



Curative effect and prognostic factors of patients with chronic subdural hematoma treated by intracranial minimally invasive evacuation guided by CT density of lesions
-
摘要:
目的 观察病灶CT密度值指导下颅内微创血肿清除术治疗慢性硬膜下血肿(CSDH)患者疗效及预后影响因素。 方法 回顾性分析2017年12月~2020年12月于我院接受治疗的134例CSDH患者的临床资料,根据手术方法分为观察组(n=74,行病灶CT密度值指导下颅内微创血肿清除术)与对照组(n=60,行常规颅骨钻孔闭式引流术)。比较两组围术期指标,并记录手术前后神经及运动功能[中国卒中量表(CSS)、改良Barthel指数(MBI)]及并发症发生。以出院后3月的Markwalder's分级作为预后情况的评估标准,将观察组分为预后不良组及预后良好组,通过单因素及多因素Logistic回归方程分析影响病灶CT密度值指导下颅内微创血肿清除术治疗CSDH预后的危险因素。 结果 两组患者术中出血、术后拔管时间、住院时间差异无统计学意义(P>0.05),观察组手术时间更长(P<0.05),术后30 d血肿清除率更高(P<0.05);CT图像显示,治疗前左侧额颞顶枕部低信号新月形影像,局部占位效应明显,脑组织受压,中线结构移位,治疗后慢性硬膜下血肿钻孔引流术后第1天,引流管留置,硬膜下积液积气表现,局部占位效应减轻,中线结构移位好转;两组患者术前CSS、MBI评分差异无统计学意义(P>0.05),两组术后30 d的CSS评分较术前降低,MBI评分较术前升高(P<0.05),且观察组术后CSS评分更低,MBI评分更高(P<0.05);两组随访3月内均无死亡病例,各项并发症发生率差异无统计学意义(P>0.05);年龄、脑萎缩及入院时格拉斯哥昏迷评分在预后良好组及预后不良组组间差异有统计学意义(P<0.05),性别、出现症状到入院时间、血肿量、饮酒史、抽烟史、血肿CT值、术后引流、抗凝药物在预后良好组及预后不良组组间差异无统计学意义(P>0.05);年龄>65岁及入院时格拉斯哥昏迷评分<13分为影响病灶CT密度值指导下颅内微创血肿清除术治疗CSDH预后的独立危险因素(P<0.05)。 结论 病灶CT密度值指导下颅内微创血肿清除术治疗CSDH效果理想,血肿清除率高,其预后与年龄及入院时格拉斯哥昏迷评分有关。 Abstract:Objective To observe the curative effect and prognostic factors of patients with chronic subdural hematoma (CSDH) treated by intracranial minimally invasive evacuation under the guidance of CT density. Methods The clinical data of 134 CSDH patients treated in our hospital from December 2017 to December 2020 were analyzed retrospectively. According to the surgical methods, they were divided into observation group (n=74, minimally invasive evacuation of intracranial hematoma guided by CT density of lesions) and control group (n=60, conventional skull drilling and closed drainage). The perioperative indexes of the two groups were compared, and the neurological and motor functions [Chinese stroke scale (CSS), modified Barthel index (MBI)] and complications were recorded before and after operation. Markwalder's grade at 3 months after discharge was taken as the evaluation standard of prognosis, and the observation group was divided into poor prognosis group and good prognosis group. The risk factors affecting the prognosis of CSDH were analyzed by univariate and multivariate Logistic regression equation. Results There were no statistically significant differences in intraoperative bleeding, postoperative extubation time and hospital stay between the two groups (P>0.05). The operation time of the observation group was significantly longer (P<0.05), and the hematoma clearance rate was significantly higher 30 days after surgery (P<0.05). CT images show that before the treatment to the top of the left frontal temporal occipital low signal crescent images, local placeholder effect obvious, compression of brain tissue, midline structure shift, after treatment of chronic subdural hematoma on the first day after drilling drainage, drainage tube indwelling, subdural effusion pneumatosis performance, reduce local placeholder effect, midline structure shift better; There was no statistical significance in preoperative CSS and MBI scores between the two groups (P>0.05). The CSS score of the two groups at 30 days after surgery was significantly lower than that before surgery, while the MBI score was significantly higher than that before surgery(P<0.05). The CSS score of the observation group was lower and THE MBI score was higher after surgery(P<0.05). There was no death in the two groups within 3 months of follow-up, and there was no statistical significance in the incidence of complications (P>0.05). Age, brain atrophy and on admission GCS score in a set of good prognosis and bad prognosis way between the difference was statistically significant (P<0.05). Gender, symptoms to hospital time, hematoma volume, history of drinking, smoking history, hematoma, postoperative drainage, CT value of anticoagulant drugs in good prognosis group were not significantly different from the bad way prognosis (P>0.05). Age>65 years old and GCS score<13 at admission were independent risk factors of prognosis of CSDH after minimally invasive intracranial hematoma removal guided by CT density value (P<0.05). Conclusion Minimally invasive evacuation of intracranial hematoma guided by CT density of lesions is effective in the treatment of CSDH, and its prognosis is related to age and GCS score at admission. -

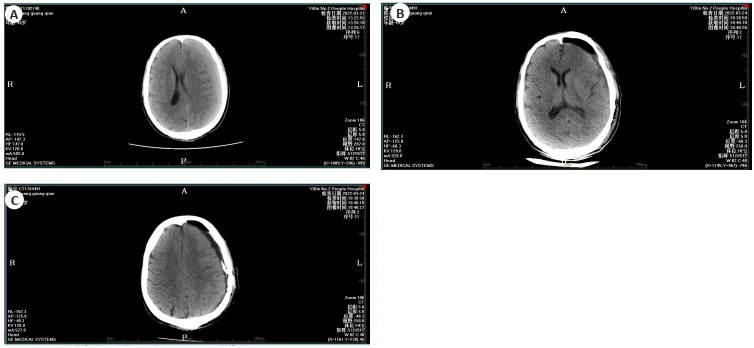
图 1 患者女性,83岁,左侧额颞顶枕部慢性硬膜下血肿
A: 左侧额颞顶枕部低信号新月形影像, 局部占位效应明显, 脑组织受压,中线结构移位; B: 慢性硬膜下血肿钻孔引流术后第1天, 引流管留置, 硬膜下积液积气表现, 局部占位效应减轻, 中线结构移位好转.
Figure 1. An 83-year-old female patient presented with a chronic subdural hematoma in the left frontotemporal parietal occipital region.

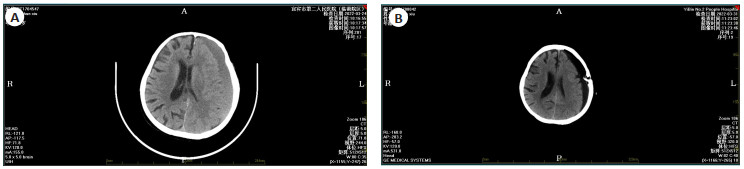
图 2 患者男性,49岁,左侧额颞顶枕部慢性硬膜下血肿
A: 左侧额颞顶枕部稍高信号新月形影像, 局部占位效应明显, 脑组织受压, 中线结构移位; B~C: 慢性硬膜下血肿钻孔引流术后第1天, 引流管留置, 硬膜下积液积气表现, 局部占位效应减轻, 中线结构移位好转.
Figure 2. A 49-year-old male patient presented with a chronic subdural hematoma in the left frontotemporal parietal occipital region.
表 1 两组患者围手术期指标比较
Table 1. Comparison of perioperative indicators between the two groups (Mean±SD)
组别 手术时间(min) 术中出血(mL) 术后拔管时间(d) 住院时间(d) 术后30 d血肿清除率(%) 观察组(n=74) 71.25±8.46 27.15±4.12 4.12±1.29 10.41±2.15 96.14±2.12 对照组(n=60) 56.21±7.45 26.58±4.51 4.41±0.96 10.58±2.46 84.25±4.23 t 10.789 0.763 1.446 0.427 21.139 P < 0.001 0.447 0.15 0.67 < 0.001  下载: 导出CSV
下载: 导出CSV
表 2 两组患者CSS、MBI评分比较
Table 2. Comparison of CSS and MBI scores between the two groups (points, Mean±SD)
组别 CSS MBI 术前 术后30 d 术前 术后30 d 观察组(n=74) 32.15±4.78 12.02±2.14* 60.48±7.45 72.15±6.45* 对照组(n=60) 31.51±5.23 24.15±4.57* 59.86±6.48 66.25±5.87* t 0.739 20.268 0.507 5.48 P 0.461 < 0.001 0.613 < 0.001 *P<0.05 vs同组术前. CSS: 中国卒中量表; MBI: 改良Barthel指数评定量表
下载: 导出CSV
表 3 两组随访期间并发症发生比较
Table 3. Comparison of complications between the two groups during follow-up [n(%)]
组别 复发 颅内积气 颅内感染 硬膜外血肿 脑脊液漏液 观察组(n=74) 3(4.05) 2(2.70) 0(0.00) 0(0.00) 1(1.35) 对照组(n=60) 6(10.00) 3(5.00) 2(3.33) 1(1.67) 2(3.33) χ2/Fisher 1.041 0.057 0.75 - 0.034 P 0.308 0.811 0.386 1 0.854
下载: 导出CSV
表 4 影响病灶CT密度值指导下颅内微创血肿清除术治疗CSDH预后的单因素分析
Table 4. Effect under the guidance of intracranial lesions on CT density values for the treatment of minimally invasive hematoma removal of CSDH prognosis of single factor analysis
因素 预后良好组(n=51) 预后不良组(n=23) χ2 P 例数(n) 构成比(%) 例数(n) 构成比(%) 年龄(岁) 8.745 0.003 ≤60 30 58.82 5 21.74 > 60 21 41.18 18 78.26 性别 0.459 0.498 男 29 56.86 15 65.22 女 22 43.14 8 34.78 出现症状到入院时间(d) 0.426 0.514 ≤7 16 31.37 9 39.13 > 7 35 68.63 14 60.87 血肿量(mL) 1.503 0.220 ≤80 30 58.82 10 43.48 > 80 21 41.18 13 56.52 饮酒史 1.416 0.234 有 34 66.67 12 52.17 无 17 33.33 11 47.83 抽烟史 0.001 0.978 有 29 56.86 13 56.52 无 22 43.14 10 43.48 脑萎缩 5.542 0.019 有 9 17.65 10 43.48 无 42 82.35 13 56.52 血肿CT值(Hu) 0.408 0.523 ≤45 37 72.55 15 65.22 > 45 14 27.45 8 34.78 GCS 10.945 0.001 <13 40 78.43 9 39.13 ≥13 11 21.57 14 60.87 术后引流 1.983 0.159 单侧 41 80.39 15 65.22 双侧 10 19.61 8.00 34.78 抗凝药物 1.009 0.315 有 14 27.45 9 39.13 无 37 72.55 14 60.87 GCS: 格拉斯哥昏迷评分.
下载: 导出CSV
表 5 影响病灶CT密度值指导下颅内微创血肿清除术治疗CSDH预后的多因素分析
Table 5. Effect under the guidance of intracranial lesions on CT density values for the treatment of minimally invasive hematoma removal of CSDH multi-factor analysis of prognosis
因素 β SE Wald χ2 OR 95% CI P 年龄(≤65岁vs>65岁) 1.235 0.341 13.117 3.438 1.762~6.708 < 0.001 入院时GCS评分(≥13分vs<13分) 0.987 0.241 16.773 2.683 1.673~4.303 < 0.001 赋值说明: 应变量y(0=>65岁, 1=≤65岁)、高血压病史(0=<13分, 1=≥13分)
下载: 导出CSV
-
[1] 谭钧城, 石柳, 张永建. 症状性慢性硬膜下血肿钻孔术后膜下引流与骨膜下引流疗效分析[J]. 实用医院临床杂志, 2019, 16(5): 269-72. doi: 10.3969/j.issn.1672-6170.2019.05.084 [2] Shen J, Yuan LL, Ge RX, et al. Clinical and radiological factors predicting recurrence of chronic subdural hematoma: a retrospective cohort study[J]. Injury, 2019, 50(10): 1634-40. doi: 10.1016/j.injury.2019.08.019 [3] Shen J, Gao YL, Li QF, et al. Risk factors predicting recurrence of bilateral chronic subdural hematomas after initial bilateral evacuation[J]. World Neurosurg, 2019, 130: e133-9. doi: 10.1016/j.wneu.2019.06.016 [4] Yamada SM, Tomita Y, Murakami H, et al. Headache in patients with chronic subdural hematoma: analysis in 1080 patients[J]. Neurosurg Rev, 2018, 41(2): 549-56. doi: 10.1007/s10143-017-0889-x [5] 陈锐锋, 朱安林. 微创钻孔引流术联合阿托伐他汀对慢性硬膜下血肿患者术后并发症及复发率的影响[J]. 安徽医学, 2019, 40(1): 62-5. doi: 10.3969/j.issn.1000-0399.2019.01.019 [6] 鲁友明, 邓志锋, 张爱军, 等. 慢性硬膜下血肿术后并发脑耗盐综合征的临床疗效(附114例病例报告)[J]. 立体定向和功能性神经外科杂志, 2019, 32(1): 42-6. https://www.cnki.com.cn/Article/CJFDTOTAL-NENG201901010.htm [7] Baschera D, Tosic L, Westermann L, et al. Treatment standards for chronic subdural hematoma: results from a survey in Austrian, German, and Swiss neurosurgical units[J]. World Neurosurg, 2018, 116: e983-95. doi: 10.1016/j.wneu.2018.05.145 [8] 方江顺, 王贤书, 杨志国, 等. 颅骨钻孔引流联合尿激酶溶栓治疗小儿创伤性硬膜外血肿的效果观察[J]. 实用心脑肺血管病杂志, 2018, 26(12): 87-90. https://www.cnki.com.cn/Article/CJFDTOTAL-SYXL201812026.htm [9] 张向前, 佟建洲, 李树文, 等. 钻孔引流术后联合脑血疏口服液治疗慢性硬膜下血肿的效观察[J]. 中西医结合心脑血管病杂志, 2019, 17(15): 2379-81. doi: 10.12102/j.issn.1672-1349.2019.15.037 [10] 徐兵, 黄录茂, 雍成明, 等. 根据病灶CT密度值选择术式治疗慢性硬膜下血肿51例[J]. 山东医药, 2018, 58(11): 69-71. https://www.cnki.com.cn/Article/CJFDTOTAL-SDYY201811021.htm [11] Frechon P, Emery E, Gaberel T. Is there an interest in performing a systematic CT scan within the first two months after chronic subdural hematoma evacuation? A ten-year single-center retrospective study[J]. Clin Neurol Neurosurg, 2020, 191: 105682. doi: 10.1016/j.clineuro.2020.105682 [12] 蔡浩荻, 吕秋石, 朱武生, 等. 用于识别大血管闭塞型卒中的院前卒中量表[J]. 国际脑血管病杂志, 2019, 27(5): 363-8. doi: 10.3760/cma.j.issn.1673-4165.2019.05.008 [13] 周海燕, 陈多妹, 王陈军. 改良Barthel指数评定量表在脑卒中患者中的应用及影响效果分析[J]. 中国药物与临床, 2018, 18(12): 2259-61. https://www.cnki.com.cn/Article/CJFDTOTAL-YWLC201812102.htm [14] 曹德茂, 彭爱军, 武永康, 等. 微创穿刺联合术中尿激酶腔内注射治疗慢性硬膜下血肿的临床研究[J]. 中国医师杂志, 2019, 21(3): 428-31. [15] 刘国栋, 王守利, 李会华, 等. 三种手术方法治疗慢性硬膜下血肿的临床分析[J]. 中华神经外科疾病研究杂志, 2017, 16(1): 58-60. https://www.cnki.com.cn/Article/CJFDTOTAL-SJWK201701015.htm [16] Kutty RK, Leela SK, Sreemathyamma SB, et al. The outcome of medical management of chronic subdural hematoma with tranexamic acid-A prospective observational study[J]. J Stroke Cerebrovasc Dis, 2020, 29(11): 105273. [17] Tran DK, Tretiakov P, Brock J, et al. Novel use of dual-lumen catheter for irrigation and drainage after evacuation of chronic subdural hematoma[J]. World Neurosurg, 2019, 132: 343-6. [18] Feghali J, Yang W, Huang J. Updates in chronic subdural hematoma: epidemiology, etiology, pathogenesis, treatment and outcome[J]. World neurosurg, 2020, 141: 339-45. [19] Holl DC, Volovici V, Dirven CMF, et al. Pathophysiology and nonsurgical treatment of chronic subdural hematoma: from past to present to future[J]. World Neurosurg, 2018, 116: 402-11. e2. [20] 石晓勇, 汤朱骁, 孙虎, 等. 高龄患者慢性硬膜下血肿复发的危险因素及再次手术策略[J]. 中华老年医学杂志, 2020, 39(2): 201-3. https://cpfd.cnki.com.cn/Article/CPFDTOTAL-ZJKX202011004065.htm [21] 张诚, 茅明凯, 张保剑, 等. 基于病灶CT密度值选择颅内微创血肿清除术治疗慢性硬膜下血肿的疗效研究[J]. 神经损伤与功能重建, 2020, 15(5): 290-2. https://www.cnki.com.cn/Article/CJFDTOTAL-GWKF202005013.htm [22] Mehta V, Harward SC, Sankey EW, et al. Evidence based diagnosis and management of chronic subdural hematoma: a review of the literature[J]. J Clin Neurosci, 2018, 50: 7-15. . [23] 张笑, 吴昊, 马百涛, 等. 慢性硬膜下血肿患者院内死亡的危险因素分析[J]. 卒中与神经疾病, 2019, 26(5): 624-5, 629. https://www.cnki.com.cn/Article/CJFDTOTAL-ZZYS201905029.htm [24] Kitya D, Punchak M, Abdelgadir J, et al. Causes, clinical presentation, management, and outcomes of chronic subdural hematoma at Mbarara Regional Referral Hospital[J]. Neurosurg Focus, 2018, 45(4): E7. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 139
- HTML全文浏览量: 68
- PDF下载量: 3
- 被引次数: 0