



Value of 3D-ASL combined with DWI and MRA in assessment of ischemic penumbra in acute ischemic cerebral infarction
-
摘要:
目的 探究三维动脉自旋标记灌注成像(3D-ASL)联合弥散加权成像(DWI)、血管成像(MRA)对急性缺血性脑梗死缺血半暗带区域(IP)的评估价值。 方法 选取2021年1月~2022年6月本院收治的急性缺血性脑梗死患者62例,所有患者均接受3D-ASL、DWI、MRA扫描,根据病灶最大层面DWI高信号面积、ASL异常灌注面积评估患者是否存在IP,根据患者发病至首次MRI检查时间(T)将患者分为超急性期(T<6 h)和急性期(6 h≤T≤24 h)。记录患者中心梗死区、IP区与IP对侧镜像区的表观扩散系数(ADC)、脑血流量(CBF)值,根据MRA图像对血管狭窄程度进行分级。 结果 急性缺血性脑梗死患者病灶DWI表现为斑点状或小片状高信号,48例患者3D-ASL异常灌注面积明显大于DWI异常高信号面积,显示存在IP区;MRA显示颅内某支主干动脉节段性狭窄,远端血管明显变细甚至消失,部分显示血管无明显异常。患者不同区域CBF、ADC值比较:中心梗死区<IP区<对侧镜像区(P<0.05);超急性期患者rCBF值、rADC值均大于急性期患者,差异有统计学意义(P<0.05)。存在IP区的患者MRA血管狭窄程度以0级为主,非IP区患者MRA血管狭窄程度以3级为主;两组患者的MRA血管狭窄程度比较,差异有统计学意义(P<0.05)。 结论 3D-ASL联合DWI、MRA检测可准确评估急性缺血性脑梗死患者IP区的存在和血管狭窄程度,有利于梗死临床精准化治疗方案的选择。 -
关键词:
- 急性缺血性脑梗死 /
- 缺血半暗带区 /
- 三维动脉自旋标记灌注成像 /
- 弥散加权成像 /
- 血管成像
Abstract:Objective To investigate the value of three-dimensional arterial spin labeling (3D-ASL) combined with diffusionweighted imaging (DWI) and magnetic resonance angiography (MRA) in assessment of ischemic penumbra (IP) in acute ischemic cerebral infarction. Methods A total of 62 patients with acute ischemic cerebral infarction were treated in the hospital from January 2021 to June 2022. All patients underwent 3D- ASL, DWI and MRA. The presence or absence of IP was determined according to the area of DWI hyperintensity at the maximum slice of the lesion and the abnormal perfusion area of ASL. According to the time from onset to first MRI, the patients were divided into the hyperacute phase (T<6 h) group and the acute phase (6 h≤T≤24 h) group. The apparent diffusion coefficient (ADC) values and cerebral blood flow (CBF) of central infarct area, IP area and contralateral area of IP were recorded. The degree of vascular stenosis was graded according to MRA images. Results The lesions of patients with acute ischemic cerebral infarction showed spotted or small pieces of high signals on DWI. 48 patients had significantly larger abnormal perfusion area on 3D-ASL than abnormal high signal area on DWI, which indicated the existence of IP area. MRA showed segmental stenosis of a intracranial main branch, significantly thinned or even disappeared distal blood vessels, and some blood vessels without obvious abnormalities. The CBF and ADC values of central infarct area, IP area, and contralateral area of IP increased in order (P<0.05). The rCBF and rADC values in hyperacute phase were higher than those in acute phase (P<0.05). MRA showed that vascular stenosis mainly was grade 0 in patients with IP, and mainly was grade 3 in patients without IP (P<0.05). Conclusion 3D-ASL combined with DWI and MRA can help to accurately assess the presence or absence of IP area and the degree of vascular stenosis in patients with acute ischemic cerebral infarction, which is beneficial to the selection of clinical treatment plan. -

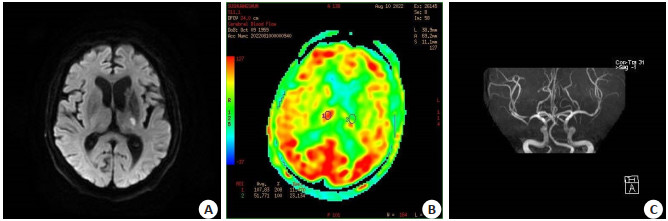
图 1 患者女,67岁,左侧内囊后肢新发梗塞
A: 左侧内囊后肢DWI呈高信号; B: ASL较对侧呈低灌注; C: MRA示左侧血管未见明显狭窄.
Figure 1. Images of a 67-year-old female patient with new posterior internal capsule infarction.

图 2 患者男,65岁,左侧尾状核头新发脑梗塞
A: 左侧尾状核头DWI高信号; B: ASL较对侧呈低灌注; C: MRA示左侧血管未见明显狭窄.
Figure 2. Images of a 65-year-old male patient with new infarction in the head of the left caudate nucleus.
表 1 急性缺血性脑梗死患者中心梗死区、IP区和对侧镜像区CBF、ADC值比较
Table 1. Comparison of CBF and ADC values of central infarcted area, IP area and contralateral area in patients with acute ischemic cerebral infarction (Mean±SD)
区域 CBF[mL/(100 g·min)] ADC(×10-3 mm2/s) 中心梗死区 20.39±3.67ab 0.32±0.10ab IP区 36.54±5.12b 0.61±0.09b 对侧镜像区 54.89±5.67 0.76±0.12 F 771.54 286.35 P < 0.001 < 0.001 aP<0.05 vs IP区; bP<0.05 vs对侧镜像区.  下载: 导出CSV
下载: 导出CSV
表 2 不同时期急性缺血性脑梗死患者rCBF、rADC值比较
Table 2. Comparison of rCBF and rADC values between patients with acute ischemic cerebral infarction in different phases (Mean±SD)
时期 rCBF[mL/(100 g·min)] rADC(×10-3 mm2/s) 急性期(n=40) 0.64±0.07 0.81±0.05 超急性期(n=22) 0.76±0.08 0.92±0.03 t 11.481 18.906 P < 0.001 < 0.001
下载: 导出CSV
表 3 急性缺血性脑梗死患者MRA血管狭窄程度与IP区的关系分析
Table 3. Relationship between vascular stenosis degree displayed by MRA and IP in patients with acute ischemic cerebral infarction [n(%)]
组别 MRA血管狭窄程度 0级 1级 2级 3级 4级 IP区(n=48) 26(54.17) 16(33.33) 5(10.42) 1(2.08) 0(0.00) 非IP区(n=14) 2(14.29) 4(28.57) 1(7.14) 7(50.00) 0(0.00) *P<0.001.行Fisher确切概率检验.
下载: 导出CSV
-
[1] Sun Z, Xu Q, Gao G, et al. Clinical observation in edaravone treatment for acute cerebral infarction[J]. Niger J Clin Pract, 2019, 22(10): 1324-7. doi: 10.4103/njcp.njcp_367_18 [2] 刘姝兰, 宋震宇, 余飞, 等. CT灌注成像与MR灌注成像诊断急性缺血性脑卒中的对比研究[J]. 医学影像学杂志, 2020, 30(8): 1345-8. https://www.cnki.com.cn/Article/CJFDTOTAL-XYXZ202008004.htm [3] 曾进胜, 于生元, 谢鹏. 重视急性脑梗死后缺血半暗带的临床评估和治疗[J]. 中国神经精神疾病杂志, 2021, 47(6): 321-3. doi: 10.3969/j.issn.1002-0152.2021.06.001 [4] 王盛磊, 朱幼玲, 唐敏. MR灌注加权成像在急性脑梗死患者临床诊治中的应用研究[J]. 中国脑血管病杂志, 2019, 16(5): 274-7. doi: 10.3969/j.issn.1672-5921.2019.05.011 [5] Pang HP, Dang XF, Ren Y, et al. 3D-ASL perfusion correlates with VEGF expression and overall survival in glioma patients: comparison of quantitative perfusion and pathology on accurate spatial location-matched basis[J]. J Magn Reson Imaging, 2019, 50(1): 209-20. doi: 10.1002/jmri.26562 [6] 黄立敏, 雷竹, 张瑜, 等. 磁共振3D-ASL技术在高级别胶质瘤靶区勾画术后残留病灶识别中的应用[J]. 中国癌症杂志, 2019, 29(11): 875-9. doi: 10.19401/j.cnki.1007-3639.2019.11.006 [7] 中华医学会神经病学分会, 中华医学会神经病学分会脑血管病学组. 中国急性缺血性脑卒中诊治指南2014[J]. 中华神经科杂志, 2015, 48(4): 246-57. doi: 10.3760/cma.j.issn.1006-7876.2015.04.002 [8] Liu YF, Li YF, Zang JK, et al. CircOGDH is a penumbra biomarker and therapeutic target in acute ischemic stroke[J]. Circ Res, 2022, 130(6): 907-24. doi: 10.1161/CIRCRESAHA.121.319412 [9] 钱小建, 严循成, 肖志锋. 动脉自旋标记成像与灌注加权成像在老年缺血性脑梗死诊断中应用价值[J]. 创伤与急危重病医学, 2018, 6(5): 300-1, 303. doi: 10.16048/j.issn.2095-5561.2018.05.16 [10] 冯中全, 钱伟军, 李杰, 等. DSC-PWI联合MRA在脑梗死慢性期预后评估中的应用价值[J]. 临床放射学杂志, 2019, 38(7): 1180-5. doi: 10.13437/j.cnki.jcr.2019.07.002 [11] Zhou JG, Fu DY, Meng Y, et al. Application of three- dimensional arterial spin labeling technique in the assessment of cerebral blood perfusion in patients with middle cerebral artery occlusion: analysis of clinical implications and prognostic factors[J]. Dis Markers, 2022, 2022: 6990590. [12] 康钰, 史浩, 刘华秀, 等. 3D-pCASL及磁敏感加权成像联合应用在预测脑缺血灶转归的应用价值[J]. 实用放射学杂志, 2019, 35(5): 708-12. doi: 10.3969/j.issn.1002-1671.2019.05.006 [13] 蔡振宇, 肖俊强, 利进琴, 等. 3D-ASL灌注联合MRA、DWI加权成像评价急性脑梗死缺血半暗带的临床价值研究[J]. 影像研究与医学应用, 2022, 6(4): 145-7. doi: 10.3969/j.issn.2096-3807.2022.04.049 [14] Brugnara G, Herweh C, Neuberger U, et al. Dynamics of cerebral perfusion and oxygenation parameters following endovascular treatment of acute ischemic stroke[J]. J Neurointerv Surg, 2022, 14(1): neurintsurg-2020-017163. [15] 蒋玉涵, 刘杨颖秋, 高冰冰, 等. 基于酰胺质子转移加权成像评估亚急性脑梗死患者梗死核心及半暗带的酸碱代谢变化[J]. 中华放射学杂志, 2021, 55(5): 500-6. doi: 10.3760/cma.j.cn112149-20200513-00682 [16] 邰兆琴, 黄清玲, 朱万荣, 等. 三维ASL联合DWI评估急性脑梗死患者缺血性半暗带及预后[J]. 中国医学影像技术, 2020, 36(9): 1292-6. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYXX202009004.htm [17] 张迷, 杨燕, 郑卫华. DTI联合DWI在诊断早期脑梗死缺血半暗带中的应用[J]. 中国CT和MRI杂志, 2019, 17(8): 15-7. doi: 10.3969/j.issn.1672-5131.2019.08.005 [18] 许超, 冯天保. 不同时期脑梗死DWI、PWI成像特征及其缺血半暗带的鉴别诊断价值研究[J]. 中国CT和MRI杂志, 2021, 19(8): 11-4. doi: 10.3969/j.issn.1672-5131.2021.08.004 [19] Cui B, Yang DD, Zheng WM, et al. Plaque enhancement in multicerebrovascular beds associates with acute cerebral infarction[J]. Acta Radiol, 2021, 62(1): 102-12. doi: 10.1177/0284185120915604 [20] 张博伦, 梁晓芸, 韩璐, 等. 三维动脉自旋标记联合扩散加权成像、磁共振血管成像在急性腔隙性脑梗死中的应用价值[J]. 实用放射学杂志, 2020, 36(12): 1898-901. doi: 10.3969/j.issn.1002-1671.2020.12.003 -


 点击查看大图
点击查看大图
计量
- 文章访问数: 157
- HTML全文浏览量: 98
- PDF下载量: 16
- 被引次数: 0