



Prediction of cervical lymph node metastasis of thyroid papillary carcinoma by ECI and SWE quantitative parameters
-
摘要:
目的 研究超声弹性对比指数(ECI)、剪切波弹性成像(SWE)定量参数预测甲状腺乳头癌颈部淋巴结转移的价值。 方法 选取2018年1月~2021年12月我院收治的甲状腺乳头状癌患者60例,将淋巴结转移者纳入淋巴转移组(n=21),未转移者纳入淋巴未转移组(n=39)。分别对两组患者的超声图像、ECI、SWEmax、SWEmin、SWEmean进行比较, 分析ECI、SWEmax、SWEmin、SWEmean联合检测对甲状腺乳头状瘤患者淋巴转移的预测效能。 结果 两组患者的纵横比、结节数量、边缘、钙化、与被膜的关系、血流信号之间的差异有统计学意义(P < 0.05);淋巴转移组患者的ECI高于淋巴未转移组(P < 0.05),淋巴转移组患者的SWEmax、SWEmin、SWEmean低于对照组(P < 0.05);ECI、SWEmax、SWEmin、SWEmean联合检测对甲状腺乳头状瘤患者淋巴转移的特异性高于单独检测。ROC曲线分析显示,ECI、SWEmax、SWEmin、SWEmean联合检测对甲状腺乳头状瘤患者淋巴转移的曲线下面积高于单独检测,ECI、SWEmax、SWEmin、SWEmean的截断值分别为4.61、30.11 kPa、21.98 kPa、25.55 kPa。 结论 ECI、SWE定量参数对于甲状腺乳头癌颈部淋巴结转移具有显著的预测价值。 Abstract:Objective To analyze the value of elastic contrast index (ECI) and shear wave elastography (SWE) quantitative parameters in predicting cervical lymph node metastasis of thyroid papillary carcinoma. Methods Sixty patients with thyroid papillary carcinoma admitted to our hospital from January 2018 to December 2021 were selected, including 21 patients with lymph node metastasis and 39 patients without lymph node metastasis. The differences of ultrasound images, ECI, SWEmax, SWEmin and SWEmean between the two groups were compared. We analyzed the predictive efficacy of ECI, SWEmax, SWEmin and SWEmean combined detection for lymphatic metastasis in patients with thyroid papilloma. Results There were statistically significant differences in aspect ratio, number of nodules, margin, calcification, relationship with capsule and blood flow signals between the two groups (P < 0.05). ECI in lymphatic metastasis group was significantly higher than that in non-lymphatic metastasis group (P < 0.05). SWEmax, SWEmin and SWEmean in lymphatic metastasis group were significantly lower than those in control group (P < 0.05). The specificity of ECI, SWEmax, SWEmin and SWEmean combined detection for lymphatic metastasis in patients with thyroid papilloma was significantly higher than that of single detection. According to ROC curve analysis, the area under curve of lymphatic metastasis in patients with thyroid papilloma by ECI, SWEmax, SWEmin and SWEmean combined detection were significantly higher than that by single detection. The truncation values of ECI, SWEmax, SWEmin and SWEmean were 4.61, 30.11 kPa, 21.98 kPa and 25.55 kPa, respectively. Conclusion ECI and SWE quantitative parameters have significant predictive value for cervical lymph node metastasis of thyroid papillary carcinoma, suggesting clinical promotion. -

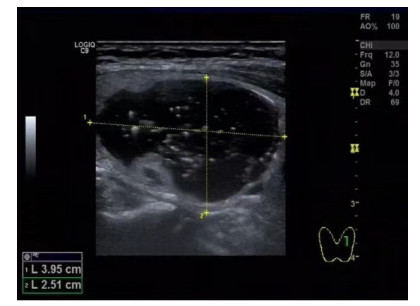
图 1 甲状腺乳头状癌患者,男,48岁
右叶下极实性结节, 边界欠清, 内部回声不均, 周边可见点状钙化, CDFI: 血流信号丰富. TI-RADS分类4c级, 弹性成像评分5分. 颈部淋巴结肿大. FNA结果为甲状腺乳头状癌.
Figure 1. A48-year-old male patient with thyroid papillary carcinoma.

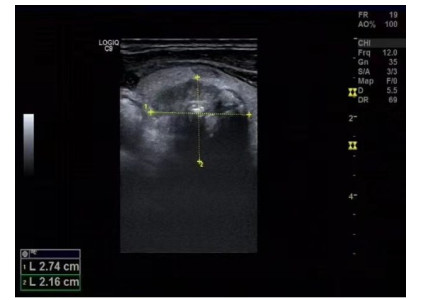
图 2 甲状腺乳头状癌患者,女,55岁
右叶上极中层实性结节, 边界欠清, 形态不规则, 内部回声不均, 周边可见点状钙化, 有低回声晕, 纵横比 > 1, TI-RADS分类4c级, 弹性成像评分6分. 颈部淋巴结肿大. FNA结果为甲状腺乳头状癌.
Figure 2. A55-year-old female patient with thyroid papillary carcinoma.

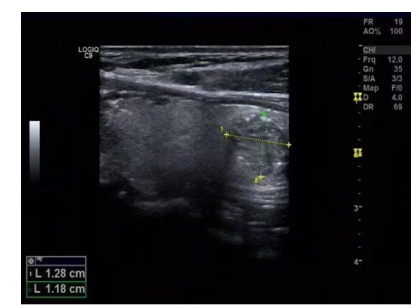
图 3 甲状腺乳头状癌患者,男,48岁
甲状腺左叶囊实性结节, 边界清, 形态规则,内部呈胶质样回声, 内壁可见乳头状突起, CDFI: 周边可见丰富血流信号; TI-RADS分类4b级, 弹性成像评分4分. 手术病理结果为甲状腺乳头状癌.
Figure 3. A 48-year-old male patient with thyroid papillary carcinoma.

图 4 甲状腺乳头状癌患者,女,44岁
甲状腺左叶实性结节, 边界不清, 形态欠规则, 内部回声不均, 周边及内部可见点簇状强回声, 后方回声衰减. 颈部多个淋巴结肿大, 形态异常. CD-FI: 周边可见丰富血流信号; TI-RADS分类5级, 弹性成像评分6分. 手术病理结果为甲状腺乳头状癌.
Figure 4. A44-year-old female patient with thyroid papillary carcinoma.
表 1 两组患者一般资料比较
Table 1. General data comparison of two groups(Mean±SD)
组别 性别(男/女, n) 年龄(岁) BMI(kg/m2) 淋巴转移组(n=21) 4/17 45.69±2.47 24.55±5.41 淋巴未转移组(n=39) 7/32 45.81±3.52 24.94±5.33 χ2/t 1.701 0.154 0.268 P 0.193 0.878 0.790  下载: 导出CSV
下载: 导出CSV
表 2 两组患者的常规超超声指标分析
Table 2. Analysis of conventional ultra-ultrasound indexes of the two groups [n(%)]
指标 淋巴转移组(n =21) 淋巴未转移组(n =39) χ2 P 纵横比 6.971 0.008 < 1 18(47.37) 20(52.63) ≥1 3(13.64) 19(86.36) 结节数量 13.301 < 0.001 单发 6(16.67) 30(83.33) 多发 15(62.50) 9(37.50) 实质背景 0.221 0.896 正常 10(33.33) 20(66.67) 桥本 5(33.33) 10(66.67) 结甲 6(40.00) 9(60.00) 实质回声 0.022 0.988 中等回声 11(35.48) 20(64.52) 低回声 5(33.33) 10(66.67) 极低回声 5(35.71) 9(64.29) 边缘 32.701 < 0.001 规则 19(79.17) 5(20.83) 不规则 2(5.88) 32(94.12) 钙化 27.121 < 0.001 无钙化 10(83.33) 2(16.67) 粗大钙化 2(6.25) 30(93.75) 微小钙化 9(56.25) 7(43.75) 与被膜关系 47.581 < 0.001 未接触 19(95.00) 1(5.00) 接触 2(6.25) 30(93.75) 不连续 0(0.00) 8(100.00) 血流 47.761 < 0.001 I型 20(90.91) 2(9.09) II型 1(3.45) 28(96.55) III型 0(0.00) 9(100.00)
下载: 导出CSV
表 3 两组患者的ECI、SWEmax、SWEmin、SWEmean比较
Table 3. Comparison of ECI, SWEmax, SWEmin and SWEmean between the two groups (Mean±SD)
指标 淋巴转移组(n =21) 淋巴未转移组(n =39) t P ECI 4.63±1.48 2.42±0.32 6.758 < 0.001 SWEmax(kPa) 30.02±2.72 35.36±3.23 6.783 < 0.001 SWEmin(kPa) 21.81±3.87 25.08±2.95 3.379 0.001 SWEmean(kPa) 25.77±2.45 28.57±2.66 4.096 < 0.001 ECI: 超声弹性对比指数; SWE: 甲状腺弹性值.
下载: 导出CSV
表 4 ECI、SWEmax、SWEmin、SWEmean联合检测对甲状腺乳头状瘤患者淋巴转移的预测效能分析
Table 4. Efficacy analysis of ECI, SWEmax, SWEmin and SWEmean combined detection in predicting lymphatic metastasis in patients with thyroid papilloma
诊断方法 真阳例数(n) 假阳例数(n) 真阴例数(n) 假阴例数(n) 准确率(%) 敏感度(%) 特异性(%) 阳性预测值(%) 阴性预测值(%) ECI 15 11 28 6 71.67 34.88 82.35 71.43 71.79 SWEmax 9 12 27 12 60.00 25.00 69.23 42.86 69.23 SWEmin 19 22 17 2 60.00 52.78 89.47 90.48 43.59 SWEmean 13 32 7 8 33.33 65.00 46.67 61.90 17.95 联合检测 20 29 10 1 50.00 66.67 90.91 95.24 25.64
下载: 导出CSV
表 5 ROC曲线分析
Table 5. ROC curve analysis
诊断方法 标准误 曲线下面积 AUC(95% CI) P ECI 0.039 0.775 0.520~0.872 0.017 SWEmax 0.036 0.603 0.600~0.746 < 0.001 SWEmin 0.03 0.692 0.607~0.816 < 0.001 SWEmean 0.027 0.778 0.762~0.869 < 0.001 联合检测 1.027 0.792 0.762~0.870 < 0.001
下载: 导出CSV
-
[1] 孙芳, 石岩, 杨智, 等. 剪切波联合二维超声对甲状腺乳头状癌中央区淋巴结转移的预测价值[J]. 实用医学杂志, 2021, 37(14): 1866-71. https://www.cnki.com.cn/Article/CJFDTOTAL-SYYZ202114019.htm [2] 江鑫辉, 陈捷, 王媚瑜, 等. 超声造影对无淋巴结转移甲状腺微小乳头状癌侵袭性的诊断价值[J]. 中国临床医学影像杂志, 2020, 31(5): 320-4, 367. https://www.cnki.com.cn/Article/CJFDTOTAL-LYYX202005006.htm [3] 刘娜香, 唐丽娜, 沈友洪, 等. 超声造影联合穿刺洗脱液甲状腺球蛋白测定在诊断甲状腺乳头状癌侧颈部转移淋巴结中的应用价值[J]. 中华超声影像学杂志, 2020, 29(12): 1060-6. [4] 王晶, 鹿皎, 王荣, 等. 甲状腺乳头状癌常规超声图像特征及声触诊组织成像预测颈部淋巴结转移的价值研究[J]. 中国临床医学影像杂志, 2020, 31(1): 11-4. https://www.cnki.com.cn/Article/CJFDTOTAL-LYYX202001007.htm [5] 黄元发, 邓峰, 许辉, 等. DWI联合超声评估无淋巴结转移单发甲状腺微小乳头状癌侵袭性的研究[J]. 放射学实践, 2020, 35(7): 850-4. https://www.cnki.com.cn/Article/CJFDTOTAL-FSXS202007009.htm [6] 李俨育, 王茜, 范公林, 等. 基于超声与细针穿刺洗脱液甲状腺球蛋白检测建立甲状腺乳头状癌颈侧区淋巴结转移的预测模型[J]. 中华超声影像学杂志, 2020(2): 131-7. [7] 刘文, 闫雪晶, 程若川, 等. 术前临床及超声检查特征对甲状腺乳头状癌中央区淋巴结转移预测价值研究[J]. 中国实用外科杂志, 2020, 40(10): 1197-201. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGWK202010030.htm [8] 纪岩松, 谷昊, 薛乐刚. 最大信号投影、峰值强度与甲状腺乳头状癌患者微血管密度及颈部淋巴结转移的相关性[J]. 中国临床医学影像杂志, 2021, 32(12): 846-8, 852. [9] 穆维娜, 刘克, 刘颖, 等. 超声误诊甲状腺癌合并颈部肉芽肿性淋巴结炎为甲状腺癌颈部淋巴结转移[J]. 中国介入影像与治疗学, 2021, 18(8): 512. https://www.cnki.com.cn/Article/CJFDTOTAL-JRYX202108027.htm [10] 谭学礼, 刘轼初, 钟晓玲, 等. 甲状腺微小乳头状癌中央区淋巴结转移复发相关因素研究分析[J]. 影像科学与光化学, 2020, 38(6): 1032-7. https://www.cnki.com.cn/Article/CJFDTOTAL-GKGH202006020.htm [11] 刘雅静, 陈雅玲, 王芬, 等. 单发甲状腺乳头状癌强回声分类与侧颈淋巴结转移的相关性研究[J]. 中华超声影像学杂志, 2020, 29(7): 597-601. [12] Yoon J, Yoon JH, Han K, et al. Ultrasonography surveillance in papillary thyroid carcinoma patients after total thyroidectomy according to dynamic risk stratification[J]. Endocrine, 2020, 69(2): 347-57. [13] Khatami F, Larijani B, Heshmat R, et al. Hypermethylated RASSF1 and SLC5A8 promoters alongside BRAF V600E mutation as biomarkers for papillary thyroid carcinoma[J]. J Cell Physiol, 2020, 235(10): 6954-68. [14] Canberk S, Montezuma D, Ince U, et al. Variants of papillary thyroid carcinoma: an algorithmic cytomorphology-based approach to cytology specimens[J]. Acta Cytol, 2020, 64(4): 288-98. [15] Trimboli P, Castellana M, Piccardo A, et al. The ultrasound risk stratification systems for thyroid nodule have been evaluated against papillary carcinoma[J]. Rev Endocr Metab Disord, 2021, 22(2): 453-60. [16] 孙建锋. 实时超声弹性成像在甲状腺乳头状癌诊断中的应用价值[J]. 分子影像学杂志, 2016, 39(4): 356-8. doi: 10.3969/j.issn.1674-4500.2016.04.04 [17] Calapkulu M, Sencar ME, Duger H, et al. Coexistence of type-1 diabetes mellitus and papillary thyroid carcinoma[J]. Curr Diabetes Rev, 2020, 16(7): 787-9. [18] Guo D, Li FY, Zhao XX, et al. Circular RNA expression and association with the clinicopathological characteristics in papillary thyroid carcinoma[J]. Oncol Rep, 2020, 44(2): 519-32. [19] Wang duo-ping, Tang xiao-zhun, Liang quan-kun, et al. microRNA- 599 promotes apoptosis and represses proliferation and epithelial- mesenchymal transition of papillary thyroid carcinoma cells via downregulation of Hey2-depentent Notch signaling pathway[J]. J Cell Physiol, 2020, 235(3): 2492-505. [20] 栾艳艳, 郑云, 王玉玲, 等. SWE定量技术评价cN0期甲状腺乳头状癌中央区淋巴结的价值[J]. 医学影像学杂志, 2022, 32(7): 1135-8. https://www.cnki.com.cn/Article/CJFDTOTAL-XYXZ202207012.htm -


 点击查看大图
点击查看大图
计量
- 文章访问数: 145
- HTML全文浏览量: 95
- PDF下载量: 4
- 被引次数: 0