



Comparison of copeptin, C-reactive protein and D-dimer levels before and after endoscopic retrograde cholangiopancreatography surgery in acute biliary pancreatitis
-
摘要:
目的 探讨经内镜逆行性胰胆管造影术(ERCP)治疗急性胆源性胰腺炎前后和肽素(CPT)、C-反应蛋白(CRP)及D-二聚体(D-D)水平变化。 方法 选取2018年5月~2020年3月在我院住院治疗的95例急性胆源性胰腺炎患者为研究对象,按照随机数字表法将患者分为对照组(n=47)和观察组(n=48),对照组采用传统开腹手术治疗,观察组采用ERCP手术治疗。比较两组患者临床疗效、临床症状恢复时间及并发症情况,观察治疗前后CPT、CRP、D-D水平变化情况。 结果 与对照组比较,观察组治疗总有效率更高(97.92% vs 87.23%,P < 0.05)。手术后1 d、4 d的CPT、CRP、D-D水平较手术前均有下降,且观察组下降幅度较对照组大(P < 0.05)。与对照组相比,观察组腹部疼痛缓解时间、胃肠功能及肝功能恢复时间均较短(P < 0.05)。与对照组相比,观察组住院时间较短,住院费用也较低,且并发症发生率较低(P < 0.05)。 结论 ERCP手术治疗急性胆源性胰腺炎有较好的治疗效果,术后CPT、CRP及D-D水平及临床症状均明显改善,且并发症少,安全性较高。 Abstract:Objective To investigate the changes of copeptin (CPT), C- reactive protein (CRP) and D- dimer (D- D) levelsbefore and after the treatment of acute biliary pancreatitis by endoscopic retrograde cholangiopancreatography (ERCP). Methods Ninety- five patients with acute biliary pancreatitis in our hospital from May 2018 to March 2020 were selected and divided into control group (n=47) and observation group (n=48) according to the random number table method . The control group was treated with traditional open surgery, and theobservation group was treated with ERCP. The clinicalefficacy, clinical symptoms recovery time and complications of the two groups were compared, and changes in CPT, CRP, and D-D levels were observed before and after treatment. Results Compared with the control group (87.23%), the total effective rate of observation group (97.92%) was significantly higher (P < 0.05). The levels of CPT, CRP, and D-D at 1 d and 4 d after the operation were lower than before the operation, and the decrease in the observation group was larger than that of the control group (P < 0.05). Compared with the control group, the observation group had shorter abdominal pain relief time, gastrointestinal function and liver function recovery time (P < 0.05). Compared with the control group, the observation group had shorter hospital stays and lower hospitalization costs, lower complication rate (P < 0.05). Conclusion ERCP surgery has a good effect in the treatment of acute biliarypancreatitis. Postoperative CPT, CRP and D-D levels and clinical symptomsare significantly improved, with fewercomplications and high safety. -

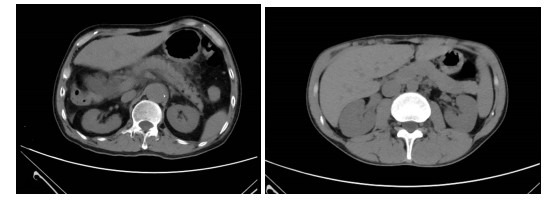
图 1 患者男,53岁,因急性胆源性胰腺炎接受ERCP治疗
A: 手术前; B: 手术1月后.
Figure 1. A 53-year-old male patient received ERCP for acute biliary pancreatitis.
表 1 两组患者临床疗效比较
Table 1. Comparison of clinical efficacy between the two groups[n(%)]
组别 显效 有效 无效 总有效率 对照组(n=47) 31(65.96) 10(21.28) 6(12.77) 41(87.23) 观察组(n=48) 38(79.17) 9(18.75) 1(2.08) 47(97.92) χ2 3.970 P 0.046  下载: 导出CSV
下载: 导出CSV
表 2 两组患者治疗前后CPT、CRP及D-D水平比较
Table 2. Comparison of CPT, CRP and D-D levels between the two groups before and after treatment (Mean± SD)
时间 组别 CPT(pg/mL) CRP(mg/L) D-D(mg/L) 术前 对照组(n=47) 198.37±35.60 95.45±23.38 3.45±1.20 观察组(n=48) 200.15±35.45 96.07±23.50 3.51±1.28 t 0.244 0.128 0.235 P 0.807 0.897 0.814 术后1 d 对照组(n=47) 121.60±26.16 91.57±18.59 2.95±0.96 观察组(n=48) 110.27±25.34 82.65±19.90 2.52±0.93 t 2.144 2.256 2.217 P 0.034 0.026 0.029 术后4 d 对照组(n=47) 98.17±22.40 52.56±11.23 1.75±0.60 观察组(n=48) 85.35±21.34 37.80±10.56 1.18±0.49 t 2.856 6.600 5.076 P 0.005 < 0.001 < 0.001 CPT: 肽素; CRP: C反应蛋白; D-D: D-二聚体.
下载: 导出CSV
表 3 两组患者临床症状恢复时间比较
Table 3. Comparison of recovery time of clinical symptoms between the two groups (d, Mean±SD)
组别 腹部疼痛缓解时间 胃肠功能恢复时间 肝功能恢复时间 对照组(n=47) 3.52±1.15 8.28±2.14 10.62±2.30 观察组(n=48) 1.55±1.08 4.50±1.80 7.40±1.77 t 8.608 10.133 7.656 P < 0.001 < 0.001 < 0.001
下载: 导出CSV
表 4 两组患者住院时间、住院费用及术后并发症比较
Table 4. Comparison of hospital stay, hospitalization cost and postoperative complications between the two groups (Mean±SD)
组别 住院时间(d) 住院费用(万元) 并发症[n(%)] 对照组(n=47) 18.75±3.48 2.62±0.51 4(8.51) 观察组(n=48) 10.78±2.87 1.47±0.46 1(2.08) t 12.189 11.545 1.967 p < 0.001 < 0.001 0.160
下载: 导出CSV
-
[1] 王海, 胥明, 陈曲. 急性胆源性胰腺炎的病因学研究进展[J]. 国际消化病杂志, 2018, 38(1): 16-8. doi: 10.3969/j.issn.1673-534X.2018.01.004 [2] 冯磊, 张轶, 徐德全, 等. 急性胆源性胰腺炎诊治进展[J]. 中国普外基础与临床杂志, 2019, 26(4): 508-12. https://www.cnki.com.cn/Article/CJFDTOTAL-ZPWL201904025.htm [3] Coutinho L, Bernardo WM, Rocha RS, et al. Early endoscopic retrograde cholangiopancreatography versus conservative treatment in patients with acute biliary pancreatitis: systematic review and Meta-analysis of randomized controlled trials[J]. Pancreas, 2018, 47 (4): 444-53. doi: 10.1097/MPA.0000000000001032 [4] Muniraj T, Whiting PF, Sundaram RS, et al. Mo1237-rapid urinary trypsinogen test in early point-of-care diagnosis of acute pancreatitis and post-ERCP pancreatitis: a systematic review[J]. Gastroenterology, 2018, 154(6): S-714. [5] 李鸿晔, 王迪迪, 洪江龙, 等. 吲哚美辛对经内镜逆行胰胆管造影术后胰腺炎患者血小板微粒水平的影响[J]. 中华消化内镜杂志, 2021, 38 (10): 840-4. doi: 10.3760/cma.j.cn321463-20210208-00098 [6] 陈文华, 林军, 王红玲, 等. 内镜下逆行性胰胆管造影术后急性胰腺的危险因素分析[J]. 中华全科医师杂志, 2019, 18(3): 256-60. doi: 10.3760/cma.j.issn.1671-7368.2019.03.010 [7] 顾林, 郑海伦, 赵睿, 等. 行治疗性内镜下逆行性胰胆管造影术超高龄胆胰病病人的临床特征分析[J]. 蚌埠医学院学报, 2021, 46(4): 499-503. https://www.cnki.com.cn/Article/CJFDTOTAL-BANG202104021.htm [8] 赖嘉文, 刘孝高, 张相森. 经内镜逆行胰胆管造影术在胆源性胰腺炎诊疗中的应用[J]. 中国现代普通外科进展, 2019, 22(6): 468-71. https://www.cnki.com.cn/Article/CJFDTOTAL-PWJZ201906015.htm [9] 王兴鹏, 许国铭, 袁耀宗, 等. 中国急性胰腺炎诊治指南(草案)[J]. 现代消化及介入诊疗, 2007, 12(3): 206-8. doi: 10.3969/j.issn.1672-2159.2007.03.021 [10] 邹卫华, 姜斌, 孙权, 等. ERCP治疗急性胆源性胰腺炎的时机及临床疗效分析[J]. 国际外科学杂志, 2019(6): 396-401. doi: 10.3760/cma.j.issn.1673-4203.2019.06.009 [11] 殷涛, 吴河水. 急性胆源性胰腺炎的诊断和治疗[J]. 临床急诊杂志, 2021, 22(3): 157-60. https://www.cnki.com.cn/Article/CJFDTOTAL-ZZLC202103001.htm [12] 黄秋林, 曾奎, 陈豪, 等. Apelin-13对急性坏死性胰腺炎大鼠胰腺组织中自噬的影响[J]. 中南医学科学杂志, 2021, 49(3): 295-9. https://www.cnki.com.cn/Article/CJFDTOTAL-HYYY202103010.htm [13] 冯秋实, 杨尹默. 急性胆源性胰腺炎合并急性重症胆管炎处理策略[J]. 中国实用外科杂志, 2020, 40(11): 1282-5. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGWK202011017.htm [14] 徐国栋, 张卫国, 张宇飞, 等. 腹腔镜手术和开腹手术治疗急性胆源性胰腺炎的疗效及安全性分析[J]. 中国临床医生杂志, 2020, 48(10): 1210-2. doi: 10.3969/j.issn.2095-8552.2020.10.022 [15] 唐义龙, 方晨光, 吴文伟, 等. 急性胆源性胰腺炎继发胰腺坏死高危因素及预测模型分析[J]. 创伤与急危重病医学, 2020, 8(2): 104-6, 109. https://www.cnki.com.cn/Article/CJFDTOTAL-CSJB202002012.htm [16] 向飞. 早期手术治疗胆源性胰腺炎的临床研究[J]. 肝胆外科杂志, 2018, 26(1): 27-30. https://www.cnki.com.cn/Article/CJFDTOTAL-GDWZ201801008.htm [17] 韩林, 郭辰晗, 韩宏民, 等. PTGD与ERCP在重症急性胆源性胰腺炎早期应用的临床疗效比较[J]. 大连医科大学学报, 2019, 41(2): 148-55. https://www.cnki.com.cn/Article/CJFDTOTAL-DLYK201902014.htm [18] 于源泉, 李江涛. 内镜技术在急性胆源性胰腺炎诊治中的合理应用[J]. 中国实用外科杂志, 2017, 37(8): 923-4, 936. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGWK201708030.htm [19] 姜欣, 姜功文, 刘莹, 等. ERCP术治疗急性胆源性胰腺炎的临床价值研究[J]. 中国实用医药, 2021, 16(15): 80-2. https://www.cnki.com.cn/Article/CJFDTOTAL-ZSSA202115028.htm [20] 杨晓龙. 急性胆源性胰腺炎治疗中经内镜逆行性胰胆管造影术临床疗效分析[J]. 中国现代医药杂志, 2019, 21(4): 80-2. https://www.cnki.com.cn/Article/CJFDTOTAL-ZHTY201904025.htm [21] 武星君, 饶艳华, 王兆雄. ERCP术治疗急性胆源性胰腺炎的综合效果及对AMYL、TBIL、ALT、CRP的影响[J]. 中国保健营养, 2018, 28 (10): 35-6. https://www.cnki.com.cn/Article/CJFDTOTAL-YLYS201831006.htm [22] 吉其舰, 许铁. 和肽素水平对重症肺炎严重程度的评价作用[J]. 现代医学, 2018, 46(7): 745-7. https://www.cnki.com.cn/Article/CJFDTOTAL-TDYX201807003.htm [23] 李晓玲, 李芳芳, 尹佳萌, 等. 血清中性粒细胞明胶酶相关载脂蛋白、核转录因子-κB及血清肌酐对重症急性胰腺炎伴急性肾损伤的预测价值[J]. 中华生物医学工程杂志, 2022(1): 49-53. [24] 傅宣, 何政, 王港, 等. 免疫微生态营养对重症急性胰腺炎患者炎症反应、免疫功能及肠黏膜屏障功能影响研究[J]. 创伤与急危重病医学, 2022, 10(2): 115-8, 123. https://www.cnki.com.cn/Article/CJFDTOTAL-CSJB202202009.htm [25] 蒋立钊, 刘石. 血清和肽素在亚特兰大新分类标准下预测急性胰腺炎严重程度的价值研究[J]. 胃肠病学和肝病学杂志, 2018, 27(7): 808-12. https://www.cnki.com.cn/Article/CJFDTOTAL-WCBX201807023.htm [26] Zhao G, Zhuo YZ, Cui LH, et al. Modified Da-Chai-hu Decoction regulates the expression of occludin and NF-κB to alleviate organ injury in severe acute pancreatitis rats[J]. Chin J Nat Med, 2019, 17 (5): 355-62. [27] 马力, 李晓锋, 熊燃, 等. 超声引导下经皮穿刺置管引流术的应用时机对中度重症急性胰腺炎的疗效[J]. 分子影像学杂志, 2021, 44(6): 917-21. https://www.cnki.com.cn/Article/CJFDTOTAL-FZYX202106006.htm [28] 赵登秋, 陈益鸣, 邬叶锋, 等. 早期内镜治疗老年急性胆源性胰腺炎对炎症因子及临床疗效的影响[J]. 中华内分泌外科杂志, 2021(5): 514-7. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 108
- HTML全文浏览量: 43
- PDF下载量: 1
- 被引次数: 0