTT对AIS患者预后的早期预测价值分析
Table 3. Analysis of early predictive value of CBF, CBV and MTT on prognosis of AIS patients
CTP参数 AUC SE. 95% CI 阈值 约登指数 敏感度(%) 特异性(%) CBF 0.701 0.058 0.596~0.793 > 57.56 0.398 51.61 88.14 CBV 0.662 0.058 0.555~0.758 > 2.32 0.389 67.74 71.19 MTT 0.698 0.058 0.592~0.791 ≤4.84 0.315 80.65 50.85 TTP 0.643 0.063 0.535~0.741 ≤18.39 0.276 58.06 69.49 联合预测 0.817 0.047 0.721~0.891 - 0.580 93.55 64.41
下载: 导出CSV
表 4 rCBF和rCBV对AIS患者预后的早期预测价值分析
Table 4. Analysis of early predictive value of rCBF and rCBV on prognosis of AIS patients
CTP参数 AUC SE. 95% CI 阈值 约登指数 敏感度(%) 特异性(%) rCBF 0.724 0.056 0.620~0.813 ≤0.50 0.442 64.52 79.66 rCBV 0.798 0.047 0.701~0.876 ≤0.76 0.464 87.10 59.32 联合预测 0.812 0.044 0.716~0.887 - 0.544 96.77 57.63
下载: 导出CSV
-
[1] 《中国脑卒中防治报告》编写组, 王陇德. 《中国脑卒中防治报告2020》概要[J]. 中国脑血管病杂志, 2022, 19(2): 136-44. doi: 10.3969/j.issn.1672-5921.2022.02.011 [2] Chen YP, Wright N, Guo Y, et al. Mortality and recurrent vascular events after first incident stroke: a 9-year community-based study of 0· 5 million Chinese adults[J]. Lancet Glob Health, 2020, 8(4): e580-90. doi: 10.1016/S2214-109X(20)30069-3 [3] Voleti S, Vidovich J, Corcoran B, et al. Correlation of Alberta stroke program early computed tomography score with computed tomography perfusion core in large vessel occlusion in delayed time windows[J]. Stroke, 2021, 52(2): 498-504. doi: 10.1161/STROKEAHA.120.030353 [4] Trillo S, Ramos MC, Aguirre C, et al. Assessment of collateral circulation using perfusion CT in middle cerebral artery thrombectomy-treated patients[J]. J Stroke Cerebrovasc Dis, 2020, 29(7): 104805. doi: 10.1016/j.jstrokecerebrovasdis.2020.104805 [5] Rava RA, Snyder KV, Mokin M, et al. Assessment of computed tomography perfusion software in predicting spatial location and volume of infarct in acute ischemic stroke patients: a comparison of Sphere, Vitrea, and RAPID[J]. J Neurointerv Surg, 2021, 13(2): 130-5. doi: 10.1136/neurintsurg-2020-015966 [6] 中华医学会神经病学分会, 中华医学会神经病学分会脑血管病学组, 彭斌, 等. 中国急性缺血性脑卒中诊治指南2018[J]. 中华神经科杂志, 2018, 51(9): 666-82. https://www.cnki.com.cn/Article/CJFDTOTAL-XDJB201911024.htm [7] 中华医学会神经病学分会, 中华医学会神经病学分会脑血管病学组. 中国脑血管病影像应用指南2019[J]. 中华神经科杂志, 2020, 53(4): 250-68. https://www.cnki.com.cn/Article/CJFDTOTAL-YYCY202019002.htm [8] van Swieten JC, Koudstaal PJ, Visser MC, et al. Interobserver agreement for the assessment of handicap in stroke patients[J]. Stroke, 1988, 19(5): 604-7. doi: 10.1161/01.STR.19.5.604 [9] 王航, 宋歌, 谢万福. 早期脑血流量检测在预测蛛网膜下腔出血迟发性脑缺血患者预后的作用研究[J]. 国际神经病学神经外科学杂志, 2018, 45(2): 128-32. https://www.cnki.com.cn/Article/CJFDTOTAL-GWSK201802006.htm [10] 罗路, 谢鸿宇, 吴毅. 脑缺血损伤后小脑血流变化及其神经调控的研究进展[J]. 中国康复医学杂志, 2020, 35(11): 1381-4. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGKF202011024.htm [11] Li L, Zhi DY, Cheng RB, et al. The neuroprotective role of SIRT1/PGC-1α signaling in limb postconditioning in cerebral ischemia/reperfusion injury[J]. Neurosci Lett, 2021, 749: 135736. doi: 10.1016/j.neulet.2021.135736 [12] Pozzi-Mucelli RA, Furlanis G, Caruso P, et al. A novel fast CT perfusion core-penumbra mismatch score: correlation with stroke outcome[J]. Neurologist, 2021, 26(2): 41-6. doi: 10.1097/NRL.0000000000000315 [13] 杨迪, 周加华, 白万胜. CTP与DWI检查在急性脑梗死缺血半暗带中的应用价值[J]. 医学临床研究, 2021, 38(12): 1846-9. [14] Haranhalli N, Mbabuike N, Grewal SS, et al. Topographic correlation of infarct area on CT perfusion with functional outcome in acute ischemic stroke[J]. J Neurosurg, 2019, 132(1): 33-41. [15] Choi IA, Yun JH, Kim JH, et al. Sequential transcriptome changes in the penumbra after ischemic stroke[J]. Int J Mol Sci, 2019, 20 (24): 6349. [16] Dekker L, Venema E, Pirson FAV, et al. Endovascular treatment in anterior circulation stroke beyond 6.5 hours after onset or time last seen well: results from the MR CLEAN Registry[J]. Stroke Vasc Neurol, 2021, 6(4): 572-80. [17] Lee KY, Kim JW, Park M, et al. Interpretation of fluid-attenuated inversion recovery vascular hyperintensity in stroke[J]. J Neuroradiol, 2022, 49(3): 258-66. [18] Hong L, Cheng X, Lin LT, et al. The blood pressure paradox in acute ischemic stroke[J]. Ann Neurol, 2019, 85(3): 331-9. [19] 韦丹, 赵静, 党超, 等. 一站式CTP对预测急性脑梗死患者预后的评估价值[J]. 中山大学学报: 医学科学版, 2021, 42(2): 279-86. https://www.cnki.com.cn/Article/CJFDTOTAL-ZSYK202102017.htm -

 点击查看大图
点击查看大图
计量
- 文章访问数: 192
- HTML全文浏览量: 123
- PDF下载量: 7
- 被引次数: 0