



Efficacy of endoscopic decompression, fusion and internal fixation in the treatment of lumbar spinal stenosis
-
摘要:
目的 探讨脊柱内镜下减压融合内固定术治疗腰椎管狭窄症的疗效。 方法 选取2019年9月~2021年9月我院腰椎管狭窄症患者50例,将其随机分为观察组和对照组,25例1组,观察组给予全脊柱内镜下减压融合内固定术,对照组给予传统开放性手术治疗。比较两组手术时间、术中出血量、住院时间,术后24、48、72 h手术切口疼痛视觉模拟量表(VAS)评分,术后3月、12月随访Oswestry功能障碍指数(ODI),术后12月随访融合率并观察术后并发症。 结果 观察组手术时间、术中出血量、住院时间优于对照组(P < 0.05),差异有统计学意义。两组患者术后24、48、72 h VAS评分差异有统计学意义(P < 0.05)。两组患者术后3月、12月随访ODI评分较术前明显改善(P < 0.05)。两组患者术后3月或12月融合节段Cobb角变化、术后12月融合率的差异无统计学意义(P > 0.05)。实验组并发症发生率为8%(2/25),对照组并发症发生率为12%(3/25),差异有统计学意义(P < 0.05)。 结论 脊柱内镜下椎管减压、腰椎间融合、经皮椎弓根钉术治疗腰椎管狭窄症的治疗效果明显优于传统手术。 -
关键词:
- 脊柱内镜 /
- 腰椎椎管狭窄 /
- 腰椎减压融合内固定术 /
- 微创
Abstract:Objective To investigate the efficacy of spinal endoscopic decompression fusion internal fixation in the treatment of lumbar spinal stenosis. Methods Fifty patients with lumbar spinal stenosis in our hospital from September 2019 to September 2021 were selected and randomly divided into the observation group (given total spinal endoscopic decompression fusion internal fixation) and the control group (given traditional open surgery), twenty-five cases/group. The operation time, intraoperative blood loss and hospital stay were compared. The visual analogue scale (VAS) score of incision pain was compared at 24, 48 and 72 hours after operation. The Oswestry disability index (ODI) and Cobb angle were followed up at 3 and 12 months after operation, and the fusion rate was observed at 12 months after operation. Postoperative complications were followed up 12 months after operation. Results The observation group was significantly better than the control group in terms of operative time, intraoperative bleeding and hospital stay (P < 0.05). There was a statistically significant difference in VAS scores at 24, 48 and 72 hours after surgery between the two groups (P < 0.05). The ODI scores at 3 and 12 months postoperative follow-up were significantly improved compared with those before surgery in both groups (P < 0.05). There was no statistically significant difference between the two groups in the change of Cobb angle of the fused segment at 3 or 12 months after surgery and the fusion rate at 12 months after surgery (P > 0.05). The complication rate was 8% (2/25) in the experimental group and 12% (3/25) in the control group, and the difference was statistically significant (P < 0.05). Conclusion The therapeutic effect of spinal endoscopic spinal decompression, lumbar interbody fusion, and percutaneous pedicle nailing for lumbar spinal stenosis are significantly better than that of traditional surgery. -

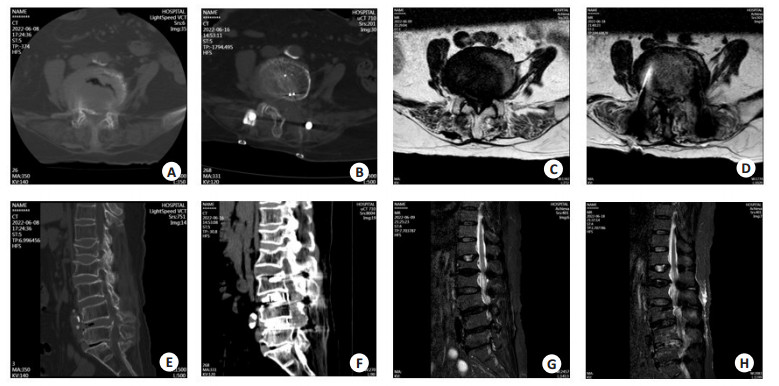
图 1 两组典型腰椎椎管狭窄症患者手术前后影像学表现
A~B: 患者男性, 术前磁共振显示L4/5腰椎椎管狭窄(A), 传统开放手术术后CT显示右侧椎板扩大减压(B). C~D: 患者女性,术前磁共振显示L4/5腰椎椎管狭窄(C); 全脊柱内镜下减压融合内固定术术后CT显示右侧椎板扩大减压(D).
Figure 1. Imaging examinations before and after surgery in two groups of typical lumbar spinal stenosis patients.

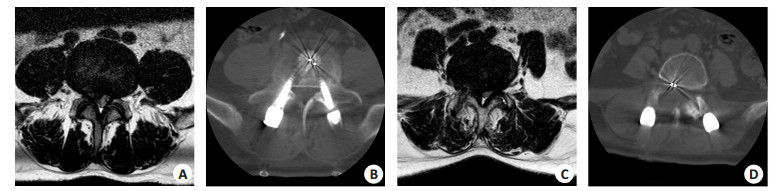
图 2 腰椎椎管狭窄症患者手术前后影像学检查(观察组典型病例)
A: 腰椎椎管狭窄症患者术前CT横断面; B: 腰椎椎管狭窄症患者术后CT横断面; C: 腰椎椎管狭窄症患者术前MR横断面; D: 腰椎椎管狭窄症患者术后MR横断面; E: 腰椎椎管狭窄症患者术前CT矢状位; F: 腰椎椎管狭窄症患者术后CT矢状位;G: 腰椎椎管狭窄症患者术前MR矢状位; H: 腰椎椎管狭窄症患者术后MR矢状位.
Figure 2. Imaging examinations before and after surgery in patients with lumbar spinal stenosis (typical cases in observation group).
表 1 两组一般资料对比
Table 1. Baseline data comparison between groups (n=25)
指标 观察组 对照组 χ2/t P 女性[n(%)] 14(56) 13(52) 0.081 0.777 年龄(岁,Mean±SD) 61.7±8.2 60.4±8.1 0.564 0.575 手术节段[n(%)] 0.082 0.774 L4~L5 15(60) 14(56) L5~SI 10(40) 11(44)  下载: 导出CSV
下载: 导出CSV
表 2 术中临床指标比较
Table 2. Intraoperative clinical indicators comparison (n=25, Mean±SD)
指标 观察组 对照组 χ2/t P 手术时间(min) 45.2±3.48 62.17±3.74 18.19 <0.001 术中出血(mL) 48.44±4.27 59.12±3.15 10.06 <0.001 住院时间(d) 5.87±1.13 7.34±1.66 3.66 <0.001
下载: 导出CSV
表 3 术后VAS评分及ODI比较
Table 3. Comparison of VAS and ODI between two groups of patients (n=25, Mean±SD)
指标 观察组 对照组 F组间 P组间 F组内 P组内 VAS 0.496 0.482 255.1 <0.001 术后24 h 4.22±1.21 3.92±0.78 术后48 h 2.46±0.97 2.59±0.72 术后72 h 0.66±0.36 0.84±0.34 ODI(%) 26.14 <0.001 650.1 <0.001 术前 31.42±4.78 30.8±4.55 术后3月 19.56±3.45 14.71±2.89 术后12月 9.71±2.27 7.25±1.79 VAS: 疼痛视觉模拟评分; ODI: Oswestry功能障碍指数.
下载: 导出CSV
表 4 两组患者术后影像学评价结果的比较
Table 4. Comparison of postoperative imaging evaluation results between two groups of patients (n=25)
指标 观察组 对照组 χ2/t P Cobb角变化(°, Mean±SD) 术后3月 1.25±1.78 1.12±1.32 0.29 0.77 术后12月 1.35±2.01 1.28±1.34 0.14 0.88 术后12月融合率(%) 88 76 1.22 0.27
下载: 导出CSV
-
[1] 姜乐涛, 杜建伟. 腰椎管狭窄症的治疗进展[J]. 局解手术学杂志, 2021, 30(11): 1012-7. https://www.cnki.com.cn/Article/CJFDTOTAL-JJXZ202111020.htm [2] 刘华, 陆圣君, 龚腊梅, 等. 经皮全脊柱内镜与显微镜辅助下经椎板间隙入路手术对老年腰椎管狭窄症的疗效及安全性分析[J]. 局解手术学杂志, 2021, 30(11): 970-4. https://www.cnki.com.cn/Article/CJFDTOTAL-JJXZ202111010.htm [3] 刘俭涛, 李新友, 张小卫, 等. 局麻或全麻下脊柱内镜经椎板间入路治疗腰椎间盘突出症的效果对比[J]. 西安交通大学学报: 医学版, 2022, 43(1): 83-7. https://www.cnki.com.cn/Article/CJFDTOTAL-XAYX202201015.htm [4] 张跃, 朱宇, 李毅, 等. 单侧双通道脊柱内镜技术治疗腰椎间盘突出症68例临床研究[J]. 中华实验外科杂志, 2021, 38(11): 2262-5. doi: 10.3760/cma.j.cn421213-20210313-01092 [5] 康立星, 杨素梅, 张鹏, 等. 单通道、单侧双通道和双侧三通道脊柱内镜技术对腰椎管狭窄症的临床疗效比较[J]. 川北医学院学报, 2021, 36(10): 1323-8. doi: 10.3969/j.issn.1005-3697.2021.10.014 [6] 汪文龙, 刘正, 吴四军, 等. 单侧双通道内镜下减压治疗腰椎管狭窄症的早期疗效观察[J]. 中国脊柱脊髓杂志, 2021, 31(10): 911-8. doi: 10.3969/j.issn.1004-406X.2021.10.06 [7] 苏保辉, 栾素娴, 孙良智, 等. 单侧双通道内镜治疗双节段腰椎管狭窄症[J]. 中国矫形外科杂志, 2022, 30(16): 1508-11. https://www.cnki.com.cn/Article/CJFDTOTAL-ZJXS202216014.htm [8] 郑晓青, 昌耘冰, 李梦远, 等. Coflex棘突间固定装置在治疗腰椎管狭窄症中的价值[J]. 中国临床解剖学杂志, 2015, 33(3): 344-8, 353. doi: 10.13418/j.issn.1001-165x.2015.03.024 [9] 郑晓青, 顾宏林, 郑超, 等. Wallis棘突间动态稳定系统治疗腰椎管狭窄症的临床疗效观察[J]. 中国临床解剖学杂志, 2014, 32(2): 221-4. https://www.cnki.com.cn/Article/CJFDTOTAL-ZLJZ201402029.htm [10] 康健, 王世轩. 中医外治法治疗腰椎管狭窄症的研究进展[J]. 实用中医内科杂志, 2022, 36(1): 97-9. https://www.cnki.com.cn/Article/CJFDTOTAL-SYZY202201031.htm [11] 黄卫国, 侯东坡, 王建光, 等. 微创椎间孔镜减压和传统开放手术治疗单节段退行性腰椎管狭窄症的临床疗效对比研究[J]. 实用骨科杂志, 2021, 27(7): 632-7. https://www.cnki.com.cn/Article/CJFDTOTAL-SGKZ202107014.htm [12] 叶丙霖, 王想福, 李淑玲, 等. 大通道内镜经单侧入路双侧减压治疗老年腰椎管狭窄症[J]. 中国骨伤, 2021, 34(1): 8-14. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGGU202101003.htm [13] 赵子豪, 李雪城, 李建军, 等. 单侧双通道内镜与经通道显微镜减压技术治疗腰椎管狭窄症疗效比较[J]. 滨州医学院学报, 2021, 44(5): 341-5. https://www.cnki.com.cn/Article/CJFDTOTAL-BZYB202105005.htm [14] 蒋强, 丁宇. 经皮内镜减压术治疗腰椎管狭窄症临床应用进展[J]. 颈腰痛杂志, 2020, 41(5): 628-30, 640. https://www.cnki.com.cn/Article/CJFDTOTAL-JYTZ202005033.htm [15] Ikuta K, Sakamoto K, Hotta K, et al. Predictors for clinical outcomes of tubular surgery for endoscopic decompression in selected patients with lumbar spinal stenosis[J]. Arch Orthop Trauma Surg, 2022, 142 (10): 2525-32. [16] Pranata R, Lim MA, Vania R, et al. Biportal endoscopic spinal surgery versus microscopic decompression for lumbar spinal Stenosis: a systematic review and Meta-analysis[J]. World Neurosurg, 2020, 138: e450-8. [17] 何贵生, 董宪杰. 经皮椎间孔脊柱内镜技术治疗退变性腰椎管狭窄症的效果分析[J]. 现代诊断与治疗, 2021, 32(19): 3102-3. https://www.cnki.com.cn/Article/CJFDTOTAL-XDZD202119059.htm [18] 谷艳超, 李莹, 谢维, 等. 单边双通道脊柱内镜技术治疗腰椎椎管狭窄症临床分析[J]. 国际骨科学杂志, 2021, 42(5): 323-8. https://www.cnki.com.cn/Article/CJFDTOTAL-GWGK202105014.htm [19] Kim JE, Choi DJ, Park EJJ, et al. Biportal endoscopic spinal surgery for lumbar spinal Stenosis[J]. Asian Spine J, 2019, 13(2): 334-42. [20] Phan K, Mobbs RJ. Minimally invasive versus open laminectomy for lumbar Stenosis: a systematic review and Meta-analysis[J]. Spine, 2016, 41(2): E91-E100. [21] Gadjradj PS, Rubinstein SM, Peul WC, et al. Full endoscopic versus open discectomy for sciatica: randomised controlled non-inferiority trial [J]. BMJ, 2022, 376: e065846. [22] Heo DH, Sharma S, Park CK. Endoscopic treatment of extraforaminal entrapment of L5 nerve root (far out syndrome) by unilateral biportal endoscopic approach: technical report and preliminary clinical results[J]. Neurospine, 2019, 16(1): 130-7. [23] Kim SK, Kang SS, Hong YH, et al. Clinical comparison of unilateral biportal endoscopic technique versus open microdiscectomy for single-level lumbar discectomy: a multicenter, retrospective analysis [J]. J Orthop Surg Res, 2018, 13(1): 22. [24] Heo DH, Lee DC, Park CK. Comparative analysis of three types of minimally invasive decompressive surgery for lumbar central stenosis: biportal endoscopy, uniportal endoscopy, and microsurgery [J]. Neurosurg Focus, 2019, 46(5): E9. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 143
- HTML全文浏览量: 80
- PDF下载量: 2
- 被引次数: 0