



Efficacy and CT manifestations of IMRT combined with chemotherapy in the treatment of esophageal cancer
-
摘要:
目的 探究调强适形放疗(IMRT)技术同步化疗治疗食管癌的效果及CT表现。 方法 选取2020年5月~2021年5月重庆市开州区人民医院收治的134例食管癌患者,将其随机分为同步放化疗组(n=68)和联合调强适形放疗组(n=68),同步放化疗组给予三维适形放疗同步化疗,联合调强适形放疗组给予IMRT技术同步化疗。比较两组临床疗效和CT表现、免疫球蛋白[免疫球蛋白A(IgA)、免疫球蛋白M(IgM)、免疫球蛋白G(IgG)]、血管内皮生长因子(VEGF)及其受体1(VEGFR-1)、血清肿瘤标志物[癌胚抗原(CEA)、鳞状上皮细胞癌抗原(SCC-Ag)、糖类抗原125(CA125)]及不良反应。 结果 联合调强适形放疗组总有效率高于同步放化疗组(P < 0.05),CT可用于评估患者临床疗效;治疗后与同步放化疗组相比,联合调强适形放疗组IgA、IgM、IgG水平较高(P < 0.05),VEGF和VEGFR-1水平较低(P < 0.05),CEA、SCC-Ag、CA125水平较低(P < 0.05);两组不良反应总发生率差异无统计学意义(P>0.05)。 结论 IMRT技术同步化疗治疗食管癌患者具有较好的疗效,对患者免疫球蛋白水平影响更小,还可下调VEGF和VEGFR-1水平,降低血清肿瘤标志物水平,安全性较好。 Abstract:Objective To investigate the efficacy and CT manifestations of intensity-modulated radiotherapy (IMRT) combined with chemotherapy in the treatment of esophageal cancer. Methods A total of 134 patients with esophageal cancer admitted to Chongqing Kaizhou District People's Hospital from May 2020 to May 2021 were selected. They were randomly divided into concurrent chemoradiotherapy group (n=68) and combined with intensity-modulated radiotherapy group (n=68). The concurrent chemoradiotherapy group was given three-dimensional conformal radiotherapy combined with chemotherapy, while the combined with intensity-modulated radiotherapy group was given IMRT combined with chemotherapy. The clinical efficacy and CT manifestations, immunoglobulin [immunoglobulin A (IgA), IgM and IgG], vascular endothelial growth factor (VEGF) and its receptor 1 (VEGFR-1), serum tumor markers (CEA, SCC-AG, CA125) and adverse reactions were compared between the two groups. Results The total effective rate of combined with intensity-modulated radiotherapy group was significantly higher than that of concurrent chemoradiotherapy group (P < 0.05). CT could be used to evaluate the clinical efficacy of patients. After treatment, compared with the concurrent chemoradiotherapy group, the levels of IgA, IgM and IgG in the combined with intensity-modulated radiotherapy group were significantly higher (P < 0.05), the levels of VEGF and VEGFR-1 were significantly lower (P < 0.05), and the levels of CEA, SCC-AG and CA125 were significantly lower (P < 0.05). There was no difference in the total incidence of adverse reactions between the two groups (P>0.05). Conclusion IMRT combined with chemotherapy has good efficacy in the treatment of esophageal cancer patients and less effect on the level of immunoglobulin. It can also down-regulate the levels of VEGF and VEGFR-1, reduce the level of serum tumor markers, and has good safety. -

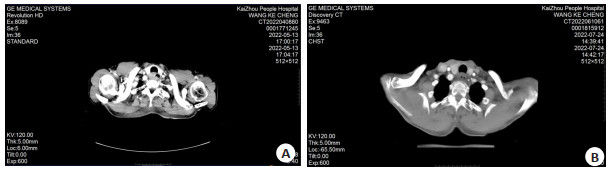
图 1 患者1 IMRT技术同步化疗治疗前后CT图
A: 治疗前; B: 治疗后.
Figure 1. CT images of patient 1 before and after IMRT concurrent chemotherapy.

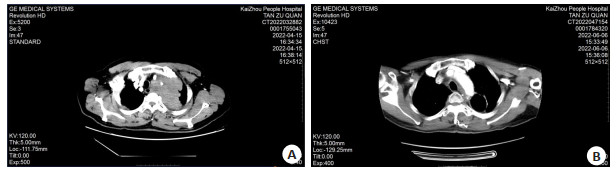
图 2 患者2 IMRT技术同步化疗治疗前后CT图
A: 治疗前; B: 治疗后.
Figure 2. CT images of patient 2 before and after IMRT concurrent chemotherapy.

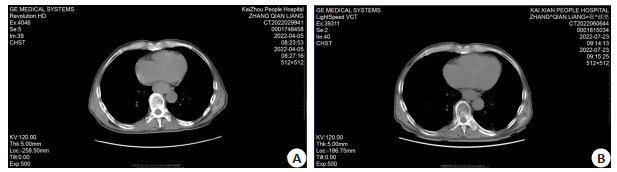
图 3 患者3 IMRT技术同步化疗治疗前后CT图
A: 治疗前; B: 治疗后.
Figure 3. CT images of patient 3 before and after IMRT concurrent chemotherapy.
表 1 两组一般资料比较
Table 1. Comparison of general data between the two groups (n=68)
资料 联合调强适形放疗组 同步放化疗组 t/χ2/Z P 性别(n) 1.063 0.303 男 39 33 女 29 35 年龄(岁, Mean±SD) 52.25±9.20 53.12±8.87 0.561 0.576 临床分期(n) 0.284 0.777 Ⅰ期 24 18 Ⅱ期 27 37 Ⅲ期 17 13 病理类型(n) 0.766 0.382 鳞癌 63 60 腺癌 5 8  下载: 导出CSV
下载: 导出CSV
表 2 临床疗效比较
Table 2. Comparison of clinical efficacy [n=68, n(%)]
组别 总有效率 进展 稳定 完全缓解 部分缓解 联合调强适形放疗组 61(89.71) 7(10.29) 16(23.53) 18(26.47) 27(39.71) 同步放化疗组 52(76.47) 16(23.53) 21(30.88) 12(17.65) 19(27.94) χ2 4.239 P 0.040
下载: 导出CSV
表 3 免疫球蛋白水平比较
Table 3. Comparison of immunoglobulin levels (g/L, n=68, Mean±SD)
组别 IgG IgA IgM 治疗前 治疗后 治疗前 治疗后 治疗前 治疗后 联合调强适形放疗组 11.40±1.24 10.08±0.95* 1.77±0.29 1.65±0.22* 1.54±0.16 1.45±0.12* 同步放化疗组 11.15±1.28 9.47±1.10* 1.73±0.32 1.45±0.18* 1.58±0.19 1.23±0.17* t 1.157 3.460 0.764 5.802 1.328 8.718 P 0.249 0.001 0.446 < 0.001 0.187 < 0.001 *P < 0.05 vs治疗前. IgG: 免疫球蛋白G; IgA: 免疫球蛋白A; IgM: 免疫球蛋白M.
下载: 导出CSV
表 4 VEGF和VEGFR-1水平比较
Table 4. Comparison of VEGF and VEGFR-1 levels (ng/L, n=68, Mean±SD)
组别 VEGF VEGFR-1 治疗前 治疗后 治疗前 治疗后 联合调强适形放疗组 970.34±194.56 570.39±151.25* 120.25±33.37 96.94±21.17* 同步放化疗组 985.69±202.49 673.43±185.62* 124.48±30.52 106.65±25.52* t 0.451 3.549 0.771 2.415 P 0.653 0.001 0.442 0.017 *P < 0.05 vs治疗前. VEGF: 血管内皮生长因子; VEGFR-1: 血管内皮生长因子受体1.
下载: 导出CSV
表 5 血清肿瘤标志物
Table 5. Serum tumor markers (n=68, Mean±SD)
组别 CEA(ng/mL) SCC-Ag(ng/mL) CA125(U/mL) 治疗前 治疗后 治疗前 治疗后 治疗前 治疗后 联合调强适形放疗组 29.72±5.10 20.25±4.56* 54.73±7.10 36.17±5.82* 82.25±17.59 31.52±10.12 同步放化疗组 30.22±5.05 24.59±4.80* 55.67±6.74 44.28±6.57* 81.02±16.51 49.54±15.86 t 0.574 5.406 0.792 7.619 0.420 7.899 P 0.567 < 0.001 0.430 < 0.001 0.675 < 0.001 *P < 0.05 vs治疗前. CEA: 癌胚抗原; CA125: 糖类抗原125; SCC-Ag: 鳞状上皮细胞癌抗原.
下载: 导出CSV
表 6 不良反应比较
Table 6. Comparison of adverse reactions [n=68, n(%)]
组别 脱发 骨髓抑制 恶心呕吐 乏力 总发生率 联合调强适形放疗组 5(7.35) 3(4.41) 6(8.82) 5(7.35) 19(27.94) 同步放化疗组 7(10.29) 4(5.88) 4(5.88) 6(8.82) 21(30.88) χ2 0.142 P 0.707
下载: 导出CSV
-
[1] Huang FL, et al. Esophageal cancer: risk factors, genetic association, and treatment[J]. Asian J Surg, 2018, 41(3): 210-5. doi: 10.1016/j.asjsur.2016.10.005 [2] Ferlay J, Colombet M, Soerjomataram I, et al. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods[J]. Int J Cancer, 2019, 144(8): 1941-53. doi: 10.1002/ijc.31937 [3] Tang Y, Yang L, Qin W, et al. Impact of genetic variant of HIPK2 on the risk of severe radiation pneumonitis in lung cancer patients treated with radiation therapy[J]. Radiat Oncol, 2020, 15(1): 9. doi: 10.1186/s13014-019-1456-0 [4] Zhang MS, Wu AJ. Radiation techniques for esophageal cancer[J]. Chin Clin Oncol, 2017, 6(5): 45. doi: 10.21037/cco.2017.06.33 [5] 滕菲, 孙晓静, 田媛, 等. 食管癌三维适形放疗前后肺功能、生活质量的变化及放射性肺炎的影响因素分析[J]. 现代生物医学进展, 2021, 21(6): 1120-4. doi: 10.13241/j.cnki.pmb.2021.06.027 [6] 刘杨, 王昆仑, 袁翎. 151例食管癌调强放疗疗效及预后影响因素分析[J]. 中华实用诊断与治疗杂志, 2015, 29(8): 791-3. doi: 10.13507/j.issn.1674-3474.2015.08.023 [7] Zhou X, et al. Survival impact of increasing time to IMRT initiation following induction chemotherapy in nasopharyngeal carcinoma: a propensity score-matched analysis[J]. Oral Oncol, 2021, 122: 105506. doi: 10.1016/j.oraloncology.2021.105506 [8] 中国医师协会放射肿瘤治疗医师分会, 中华医学会放射肿瘤治疗学分会, 中国抗癌协会肿瘤放射治疗专业委员会. 中国食管癌放射治疗指南(2019年版[) J]. 国际肿瘤学杂志, 2019, 46(7): 385-98. doi: 10.3760/cma.j.issn.1673-422X.2019.07.001 [9] 殷蔚伯, 余子豪, 徐国镇, 胡逸民. 肿瘤放射治疗学[M]. 4版. 北京: 中国协和医科大学出版社, 2008: 1200-1206. [10] Troeller A, et al. Comparison and limitations of DVH-based NTCP models derived from 3D-CRT and IMRT data for prediction of gastrointestinal toxicities in prostate cancer patients by using propensity score matched pair analysis[J]. Int J Radiat Oncol, 2015, 91(2): 435-43. doi: 10.1016/j.ijrobp.2014.09.046 [11] 杜峰, 王光明, 魏曾曾. 调强放疗同步替吉奥或卡培他滨化疗治疗中老年晚期食管癌的临床研究[J]. 中国医刊, 2022, 57(4): 389-92. doi: 10.3969/j.issn.1008-1070.2022.04.012 [12] Matsumoto T, Toya R, Shimohigashi Y, et al. Plan quality comparisons between 3D-CRT, IMRT, and VMAT based on 4D-CT for gastric MALT lymphoma[J]. Anticancer Res, 2021, 41(8): 3941-7. doi: 10.21873/anticanres.15190 [13] 李日著, 高洁, 农峰, 等. 食管癌患者血清白细胞介素和免疫球蛋白水平检测及其临床意义[J]. 中国医药导报, 2021, 18(14): 89-92, 110. https://www.cnki.com.cn/Article/CJFDTOTAL-YYCY202114023.htm [14] 何栋成, 韩济华, 曹磊, 等. IMRT及3D-CRT对早期NSCLC患者的治疗效果和对肿瘤标记物及免疫功能的影响[J]. 医学临床研究, 2018, 35(11): 2107-10. doi: 10.3969/j.issn.1671-7171.2018.11.009 [15] Ye X, Abou-Rayyah Y, Bischoff J, et al. Altered ratios of pro-and anti-angiogenic VEGF-A variants and pericyte expression of DLL4 disrupt vascular maturation in infantile haemangioma[J]. J Pathol, 2016, 239(2): 139-51. doi: 10.1002/path.4715 [16] 杨勇. SCC-Ag、CA19-9、VEGF在晚期食管鳞癌化疗疗效判断中的价值[J]. 检验医学, 2021, 36(1): 20-4. doi: 10.3969/j.issn.1673-8640.2021.01.004 [17] 魏磊, 唐正中, 强铭, 等. TP联合替吉奥胶囊对中晚期食管癌患者的临床疗效及血清VEGF、VEGFR-1的影响[J]. 川北医学院学报, 2020, 35(4): 717-20. doi: 10.3969/j.issn.1005-3697.2020.04.41 [18] 王佳龙, 杨超, 顾春荣, 等. 调强适形放疗联合三氧疗法对鼻咽癌患者免疫功能及氧化应激指标的影响[J]. 癌症进展, 2021, 19(4): 373-6, 387. https://www.cnki.com.cn/Article/CJFDTOTAL-AZJZ202104013.htm [19] 倪峰, 徐健, 邰国梅, 等. 复方苦参注射液联合放疗治疗老年中晚期食管癌临床疗效及对患者血清CEA、CA199及CA50水平的影响[J]. 湖北中医药大学学报, 2022, 24(1): 38-41. https://www.cnki.com.cn/Article/CJFDTOTAL-HZXX202201009.htm [20] Qiao YF, Chen CG, Yue J, et al. Tumor marker index based on preoperative SCC and CYFRA 21-1 is a significant prognostic factor for patients with resectable esophageal squamous cell carcinoma[J]. Cancer Biomark, 2019, 25(3): 243-50. [21] 鲁为山, 陈晟, 方军. 复方苦参注射液联合放化疗对老年食管癌患者血清CEA、CA199和CA125水平及细胞免疫功能的影响[J]. 中国老年学杂志, 2020, 40(6): 1186-9. doi: 10.3969/j.issn.1005-9202.2020.06.022 [22] Robelin P, et al. Comparative analysis of predictive values of the kinetics of 11 circulating miRNAs and of CA125 in ovarian cancer during first line treatment (a GINECO study)[J]. Gynecol Oncol, 2020, 159(1): 256-63. [23] 王皓颖, 赵一电, 梁垲, 等. 调强适形放疗与三维适形放疗对局部晚期非小细胞肺癌患者肿瘤标志物及预后的影响[J]. 右江医学, 2021, 49(9): 677-82. https://www.cnki.com.cn/Article/CJFDTOTAL-YJYX202109011.htm [24] Bergsma DP, Salama JK, Singh DP, et al. The evolving role of radiotherapy in treatment of oligometastatic NSCLC[J]. Expert Rev Anticancer Ther, 2015, 15(12): 1459-71. [25] 王新森, 王燕霞, 李鸣鹤, 等. 调强放疗和三维适形放疗治疗局部晚期直肠癌的近远期效果及安全性[J]. 中国实用医刊, 2019, 46(9): 55-9. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 159
- HTML全文浏览量: 88
- PDF下载量: 4
- 被引次数: 0