



Establishment of microsatellite instability assessment model for endometrial carcinoma by clinic-imaging omics
-
摘要:
目的 探讨应用临床因素联合影像组学建立子宫内膜癌(EC)微卫星不稳定性(MSI)评估模型的价值。 方法 回顾性分析2018年6月~2022年1月手术前经MR影像学检查及手术后病理学检测确诊为EC的患者68例,收集患者影像学及临床病理资料,根据患者微卫星稳定情况将患者分为不稳定组(n=27)和稳定组(n=41)。临床模型构建采用Logistic回归分析对临床因素进行筛选,影像组学模型构建采用3DSlicer软件勾画病灶感兴趣区并提取影像组学特征,利用最小绝对收缩和选择算子算法进行特征降维。绘制ROC曲线对影像组学模型、临床模型和临床-影像联合模型进行预测效能评估,并使用Delong检验比较3种模型的预测效能是否具有统计学差异。 结果 Logistic回归分析显示,错配修复蛋白MutL同源物1、减数分裂后分离蛋白表达和肿瘤分化程度、肌层侵犯深度是EC MSI的临床危险因素。筛选6个影像组学特征用于构建影像组学模型(P < 0.05)。经ROC曲线分析,临床-影像联合模型在EC MSI中具有较好的预测及评估性能(P < 0.05),临床模型、影像组学模型及临床-影像联合模型AUC分别为0.871、0.932、0.981。Delong检验结果显示临床-影像联合模型和影像组学模型与临床模型比较,差异有统计学意义(Z=1.933、2.735,P=0.046、0.006)。 结论 应用临床因素联合MR影像组学特征建立的评估模型对EC MSI具有较好的预测价值。 Abstract:Objective To investigate the value of microsatellite instability (MSI) assessment model of endometrial carcinoma (EC) established by clinical factors combined with imaging omics. Methods Sixty- eight patients with EC diagnosed by preoperative MR imaging and postoperative pathological examination from June 2018 to January 2022 were retrospectively analyzed, with imaging and clinicopathologic data collected. Patients were divided into unstable group (n=27) and stable group (n=41) according to microsatellite stability. Logistic regression analysis was used to screen the clinical factors. ITK-SNAP software was used to delineate the region of interest of the lesion and extract the image omics characteristics. The minimum absolute contraction and selection operator algorithm were used for feature dimension reduction. ROC curve was plotted to assess the predictive power of the image-omics model, the clinical model, and the combined clinical-imaging model, and Delong test was used to compare the predictive power of the three models. Results Logistic regression analysis showed that mismatch repair protein MutL homolog 1, post-meiotic segregation protein 2 expression, tumor differentiation and depth of myometrial invasion were clinical risk factors of EC MSI. Six image-omics features were screened for construction of imageomics models (P < 0.05). Through ROC curve analysis, the combined clinic-image model had good prediction and evaluation performance in EC MSI, and the AUCs of the clinical model, the image-omics model, and the combined clinic-image model were 0.871, 0.932 and 0.981, respectively. The results of Delong test showed that the difference between the clinical imaging combined model and the imaging omics model and the clinical model was statistically significant (Z=1.933, 2.735, P=0.046, 0.006). Conclusion The assessment model established by clinical factors combined with MR imaging omics characteristics has a good predictive value for EC MSI. -

图 1 某55岁患者,手术治疗前MR影像
Figure 1. MR images of a 55-year-old patient, before surgical treatment.

图 2 某74岁患者,手术治疗前MR影像
Figure 2. MR image of a 74-year-old patient, before surgical treatment.
表 1 临床病理特征单因素分析
Table 1. Single factor analysis of clinical and pathological characteristics
因素 不稳定组(n=27) 稳定组(n=41) t/χ2 P 年龄(岁,Mean±SD) 46.56±8.26 47.13±7.74 0.289 0.773 肿瘤分化程度[n(%)] 9.811 0.007 高分化 7(25.9) 22(53.7) 中分化 8(29.6) 14(34.1) 低分化 12(44.5) 5(12.2) BMI(kg/m2, Mean±SD) 28.54±4.67 27.95±4.32 0.534 0.595 FIGO分期[n(%)] 0.957 0.328 Ⅰ~Ⅱ撕 16(59.3) 29(70.7) Ⅲ~Ⅳ期 11(40.7) 12(29.3) 肌层侵犯深度[n(%)] 6.502 0.011 < 1/2层 13(48.2) 32(78.0) ≥ 1/2层 14(51.8) 9(22.0) MMRP阳性表达情况[n(%)] MLH1 19(70.4) 40(97.6) 8.247 0.004 MSH2 23(85.2) 39(95.2) 0.954 0.329 MSH6 25(92.6) 41(100.0) 2.417 0.120 PMS2 8(29.6) 41(100.0) 40.040 < 0.001 淋巴结转移[n(%)] 0.207 0.649 无 17(63.0) 28(68.3) 有 10(37.0) 13(31.7) MMRP: 错配修复蛋白; MLH1: MutL同源物1; MSH2: MutS同源物2; MSH6:MutS同源物6; PMS2:减数分裂后分离蛋白.  下载: 导出CSV
下载: 导出CSV
表 2 临床病理特征Logistic回归分析
Table 2. Logistic regression analysis of clinical and pathological characteristics
因素 B SE P OR 95% CI 肿瘤分化程度 1.005 0.265 < 0.001 2.732 1.704~4.813 肌层侵犯深度 0.688 0.265 0.010 1.989 1.324~3.746 MLH1 0.836 0.237 < 0.001 2.307 1.685~4.268 PMS2 1.525 0.478 0.001 4.593 2.305~15.020
下载: 导出CSV
表 3 不同评估模型对MSI诊断的卡方拟合优度检验
Table 3. Chi square goodness of fit test of different evaluation models for MSI diagnosis [n=68, n(%)]
模型 MSI χ2 P 标准值 27(39.7) - - 临床模型 22(32.4) 1.533 0.216 影像组学模型 24(35.3) 0.551 0.458 临床-影像模型 26(38.2) 0.061 0.805 MSI: 微卫星不稳定性.
下载: 导出CSV
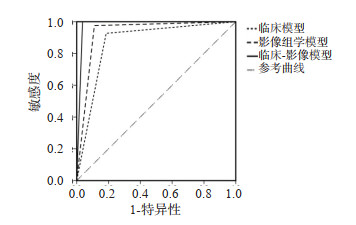
表 4 不同评估模型预测效能分析
Table 4. Prediction Effectiveness Analysis of Different Evaluation Models
模型 AUC 标准误 P 敏感度(%) 特异性(%) 临床模型 0.871 0.050 < 0.001 92.7 81.5 影像组学模型 0.932 0.038 < 0.001 97.6 88.9 临床-影像模型 0.981 0.021 < 0.001 100.0 96.3
下载: 导出CSV
-
[1] 王芬芬, 谢幸. 子宫内膜癌的病因及高危因素[J]. 实用妇产科杂志, 2020, 36(6): 401-3. https://www.cnki.com.cn/Article/CJFDTOTAL-SFCZ202006001.htm [2] 田士峰, 刘爱连, 陈丽华, 等. 磁敏感序列多定量参数预测子宫内膜癌微卫星不稳定状态[J]. 磁共振成像, 2020, 11(7): 493-6. https://www.cnki.com.cn/Article/CJFDTOTAL-CGZC202007006.htm [3] 廖鸿力, 林鹏. 子宫内膜癌miR-129-2甲基化与微卫星不稳定性的关系研究[J]. 中国妇幼保健, 2021, 36(1): 168-72. https://www.cnki.com.cn/Article/CJFDTOTAL-ZFYB202101059.htm [4] Wu XY, Snir O, Rottmann D, et al. Minimal microsatellite shift in microsatellite instability high endometrial cancer: a significant pitfall in diagnostic interpretation[J]. Mod Pathol, 2019, 32(5): 650-8. doi: 10.1038/s41379-018-0179-3 [5] 中国抗癌协会妇科肿瘤专业委员会. 妇科恶性肿瘤多学科诊疗中国专家共识(2022年版)[J]. 中国癌症杂志, 2022, 32(8): 747-56. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGAZ202208013.htm [6] 朱炜宇, 张青陵, 张绪霞, 等. 基于超声的影像组学在常见肿瘤应用中的研究进展[J]. 中国医疗设备, 2022, 37(2): 164-7, 178. doi: 10.3969/j.issn.1674-1633.2022.02.038 [7] 刘旭, 冯卫华, 王涛, 等. 临床-影像组学联合模型对直肠癌微卫星不稳定性的预测价值[J]. 精准医学杂志, 2022, 37(4): 326-31. https://www.cnki.com.cn/Article/CJFDTOTAL-SPAN202204009.htm [8] 肖婧, 吴颖. 子宫内膜癌患者微卫星不稳定性及其临床意义研究[J]. 中国全科医学, 2022, 25(3): 275-9, 284. https://www.cnki.com.cn/Article/CJFDTOTAL-QKYX202203024.htm [9] 中国抗癌协会妇科肿瘤专业委员会. 子宫内膜癌诊断与治疗指南(2021年版)[J]. 中国癌症杂志, 2021, 31(6): 880-6. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGAZ202106008.htm [10] 林仲秋. FIGO/IGCS妇科恶性肿瘤分期及临床实践指南(四): 子宫内膜癌[J]. 国际妇产科学杂志, 2008, 35(4): 303-4. https://www.cnki.com.cn/Article/CJFDTOTAL-GWVC200804027.htm [11] 于文亮, 潘长清, 郑茜文. 子宫内膜癌组织中错配修复蛋白的表达情况及与患者免疫功能和微卫星不稳定的关系[J]. 癌症进展, 2020, 18 (12): 1248-52. https://www.cnki.com.cn/Article/CJFDTOTAL-AZJZ202012015.htm [12] 石洪堂, 刘志强, 孟玮, 等. 微卫星不稳定对子宫内膜样癌组织PDL1和CD8表达影响及意义[J]. 中华肿瘤防治杂志, 2020, 27(12): 958-62, 985. https://www.cnki.com.cn/Article/CJFDTOTAL-QLZL202012007.htm [13] 何翊姣, 陈茜, 王建六. Lynch综合征相关性子宫内膜癌的研究进展[J]. 中国妇产科临床杂志, 2021, 22(2): 209-11. https://www.cnki.com.cn/Article/CJFDTOTAL-FKLC202102041.htm [14] 戴一博, 王婧元, 赵路阳, 等. 子宫内膜癌DNA错配修复基因异常的相关研究进展[J]. 中华妇产科杂志, 2019, 54(12): 869-72. [15] 李碧岚, 黄宇佳, 万小平. 子宫内膜癌患者错配修复基因表达与微卫星不稳定性和临床病理特征相关性分析[J]. 肿瘤药学, 2020, 10(5): 559-63. https://www.cnki.com.cn/Article/CJFDTOTAL-LIYX202005010.htm [16] 曾嘉敏, 黎相照, 廖德贵, 等. 子宫内膜癌微卫星稳定性检测分析[J]. 诊断病理学杂志, 2022, 29(7): 577-81. https://www.cnki.com.cn/Article/CJFDTOTAL-ZDBL202207001.htm [17] 张立英, 乔星, 祁晓莉, 等. 子宫内膜癌错配修复蛋白表达与临床病理特征的关系分析[J]. 中国妇产科临床杂志, 2019, 20(4): 356-8. https://www.cnki.com.cn/Article/CJFDTOTAL-FKLC201904020.htm [18] 方如旗, 薛晓铃, 章国伟, 等. 建立MRI影像组学列线图术前预测子宫内膜癌浸润深肌层[J]. 中国医学影像技术, 2022, 38(4): 561-5. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYXX202204016.htm [19] 孙伟杰, 彭海霞. 微卫星不稳定性与结直肠癌的研究进展[J]. 胃肠病学, 2020, 25(1): 55-8. https://www.cnki.com.cn/Article/CJFDTOTAL-WIEC202001013.htm [20] 吴新军, 郜庆祖, 李岩, 等. 242例食管胃结合部腺癌患者Siewert分型、微卫星不稳定、HER2表达分析[J]. 国际外科学杂志, 2021(11): 769-73, F0004. [21] 邱燕如, 戴毅君, 戴炀斌, 等. 微卫星不稳定及免疫治疗在分化型甲状腺癌中的研究进展[J]. 中国肿瘤临床, 2020, 47(23): 1236-41. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGZL202023014.htm [22] 田士峰, 刘爱连, 郭妍, 等. 基于增强T2*加权血管成像序列R2*图肿瘤全域纹理分析预测子宫内膜癌微卫星不稳定性[J]. 中国医学影像技术, 2022, 38(2): 257-61. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYXX202202020.htm [23] 谢元亮, 杜丹, 谢伟, 等. DCE-MRI纹理分析鉴别宫颈鳞癌与腺癌及预测分级的价值[J]. 放射学实践, 2019, 34(8): 835-40. https://www.cnki.com.cn/Article/CJFDTOTAL-FSXS201908002.htm [24] Doghri R, Houcine Y, Boujelbène N, et al. Mismatch repair deficiency in endometrial cancer: immunohistochemistry staining and clinical implications[J]. Appl Immunohistochem Mol Morphol, 2019, 27(9): 678-82. [25] 王宏睿, 李金玲, 张强, 等. 磁共振表观扩散系数直方图和血清CA125有助于评估子宫内膜样腺癌的病理组织学特征[J]. 分子影像学杂志, 2022, 45(4): 480-5. doi: 10.12122/j.issn.1674-4500.2022.04.04 [26] 田士峰, 刘爱连, 刘静红, 等. 初探基于肿瘤全域ADC图的灰度共生矩阵纹理分析与子宫内膜癌Ki-67表达的相关性[J]. 磁共振成像, 2019, 10(11): 826-9. https://www.cnki.com.cn/Article/CJFDTOTAL-CGZC201911009.htm -

 点击查看大图
点击查看大图
计量
- 文章访问数: 177
- HTML全文浏览量: 94
- PDF下载量: 8
- 被引次数: 0