



Effect of scalp acupuncture combined with butylphthalide on the stenosis and hypoperfusion area of middle cerebral artery and cognitive function
-
摘要:
目的 探讨头穴透刺联合丁苯酞对严重大脑中动脉狭窄低灌注区脑灌注及认知功能的影响。 方法 选取2019年3月~2020年12月我院神经内科门诊收治的符合入选标准的单侧大脑中动脉狭窄患者96例为研究对象,根据随机数字表法将其分为研究组及对照组,48例/组。两组均给予基础药物治疗:阿托伐他汀+氯吡格雷,每种口服1片/d,连服4周;研究组增加头穴透刺联合丁苯酞软胶囊。两组患者治疗前后行CT灌注成像,观测患区及对称非患病区脑血容量(CBV)、脑血流量(CBF)、平均通过时间(MTT)和达峰时间(TTP),计算患区灌注参数与对称非患区灌注参数比值,即rCBV、rCBF、rMTT、rTTP;采集两组患者治疗前后空腹静脉血检测血清一氧化氮、内皮素-1、血栓素B2、血管紧张素Ⅱ、血管内皮生长因子、脑源性神经营养因子、神经元特异性烯醇化酶、s100β蛋白水平,并行简易精神状态评价量表评价患者认知能力。 结果 治疗后,研究组的CBV、CBF高于治疗前及治疗后对照组(P<0.05),MTT、TTP、rCBV、rCBF、rMTT、rTTP均低于治疗前及治疗后对照组(P<0.05);治疗后两组血清一氧化氮、内皮素-1、血管内皮生长因子、脑源性神经营养因子、神经元特异性烯醇化酶、s100β蛋白水平均高于治疗前,且研究组高于对照组(P<0.05);两组治疗后血栓素B2、血管紧张素Ⅱ均低于治疗前,且研究组低于对照组(P<0.05);治疗后两组认知功能各指标均显著高于治疗前,且研究组高于对照组(P<0.05)。 结论 头穴透刺联合丁苯酞可有效改善严重大脑中动脉狭窄患者远端侧支循环开放,提高脑血流量,上调神经营养因子,促进认知功能恢复。 Abstract:Objective To explore the effect of scalp acupuncture combined with butylphthalide on cerebral perfusion and cognitive function in severe middle cerebral artery stenosis hypoperfusion area. Methods A total of 96 patients with unilateral middle cerebral artery stenosis who were admitted to the department of Neurology outpatient department of our hospital from March 2019 to December 2020 were selected as the subjects. They were randomly divided into study group and control group according to random number table method, with 48 patients in each group. Both groups were given basic drug therapy: atorvastatin + clopidogrel, 1 tablet per day orally for 4 weeks. In the study group, the combination of head point penetration and butylphthalide soft capsule was added. CT perfusion imaging (CTP) was performed before and after treatment in 2 groups. Cerebral blood volume (CBV), cerebral blood flow (CBF), mean time to pass (MTT) and peak time (TTP) in affected area and symmetric non- affected area were observed. The ratio of affected area perfusion parameters to symmetric nonaffected area perfusion parameters, namely rCBV, rCBF, rMTT and rTTP were calculated. Serum nitric oxide, endothelin-1, thromboxane B2 and AngII were detected in fasting venous blood of two groups before and after treatment, vascular endothelial growth factor, brain-derived neurotrophic factor, neuron specific enolase, S100 β protein and the Simple Mental State Assessment Scale were used to evaluate the cognitive ability of the patients. Results After treatment, CBV and CBF in the study group were significantly higher than those before and after treatment (P<0.05). MTT, TTP, rCBV, rCBF, rMTT and rTTP were significantly lower than those in the control group (P<0.05). After treatment, the levels of nitric oxide, endothelin-1, vascular endothelial growth factor, brain- derived neurotrophic factor, neuron specific enolase and s100β in the two groups were significantly higher than before, and the study group was significantly higher than the control group. After treatment, thromboxane B2 and AngII in both groups were significantly lower than before, and the study group was significantly lower than the control group (P<0.05). After treatment, the indexes of cognitive function in the two groups were significantly higher than before, and the study group was higher than the control group (P<0.05). Conclusion Head point penetrating acupuncture combined with butylphthalide can effectively improve distal collateral circulation opening, increase cerebral blood flow, upregulate neurotrophic factors and promote cognitive function recovery in patients with severe middle cerebral artery stenosis. -

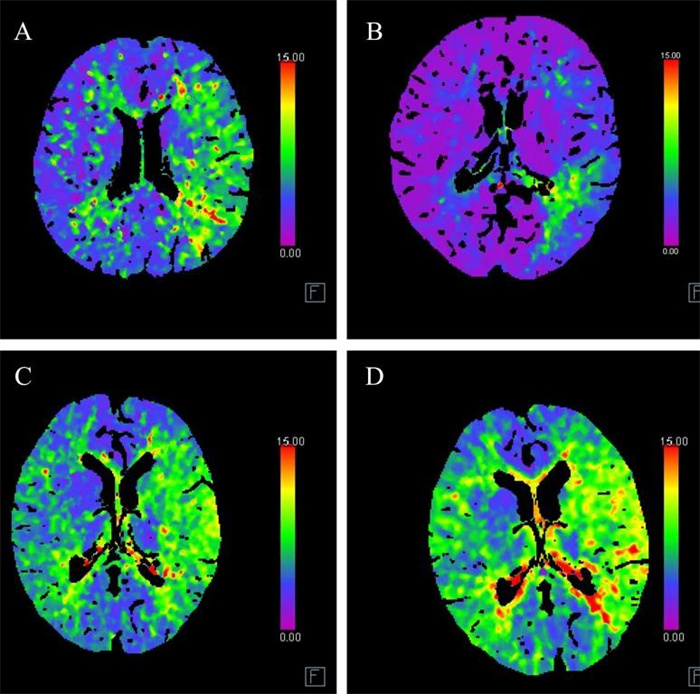
图 1 患者CTP图像
A~B: 研究组1例患者治疗前后CTP图像; C~D: 对照组1例患者治疗前后CTP图像.
Figure 1. CTP imagings of patients
表 1 两组患者一般资料比较
Table 1. Comparison of general data of the two groups of patients [n=48, n(%)]
指标 研究组 对照组 χ2/t P 性别(男/女, n) 25/23 27/21 0.17 0.68 年龄(岁, Mean±SD) 59.24±14.31 60.21±14.05 0.34 0.74 BMI(kg/m2, Mean±SD) 24.14±5.34 25.03±6.27 0.82 0.41 受教育程度 1.19 0.55 中学及以下 12 (25.00) 16(33.33) 高中/中专 15(31.25) 11(22.92) 大学/大专 13(27.08) 15(31.25) 研究生及以上 8(16.67) 6(12.50) 高同型半胱氨酸血症 37(77.08) 34(70.83) 0.49 0.49 吸烟史 28(58.33) 30(62.50) 1.07 0.30 糖尿病史 24(50.00) 30(62.50) 1.52 0.22 高血压史 34(70.83) 33(68.75) 0.05 0.82 高血脂史 36(75.00) 40(83.33) 1.01 0.32  下载: 导出CSV
下载: 导出CSV
表 2 两组患者CTP各参数比较
Table 2. Comparison of CTP parameters between the two groups (n=48, Mean±SD)
指标 治疗前 t P 治疗后 t P 研究组 对照组 研究组 对照组 CBV(mL/100g) 48.21±12.17 47.09±13.48 0.43 0.67 63.22±15.32* 53.04±14.08 3.81 < 0.01 CBF(mL/100g) 50.40±14.46 50.09±15.02 0.10 0.92 60.91±16.07* 51.42±18.97 4.91 0.01 MTT(s) 7.01±1.38 7.08±1.41 0.25 0.81 4.78±1.01* 6.06±1.37 2.74 0.01 TTP(s) 20.23±2.06 20.06±3.18 0.31 0.76 17.71±1.84* 19.26±2.12 8.28 < 0.01 rCBV 1.34±0.10 1.32±0.10 0.98 0.33 1.11±0.19* 1.30±0.32 7.70 < 0.01 rCBF 0.82±0.21 0.83±0.26 0.21 0.84 0.68±0.23* 0.88±0.21 5.64 < 0.01 rMTT 1.41±0.27 1.40±0.25 0.19 0.85 1.01±0.19* 1.31±0.24 15.21 < 0.01 rTTP 1.18±0.30 1.15±0.31 0.48 0.63 1.02±0.11* 1.07±0.23 8.60 < 0.01 *P<0.05 vs研究组治疗前. CBV: 脑血容量; CBF: 脑血流量; MTT: 平均通过时间; TTP: 达峰时间; rCBV、rCBF、rMTT、rTTP表示各患区灌注参数与对称非患区灌注参数比值.
下载: 导出CSV
表 3 两组患者血清指标比较
Table 3. Comparison of serum indicators between the two groups (n=48, Mean±SD)
指标 治疗前 t P 治疗后 t P 研究组 对照组 研究组 对照组 一氧化氮(μmol/L) 61.12±8.03 62.00±8.25 0.53 0.60 100.34±14.31* 87.23±19.07* 3.81 < 0.01 ET-1(μg/L) 81.07±13.23 81.70±14.40 0.22 0.82 55.02±11.21* 67.21±13.07* 4.91 0.01 TXB2(μg/L) 148.06±21.92 147.59±21.07 0.11 0.91 120.26±20.01* 132.04±22.04* 2.74 0.01 Ang II(pg/mL) 61.02±9.37 61.17±9.48 0.08 0.94 37.44±6.12* 49.67±8.21* 8.28 < 0.01 VEGF(μg/L) 219.36±40.02 220.08±39.91 0.09 0.93 431.60±57.08* 331.26±70.02* 7.70 < 0.01 BDNF(μg/L) 1.77±0.43 1.78±0.41 0.12 0.91 2.97±0.79* 1.97±0.94* 5.64 < 0.01 NSE(μg/L) 37.38±4.35 37.79±4.26 0.47 0.64 16.54±2.73* 29.28±5.12* 15.21 < 0.01 s100β(μg/L) 2.06±0.34 2.10±0.30 0.61 0.54 1.40±0.27* 1.91±0.31* 8.60 < 0.01 *P<0.05 vs 同组治疗前. ET-1: 内皮素-1; TXB2: 血栓素 B2; AngⅡ: 血管紧张素Ⅱ; VEGF: 血管内皮生长因子; BDNF: 脑源性神经营养因子; NSE: 神经元特异性烯醇化酶.
下载: 导出CSV
表 4 两组患者治疗前后认知功能比较
Table 4. Comparison of cognitive function between the two groups before and after treatment (n=48, Mean±SD)
认知功能 研究组 对照组 t治疗后 P治疗后 治疗前 治疗后 治疗前 治疗后 时间定向力 1.10±0.31 2.42±0.67* 1.09±0.25 1.59±0.38* 7.47 < 0.01 地点定向力 1.11±0.14 2.51±0.35* 1.12±0.28 1.79±0.29* 10.98 < 0.01 即刻记忆 1.08±0.21 2.58±0.41* 1.10±0.21 1.87±0.37* 8.91 < 0.01 延迟记忆 1.07±0.13 2.51±0.43* 1.03±0.20 1.89±0.24* 8.72 < 0.01 注意力 1.31±0.20 2.57±0.36* 1.27±0.26 1.81±0.32* 10.93 < 0.01 计算力 1.01±0.12 2.60±0.51* 1.04±0.16 1.86±0.26* 8.96 < 0.01 语言能力 3.40±1.12 5.67±1.18* 3.18±1.13 3.79±1.34* 7.3 < 0.01 视空间力 3.54±1.05 5.69±1.12* 3.67±1.17 4.39±1.47* 4.87 < 0.01 MMSE总分 13.69±3.18 27.07±7.18* 13.57±3.37 18.99±4.08* 6.78 < 0.01 *P<0.05 vs同组治疗前.
下载: 导出CSV
-
[1] 呼格吉乐, 丛殿宝, 张建辉, 等. 阿司匹林+氯吡格雷双联抗血小板聚集联合丁苯酞治疗高龄急性大脑中动脉缺血性脑卒中的疗效[J]. 中国老年学杂志, 2019, 39(21): 5183-6. doi: 10.3969/j.issn.1005-9202.2019.21.013 [2] 单娜, 赵丽, 林晓东. 首发急性缺血性脑卒中患者认知障碍发生的危险因素及对Lp-PLA2、sCD40L的相关性研究[J]. 川北医学院学报, 2022, 37(6): 754-8. https://www.cnki.com.cn/Article/CJFDTOTAL-NOTH202206017.htm [3] 李蕾, 李远庆, 迟淑萍, 等. CT灌注成像快速评估脑组织缺血半暗带指导拓宽脑卒中治疗时间窗的可行研究[J]. 中国医学装备, 2021, 18(3): 76-80. doi: 10.3969/J.ISSN.1672-8270.2021.03.019 [4] 路永坤, 王新志, 刘向哲, 等. 参归通络汤对严重狭窄大脑中动脉远端脑组织低灌注区侧支循环的影响[J]. 中国老年学杂志, 2020, 40(7): 1376-9. doi: 10.3969/j.issn.1005-9202.2020.07.010 [5] 卢芳环, 历金财, 宋兰英, 等. 丁苯酞结合通神复脑丸治疗循环缺血性眩晕患者的疗效及对血清PAF、TXB2表达的影响[J]. 中国急救复苏与灾害医学杂志, 2021, 16(6): 650-3. doi: 10.3969/j.issn.1673-6966.2021.06.017 [6] 王磊磊, 胡方梅, 陈华, 等. 抽提透刺法对脑梗死模型大鼠脑的保护机制及对CXCL12-CXCR4信号通路的作用研究[J]. 陕西中医, 2020, 41(11): 1524-8. https://www.cnki.com.cn/Article/CJFDTOTAL-SXZY202011003.htm [7] 柳翔耀, 梁爽. 高分辨率MR血管壁成像对脑梗死患者颅内动脉狭窄、闭塞的诊断价值分析[J]. 中国医学工程, 2022, 30(5): 36-9. https://www.cnki.com.cn/Article/CJFDTOTAL-YCGC202205008.htm [8] 杨敏. 大脑中动脉不同程度狭窄患者认知功能损害的特点[D]. 石河子: 石河子大学, 2017. [9] Jadhav AP, Diener HC, Bonafe A, et al. Correlation between clini caloutcomes and baseline CT and CT angiographic findings in the SWIFT PRIME trial[J]. AJNR Am J Neuroradiol, 2017, 38(12): 2270-6. doi: 10.3174/ajnr.A5406 [10] 邓奇. 丁苯酞治疗后循环脑梗死的疗效及对神经功能缺损的影响[J]. 川北医学院学报, 2018, 33(6): 933-5. doi: 10.3969/j.issn.1005-3697.2018.06.035 [11] 余王梅, 黄芸, 张宇宇. 丁苯酞治疗短暂性脑缺血发作疗效及安全性的Meta分析[J]. 健康研究, 2020, 40(4): 439-44. doi: 10.3969/j.issn.1674-6449.2020.04.020 [12] 陈开民, 黄丹, 吕艳, 等. 丁苯酞联合奥扎格雷钠对急性脑梗死的应用效果及对神经细胞功能、氧化应激水平的影响[J]. 中华保健医学杂志, 2021, 23(3): 287-9. doi: 10.3969/j.issn.1674-3245.2021.03.023 [13] 孙红, 王涛. 血府逐瘀汤对激光光凝术后眼底病患者眼部血流动力学及视觉功能的影响[J]. 湖北中医药大学学报, 2021, 23(1): 32-6. https://www.cnki.com.cn/Article/CJFDTOTAL-HZXX202101008.htm [14] 李兰辰, 金晓宇, 曾学清. 头穴针刺结合尼莫地平治疗脑卒中后轻度认知功能障碍的临床研究[J]. 中医药导报, 2019, 25(22): 49-52. https://www.cnki.com.cn/Article/CJFDTOTAL-HNZB201922015.htm [15] 吉贞料, 王高岸, 张长杰. 头穴透刺联合持续经颅磁刺激治疗脑卒中后运动功能障碍疗效观察[J]. 现代中西医结合杂志, 2021, 30(8): 830-3, 860. doi: 10.3969/j.issn.1008-8849.2021.08.007 [16] 赵文瑾. 丁苯酞联合针刺对急性缺血性脑卒中患者神经功能的影响[J]. 西南国防医药, 2019, 29(2): 149-51. https://www.cnki.com.cn/Article/CJFDTOTAL-XNGF201902018.htm [17] 占振瀛, 王安荔, 王志杰. 丁苯酞氯化钠注射液联合温针灸治疗进展性脑卒中临床研究[J]. 新中医, 2021, 53(19): 173-6. https://www.cnki.com.cn/Article/CJFDTOTAL-REND202119037.htm [18] Zhang J, Luo WJ, Li QY, et al. Peripheral brain-derived neurotrophicfactor in attention- deficit/hyperactivity disorder: a comprehensivesystematic review and meta-analysis[J]. J Affect Disord, 2018, 227: 298-304. [19] 李清华, 侯双兴, 杨化兰, 等. 丹红注射液联合丁苯酞注射液对急性脑梗死病人BDNF、NPY和NSE的影响[J]. 中西医结合心脑血管病杂志, 2020, 18(7): 1148-51. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYYY202007030.htm [20] 牛磊, 秦合伟, 孔艳芳. 头穴丛刺长留针法联合认知功能训练治疗脑梗死后认知功能障碍临床研究[J]. 中西医结合研究, 2021, 13(6): 377-80, 388. https://www.cnki.com.cn/Article/CJFDTOTAL-ZXYH202106005.htm -

 点击查看大图
点击查看大图
计量
- 文章访问数: 151
- HTML全文浏览量: 65
- PDF下载量: 4
- 被引次数: 0