



Evaluated value of CT perfusion imaging on cerebral tissue blood perfusion, cerebral collateral blood circulation status and responsible vessel stenosis in patients with acute ischemic stroke
-
摘要:
目的 探究CT灌注成像(CTPI)对急性缺血性脑卒中患者脑组织血流灌注情况、脑侧支血流循环状态及责任血管狭窄的评估价值。 方法 选取攀枝花市中西医结合医院2021年3月~2022年3月收治的51例急性缺血性脑卒中患者,入院后行CT平扫及CT灌注成像。分析患者不同区域脑血流量(CBF)、脑血容量(CBV)、对比剂平均通过时间(MTT)、对比剂峰值时间(TTP),比较不同侧支血流循环状态CTPI参数情况及责任血管不同狭窄程度。 结果 CTPI显示,46例脑组织血流灌注发生异常,CTPI阳性率为90.20%(46/51)。患者患侧梗死病灶区及缺血半暗带CBF值、CBV值均小于健侧,MTT值、TTP值均长于健侧(P < 0.05)。侧支循环良好者患侧CBF值小于健侧,MTT值及TTP值均长于健侧(P < 0.05),而患侧与健侧CBV值比较差异无统计学意义(P > 0.05);侧支循环不良者患侧CBF值及CBV值均小于健侧,且MTT值及TTP值均长于健侧(P < 0.05)。CTPI提示AIS脑组织血流灌注异常患者责任血管重度狭窄或闭塞发生率高于CTPI提示血流灌注正常患者(P < 0.05)。 结论 CTPI可及时准确反映急性缺血性脑卒中患者梗死病灶区、缺血半暗带血流灌注情况,有助于临床掌握患者侧支循环状态,对责任血管狭窄程度进行客观评估。 Abstract:Objective To explore the evaluated value of CT perfusion imaging (CTPI) on cerebral tissue blood perfusion, cerebral collateral blood circulation status and responsible vessel stenosis in patients with acute ischemic stroke. Methods Fifty- one patients with acute ischemic stroke who were treated in Panzhihua Hospital of Integrated Traditional Chinese and Western Medicine were selected from March 2021 to March 2022, and they underwent CT plain scan and CT perfusion imaging after admission. The cerebral blood flow (CBF), cerebral blood volume (CBV), mean transit time (MTT) and time to peak (TTP) in different regions of patients were analyzed. CTPI parameters in different collateral blood circulation status and different stenosis degrees of responsible vessels were compared. Results CTPI of patients with AIS showed abnormal cerebral tissue blood perfusion in 46 cases, with the positive rate of CTPI was 90.20% (46/51). The CBF and CBV of the infarcted lesion area and ischemic penumbra of the affected side were lower than those of the healthy side. The MTT and TTP were longer than those of the healthy side (P < 0.05). Among patients with good collateral circulation, the CBF value of the affected side was lower than that of the healthy side, and the MTT and TTP were longer than those of the healthy side (P < 0.05). But there was no statistical significance in CBV between the affected side and the healthy side (P > 0.05). The CBF and CBV of the affected side in patients with poor collateral circulation were lower than those of the healthy side, and the MTT and TTP were longer than those of the healthy side (P < 0.05). The incidence rate of severe stenosis or occlusion of responsible vessels in patients with abnormal cerebral tissue blood perfusion indicated by CTPI was higher than that in patients with normal blood perfusion indicated by CTPI (P < 0.05). Conclusion CTPI can timely and accurately reflect the blood perfusion in the infarcted lesion area and ischemic penumbra in patients with acute ischemic stroke. It is helpful for clinically grasping the collateral circulation status, objectively assessing the responsible vessel stenosis degree. -

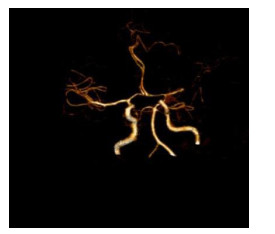
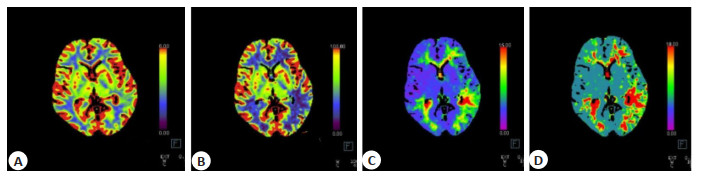
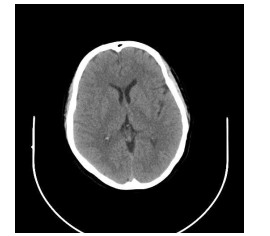
图 3 AIS患者脑部CTP成像
A: L-MCA供血区CBV较对侧略增加; B: L-MCA供血区CBF较对侧降低; C: L-MCA供血区TTP较对侧延长; D: L-MCA供血区MTT较对侧延长.
Figure 3. CTP imaging of patients withAIS.
表 1 CTPI阳性患者患侧梗死病灶区与健侧相应区域CTPI参数比较
Table 1. Comparison of CTPI parameters between the infarcted lesion area of the affected side and the corresponding area of the healthy side in CTPI-positive patients (n=46, Mean±SD)
部位 CBF[mL/(100 g·min)] CBV(mL/100 g) MTT(s) TTP(s) 患侧 23.25±3.46 2.09±0.53 6.03±0.97 16.24±2.08 健侧 45.83±6.59 2.74±0.62 3.39±0.52 12.16±1.47 t 20.575 5.405 16.269 10.864 P < 0.001 < 0.001 < 0.001 < 0.001 CBF: 脑血流量; CBV: 脑血容量; MTT: 平均通过时间; TTP: 峰值时间.  下载: 导出CSV
下载: 导出CSV
表 2 CTPI阳性患者患侧缺血半暗带与健侧相应区域CTPI参数比较
Table 2. Comparison of CTPI parameters between the ischemic penumbra of the affected side and the corresponding area of the healthy side in CTPI-positive patients (n=46, Mean±SD)
部位 CBF[mL/(100 g·min)] CBV(mL/100g) MTT(s) TTP(s) 患侧 32.76±3.15 2.29±0.43 5.74±0.84 15.37±2.43 健侧 47.07±6.84 2.87±0.65 3.48±0.69 11.75±1.56 t 12.888 5.047 11.854 8.502 P < 0.001 < 0.001 < 0.001 < 0.001
下载: 导出CSV
表 3 侧支循环良好者梗死病灶区与健侧CTPI参数比较
Table 3. Comparison of CTPI parameters between infarcted lesion area and healthy side in patients with good collateral circulation (n=20, Mean±SD)
部位 CBF[mL/(100 g·min)] CBV(mL/100 g) MTT(s) TTP(s) 患侧 25.45±1.06 2.49±0.11 5.76±0.31 15.43±1.16 健侧 46.07±5.19 2.62±0.33 3.32±0.37 11.96±1.07 t 17.408 1.671 22.606 12.242 P < 0.001 0.103 < 0.001 < 0.001
下载: 导出CSV
表 4 侧支循环不良者患侧梗死病灶区CTPI参数比较
Table 4. Comparison of CTPI parameters between infarcted lesion area and healthy side in patients with poor collateral circulation (n=31, Mean±SD)
部位 CBF[mL/(100 g·min)] CBV(mL/100 g) MTT(s) TTP(s) 患侧 22.74±2.54 1.97±0.28 6.13±0.52 16.58±1.42 健侧 44.12±3.96 2.89±0.36 3.59±0.24 12.36±1.03 t 25.303 11.231 24.693 13.394 P < 0.001 < 0.001 < 0.001 < 0.001
下载: 导出CSV
表 5 责任血管不同狭窄程度患者CTPI血流灌注情况比较
Table 5. Comparison of CTPI blood perfusion status in patients with different stenosis degrees of responsible vessels [n(%)]
CTPI血流灌注情况 责任血管狭窄程度 轻度狭窄 中度狭窄 重度狭窄或闭塞 血流灌注异常(n=46) 8(63.64) 20(95.45) 18(100.00) 血流灌注正常(n=5) 3(36.36) 2(4.55) 0(0) Z 2.260 P 0.024 CTPI: CT灌注成像.
下载: 导出CSV
-
[1] Seners P, Oppenheim C, Turc G, et al. Perfusion imaging and clinical outcome in acute ischemic stroke with large core[J]. Ann Neurol, 2021, 90(3): 417-27. doi: 10.1002/ana.26152 [2] 周思超. 颅脑CT血管成像对急性缺血性脑卒中患者诊断及预后判断的价值[J]. 中国CT和MRI杂志, 2022, 20(1): 28-31. https://www.cnki.com.cn/Article/CJFDTOTAL-CTMR202201009.htm [3] Stragapede L, Furlanis G, Ajčević M, et al. Brain oscillatory activity and CT perfusion in hyper-acute ischemic stroke[J]. J Clin Neurosci, 2019, 69: 184-9. doi: 10.1016/j.jocn.2019.07.068 [4] 匡祖颖, 向姣, 张新斐, 等. CT灌注成像评价急性缺血性脑卒中患者远隔肢体缺血后适应的价值[J]. 实用医学杂志, 2019, 35(14): 2311-5. doi: 10.3969/j.issn.1006-5725.2019.14.026 [5] Katyal A, Bhaskar SMM. Value of pre-intervention CT perfusion imaging in acute ischemic stroke prognosis[J]. Diagn Interv Radiol, 2021, 27(6): 774-85. doi: 10.5152/dir.2021.20805 [6] Wang K, Li YM, Cheng HY, et al. Perfusion CT detects alterations in local cerebral flow of glioma related to IDH, MGMT and TERT status[J]. BMC Neurol, 2021, 21(1): 460. doi: 10.1186/s12883-021-02490-4 [7] 中华医学会神经病学分会, 中华医学会神经病学分会脑血管病学组, 彭斌, 等. 中国急性缺血性脑卒中诊治指南2018[J]. 中华神经科杂志, 2018, 51(9): 666-82. doi: 10.3760/cma.j.issn.1006-7876.2018.09.004 [8] Hoelter P, Muehlen I, Goelitz P, et al. Automated ASPECT scoring in acute ischemic stroke: comparison of three software tools[J]. Neuroradiology, 2020, 62(10): 1231-8. doi: 10.1007/s00234-020-02439-3 [9] 中华医学会神经病学分会, 中华医学会神经病学分会脑血管病学组. 中国脑血管病影像应用指南[J]. 中华神经科杂志, 2016, 49(3): 164- 81. doi: 10.3760/cma.j.issn.1006-7876.2016.03.002 [10] Bill O, Inácio NM, Lambrou D, et al. Focal hypoperfusion in acute ischemic stroke perfusion CT: clinical and radiologic predictors and accuracy for infarct prediction[J]. AJNR Am J Neuroradiol, 2019, 40 (3): 483-9. [11] Wang Z, Xie J, Tang TY, et al. Collateral status at single-phase and multiphase CT angiography versus CT perfusion for outcome prediction in anterior circulation acute ischemic stroke[J]. Radiology, 2020, 296(2): 393-400. doi: 10.1148/radiol.2020192029 [12] 汪林刚, 冯波, 俞蓉蓉. 全脑CT灌注成像联合头颈部CT血管造影用于急性缺血性脑卒中的诊断价值[J]. 中国基层医药, 2020, 27(4): 408-11. doi: 10.3760/cma.j.issn.1008-6706.2020.04.006 [13] Xu SM, Wang L, Zhao LD. Clinical application value of brain CT perfusion imaging in the treatment of acute ischemic stroke thrombolytic therapy[J]. Exp Ther Med, 2019, 17(5): 3971-6. [14] 李蕾, 李远庆, 迟淑萍, 等. CT灌注成像快速评估脑组织缺血半暗带指导拓宽脑卒中治疗时间窗的可行性研究[J]. 中国医学装备, 2021, 18(3): 76-80. doi: 10.3969/J.ISSN.1672-8270.2021.03.019 [15] 刘姝兰, 宋震宇, 余飞, 等. CT灌注成像与MR灌注成像诊断急性缺血性脑卒中的对比研究[J]. 医学影像学杂志, 2020, 30(8): 1345-8. https://www.cnki.com.cn/Article/CJFDTOTAL-XYXZ202008004.htm [16] 吕沙沙, 曹萌萌. CT血管成像与CT灌注成像对急性缺血性脑卒中的诊断价值分析[J]. 实用放射学杂志, 2020, 36(5): 816-8, 830. doi: 10.3969/j.issn.1002-1671.2020.05.032 [17] 陈聚惠, 苗重昌. 急性缺血性脑卒中侧支循环的影像评估[J]. 国际医学放射学杂志, 2019, 42(3): 303-7. https://www.cnki.com.cn/Article/CJFDTOTAL-GWLC201903012.htm [18] 张为, 李小虎, 吴宗山, 等. 多时相CT血管成像"一站"扫描对急性缺血性脑卒中的价值研究[J]. 安徽医药, 2020, 24(9): 1835-8, 1915. doi: 10.3969/j.issn.1009-6469.2020.09.036 [19] Li GS, Huang R, Bi GR. The impact of FLAIR vascular hyperintensity on clinical severity and outcome: a retrospective study in stroke patients with proximal middle cerebral artery stenosis or occlusion[J]. Neurol Sci, 2021, 42(2): 589-98. [20] Jaiswal SK, Yan FL, Min L. Prevalence of intracranial artery Stenosis in patients with acute ischemic stroke in a tertiary care hospital of China[J]. JNMA J Nepal MedAssoc, 2020, 58(229): 634-9. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 168
- HTML全文浏览量: 99
- PDF下载量: 7
- 被引次数: 0