



Effect of pre-radiotherapy NLR, PLR and LMR on the prognosis of patients with brain metastases and analysis of related factors
-
摘要:
目的 探讨放疗前外周血中性粒细胞-淋巴细胞比值(NLR)、血小板-淋巴细胞比值(PLR)及淋巴细胞-单核细胞比值(LMR)对脑转移患者全脑放疗预后的影响。 方法 回顾性纳入118例脑转移患者的临床资料,分析各个炎性复合指标和临床资料与脑转移瘤患者全脑放疗预后的关系。采用ROC曲线确定脑转移瘤患者全脑放疗预后NLR、PLR及LMR的临界值。采用Kaplan-Meier法进行单因素生存分析、Log-rank检验进行各组生存率之间的比较,采用Cox比例风险模型进行多因素回归分析。 结果 118例脑转移瘤患者的中位生存期为12.5月,1年、2年生存率分别为72.8%和50.1%。通过ROC曲线确定NLR、PLR和LMR的临界值分别为4.28、217.8和1.95。Kaplan-Meier单因素分析显示,肿瘤分期、靶向治疗、NLR、PLR以及LMR均是影响脑转移瘤患者全脑放疗预后的危险因素(P=0.001、0.032、0.008、0.003、0.002),进一步多因素Cox回归分析表明PLR是唯一的独立不良预后因素(P=0.003)。 结论 放疗前外周血PLR升高是脑转移瘤患者全脑放疗的独立不良预后因素。 -
关键词:
- 脑转移 /
- 全脑放疗 /
- 中性粒细胞-淋巴细胞比值 /
- 血小板-淋巴细胞比值 /
- 淋巴细胞-单核细胞比值
Abstract:Objective To investigate the relationship between peripheral blood neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR) and lymphocyte to monocyte ratio (LMR) and prognosis of patients with brain metastases. Methods A total of 118 patients with brain metastases treated with whole brain radiotherapy were retrospectively analyzed. The relationship of NLR, PLR, LMR and clinical data with the prognosis patients were analyzed. Receiver operating characteristic curve was used to calculate the optimal cut-off values of NLR, PLR and LMR. The overall survival analysis was performed by Kaplan- Meier method. Significant differences were analyzed by Log-rank test. Multivariate analysis for survival was performed by Cox proportional regression model. Results The median overall survival time of 188 patients with brain metastases was 12.5 months. The 1-year, 2-year survival rates were 72.8% and 50.1%, respectively. The optimal cut-off values of NLR, PLR and LMR were determined by ROC curve to be 4.28, 217.8 and 1.95, respectively. The tumor stage, targeted therapy, NLR, PLR, and LMR were all associated with the prognosis of patients with brain metastases (P=0.001, 0.032, 0.008, 0.003, 0.002). The PLR were an independent prognostic factors for the patients with brain metastases (P=0.003). Conclusion The peripheral blood PLR before whole brain radiotherapy may be an independent prognostic factor in the patients with brain metastases. -

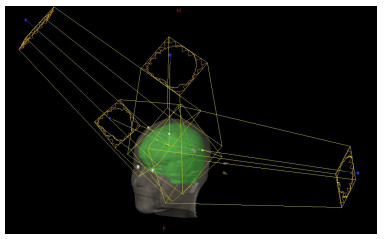
图 1 脑转移瘤患者全脑调强放疗计划布野示意图
Figure 1. Schematic diagram of intensity-modulated radiotherapy plan for patient metastasis.

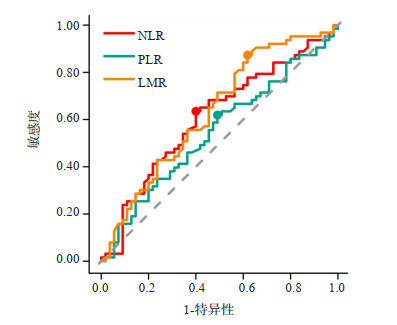
图 2 脑转移瘤患者全脑放疗预后NLR、PLR及LMR的受试者工作特征曲线
Figure 2. Receiver operating characteristic curve of the patients with brain metastasis treated with whole brain radiotherapy according to the NLR, PLR and LMR.

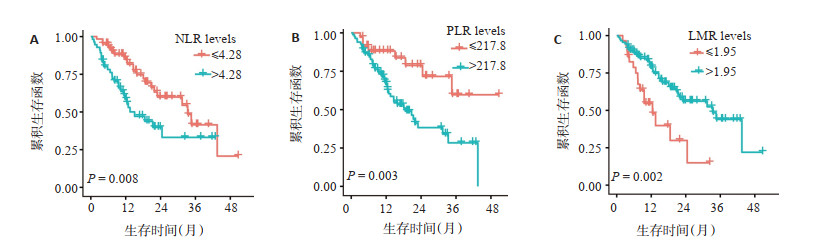
图 4 118例脑转移患者不同NLR(A)、PLR(B)、LMR(C)的生存曲线
Figure 4. Overall survival curves of 118 patients with brain metastasis treated with whole brain radiotherapy according to NLR (A), PLR(B), and LMR(C).
表 1 118例脑转移患者总生存期的单因素分析结果
Table 1. Univariate analyses of OS in 118 patients with brain metastases
临床特征 例数(n) χ2 P 临床特征 例数(n) χ2 P 性别 0.962 0.330 化疗 0.204 0.650 男 47 是 83 女 71 否 35 年龄(岁) 2.310 0.130 手术 2.97 0.085 ≤ 70 86 是 104 > 70 32 否 14 卡氏功能 0.625 0.430 靶向治疗 4.570 0.032 ≤ 70 67 是 79 > 70 51 否 39 脑转移数目 0.164 0.690 NLR 6.950 0.008 ≤ 3 31 ≤ 4.28 62 > 3 87 > 4.28 56 颅外转移 0.098 0.750 PLR 8.610 0.003 是 57 ≤ 217.8 35 否 61 > 217.8 83 肿瘤分期 10.300 0.001 LMR 9.980 0.002 T1~T2 61 ≤ 1.95 29 T3~T4 23 > 1.95 89 NLR: 中性粒细胞-淋巴细胞比值; PLR: 血小板-淋巴细胞比值; LMR: 淋巴细胞-单核细胞比值.  下载: 导出CSV
下载: 导出CSV
表 2 118例脑转移患者总生存期的多因素Cox回归分析
Table 2. Multivariate Cox risk regression model analysis of OS in 118 patients with brain metastases
临床因素 B S.E. Wald HR (95% CI) P 肿瘤分期(T3~T4 vs T1~T2) 1.046 0.564 -1.87 2.845 (0.942~8.588) 0.064 手术(是vs否) -0.657 0.709 -0.93 2.298(0.962~5.490) 0.354 靶向治疗(否vs是) -0.832 0.444 1.85 0.519 (0.129~2.082) 0.061 NLR (>4.28vs≤4.28) -0.524 0.735 -0.71 0.592 (0.140~2.500) 0.476 PLR (≤217.8vs>217.8) 2.012 0.670 3.00 0.134 (0.035~0.497) 0.003 LMR (≤1.95vs>1.95) -1.121 0.731 -1.53 3.067 (0.732~12.848) 0.125
下载: 导出CSV
-
[1] Patchell RA, et al. The management of brain metastases[J]. Cancer Treat Rev, 2003, 29(6): 533-40. doi: 10.1016/S0305-7372(03)00105-1 [2] 马玉超, 肖建平, 毕楠, 等. HT全脑+病灶同步推量放疗多发性脑转移瘤剂量学及临床分析[J]. 中华放射肿瘤学杂志, 2018, 27(5): 435-40. doi: 10.3760/cma.j.issn.1004-4221.2018.05.001 [3] Nieder C, Norum J, Stemland JG, et al. Resource utilization in patients with brain metastases managed with best supportive care, radiotherapy and/or surgical resection: a Markov analysis[J]. Oncology, 2010, 78(5/6): 348-55. [4] Gaspar LE, Mehta MP, Patchell RA, et al. The role of whole brain radiation therapy in the management of newly diagnosed brain metastases: a systematic review and evidence-based clinical practice guideline[J]. J Neurooncol, 2010, 96(1): 17-32. doi: 10.1007/s11060-009-0060-9 [5] 韩雪, 李红梅. 非小细胞肺癌脑转移治疗的研究进展[J]. 中国肺癌杂志, 2020, 23(12): 1087-94. doi: 10.3779/j.issn.1009-3419.2020.102.39 [6] Zhou C, Shan CG, Lai MY, et al. Individualized nomogram for predicting survival in patients with brain metastases after stereotactic radiosurgery utilizing driver gene mutations and volumetric surrogates[J]. Front Oncol, 2021, 11((5)): 659538. [7] Proctor MJ, McMillan DC, Morrison DS, et al. A derived neutrophil to lymphocyte ratio predicts survival in patients with cancer[J]. Br J Cancer, 2012, 107(4): 695-9. doi: 10.1038/bjc.2012.292 [8] Md BA, Md JP, et al. Usefulness of the neutrophil-to-lymphocyte ratio in predicting short-and long-term mortality in breast cancer patients[J]. Ann Surg Oncol, 2012, 19(1): 217-24. doi: 10.1245/s10434-011-1814-0 [9] Kao SCH, Pavlakis N, Harvie R, et al. High blood neutrophil-tolymphocyte ratio is an indicator of poor prognosis in malignant mesothelioma patients undergoing systemic therapy[J]. Clin Cancer Res, 2010, 16(23): 5805-13. doi: 10.1158/1078-0432.CCR-10-2245 [10] Grimes N, Hannan C, Tyson M, et al. The role of neutrophillymphocyte ratio as a prognostic indicator in patients undergoing nephrectomy for renal cell carcinoma[J]. Can Urol Assoc J, 2018, 12(7): E345-E348. [11] Sarraf KM, et al. Neutrophil/lymphocyte ratio and its association with survival after complete resection in non-small cell lung cancer [J]. J Thorac Cardiovasc Surg, 2009, 137(2): 425-8. doi: 10.1016/j.jtcvs.2008.05.046 [12] Zheng J, Cai JY, Li H, et al. Neutrophil to lymphocyte ratio and platelet to lymphocyte ratio as prognostic predictors for hepatocellular carcinoma patients with various treatments: a Metaanalysis and systematic review[J]. Cell Physiol Biochem, 2017, 44 (3): 967-81. doi: 10.1159/000485396 [13] Kim SI. The author's reply: prognostic significance of preoperative and follow-up neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in patients with non-metastatic clear cell renal cell carcinoma[J]. Investig Clin Urol, 2019, 60(4): 332. doi: 10.4111/icu.2019.60.4.332 [14] Schneider M, Schäfer N, Bode C, et al. Prognostic value of preoperative inflammatory markers in melanoma patients with brain metastases[J]. J Clin Med, 2021, 10(4): 634. doi: 10.3390/jcm10040634 [15] 贾纪云, 胡晓明, 邢向茹. 术前NLR、PLR、血清CEA与上皮性卵巢癌病理特征的关系及对预后的临床预测价值[J]. 实用癌症杂志, 2022, 37(8): 1359-62. https://www.cnki.com.cn/Article/CJFDTOTAL-SYAZ202208038.htm [16] 王琳, 吕喜英. 外周血中性粒细胞与淋巴细胞比值、血小板与淋巴细胞比值对小细胞肺癌患者预后的评估价值[J]. 临床肺科杂志, 2017, 22(6): 983-7. doi: 10.3969/j.issn.1009-6663.2017.06.004 [17] 冷建彬, 李凤虎, 常建英, 等. 乳腺癌患者治疗前血小板和血小板/淋巴细胞比值临床意义探讨[J]. 中华肿瘤防治杂志, 2018, 25(3): 189-96. https://www.cnki.com.cn/Article/CJFDTOTAL-QLZL201803009.htm [18] Wojtukiewicz MZ, Sierko E, Hempel D, et al. Platelets and cancer angiogenesis nexus[J]. Cancer Metastasis Rev, 2017, 36(2): 249-62. doi: 10.1007/s10555-017-9673-1 [19] Orellana R, Kato S, Erices R, et al. Platelets enhance tissue factor protein and metastasis initiating cell markers, and act as chemoattractants increasing the migration of ovarian cancer cells[J]. BMC Cancer, 2015, 15: 290. doi: 10.1186/s12885-015-1304-z [20] Mei Z, Liu Y, Liu C, et al. Tumour-infiltrating inflammation and prognosis in colorectal cancer: systematic review and meta-analysis [J]. Br J Cancer, 2014, 110(6): 1595-605. doi: 10.1038/bjc.2014.46 [21] Togashi Y, Shitara K, Nishikawa H. Regulatory T cells in cancer immunosuppression—implications for anticancer therapy[J]. Nat Rev Clin Oncol, 2019, 16(6): 356-71. doi: 10.1038/s41571-019-0175-7 [22] 赵贺, 王冲, 张文静, 等. 术前LSR、NLR及PLR检测评估结直肠癌预后的应用价值[J]. 分子诊断与治疗杂志, 2022, 14(2): 228-31, 236. https://www.cnki.com.cn/Article/CJFDTOTAL-YXYQ202202012.htm [23] Chen JH, Zhai ET, Yuan YJ, et al. Systemic immune-inflammation index for predicting prognosis of colorectal cancer[J]. World J Gastroenterol, 2017, 23(34): 6261-72. doi: 10.3748/wjg.v23.i34.6261 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 288
- HTML全文浏览量: 161
- PDF下载量: 20
- 被引次数: 0