



CT image prediction of pure ground-glass nodule invasion degree and pathological nature of pulmonary nodules in patients with lung adenocarcinoma
-
摘要:
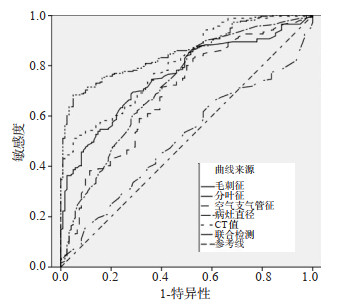
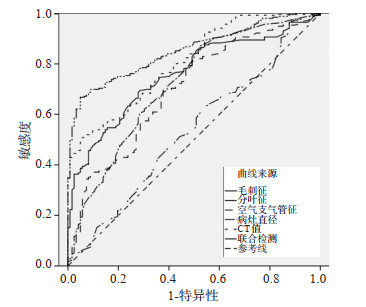
目的 研究肺腺癌患者CT影像对纯磨玻璃结节(PGGN)浸润程度及对肺结节病理性质的预测价值。 方法 采用回顾性研究方法,以我院2017年1月~2021年1月住院治疗的122例PGGN患者作为研究对象。根据肺腺癌的种类分组,其中侵袭前组患者82例原位腺癌(AIS)组患者39例,微浸润性腺癌(MIA)组患者43例,侵袭组患者40例; 根据肺腺癌良恶性分组,其中良性组80例,恶性组42例。比较侵袭前组与侵袭组、AIS组与MIA组以及良性组与恶性组患者的病灶直径、CT值、形状、瘤肺界面、毛刺征、空泡征、三维形状、分叶征、空气支气管征、胸膜凹陷症情况之间的差异。 结果 侵袭前组以及侵袭组患者的病灶直径、CT值、形状、毛刺征、分叶征、空气支气管征情况之间的差异有统计学意义(P < 0.05);AIS以及MIA组患者的分叶征、空泡征、CT值之间的差异有统计学意义(P < 0.05);良性组以及恶性组患者的瘤肺界面、病灶直径、CT值、形状、毛刺征、分叶征、空气支气管征情况之间的差异有统计学意义(P < 0.05);病灶直径、CT值、形状、毛刺征、分叶征、空气支气管征联合检测对肺癌的侵袭以及恶性组患者的诊断敏感度高于单独检测; ROC曲线分析示,病灶直径、CT值、形状、毛刺征、分叶征、空气支气管征联合检测对浸润性以及恶性肿瘤的曲线下面积高于单独检测。 结论 肺腺癌患者CT影像对于PGGN浸润程度及对肺结节病理性质具有显著的预测价值。 Abstract:Objective To explore the predictive value of CT images in the degree of pure ground-glass nodule (PGGN) infiltration and the pathological properties of pulmonary nodules in patients with lung adenocarcinoma. Methods A total of 122 patients with pggn hospitalized in our hospital from January 2017 to January 2021 were selected. According to the types of lung adenocarcinoma, 82 patients in the pre invasion group [39 patients in adenocarcinoma in situ (AIS) group and 43 patients in microinvasive adenocarcinoma (MIA) group] and 40 patients in the invasion group. According to the classification of benign and malignant lung adenocarcinoma, there were 80 cases in benign group and 42 cases in malignant group. We compared the differences of lesion diameter, CT value, shape, tumor lung interface, hairpin sign, vacuole sign, three-dimensional shape, lobulation sign, air bronchus sign and pleural indentation between the pre invasion group and the invasion group, AIS group and MIA group, benign group and malignant group. Results The differences of lesion diameter, CT value, shape, burr sign, lobulation sign and air bronchogram sign between the pre invasion group and the invasion group were significant (P < 0.05). The differences of lobation sign, vacuole sign and CT value between AIS and MIA groups were statistically significant (P < 0.05). The differences of tumor lung interface, lesion diameter, CT value, shape, burr sign, lobulation sign and air bronchial sign between benign group and malignant group were significant (P < 0.05). The diagnostic sensitivity of combined detection of lesion diameter, CT value, shape, burr sign, lobulation sign and air bronchogram sign in patients with lung cancer invasion and malignant group was significantly higher than that of single detection. ROC curve analysis showed that the area under the curve of the combined detection of lesion diameter, CT value, shape, burr sign, lobulation sign and air bronchial sign were significantly higher than that of the single detection. Conclusion CT images of patients with lung adenocarcinoma have significant predictive value for the degree of PGGN infiltration and the pathological properties of pulmonary nodules. -
Key words:
- CT /
- pulmonary ground glass nodules /
- invasive /
- pathological properties /
- CT value
-

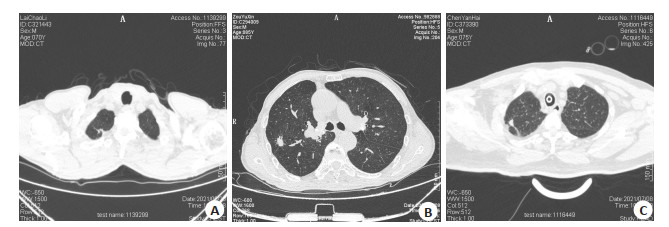
图 1 肺腺癌的影像学特征
A: 右肺上叶原位癌; B: 右肺上叶浸润癌; C: 右肺上叶微浸润癌.
Figure 1. Imaging features of lung adenocarcinoma.
表 1 两组患者的一般资料比较
Table 1. Comparison of general data between the two groups
分组 性别(男/女, n) BMI(kg/m2, Mean±SD) 年龄(岁, Mean±SD) 侵袭前组(n=82) 40/42 24.33±2.32 55.74±2.85 侵袭组(n=40) 26/14 24.76±2.24 55.53±3.48 t/χ2 1.159 0.492 0.334 P 0.560 0.624 0.739  下载: 导出CSV
下载: 导出CSV
表 2 两组患者的影像学特征分析
Table 2. Imaging characteristics of the two groups of patients [n(%)]
CT征象 侵袭前组(n=82) 侵袭组(n=40) χ2 P 瘤肺界面 0.371 0.545 清晰 73(89.02) 37(92.50) 模糊 9(10.98) 3(7.50) 毛刺征 21.292 < 0.001 有 6(7.32) 20(50.00) 无 76(92.68) 20(50.00) 空泡征 2.481 0.116 有 8(9.76) 8(20.00) 无 74(90.24) 32(80.00) 三维形状 0.061 0.812 球体 11(13.41) 6(15.00) 非球体 71(86.59) 34(85.00) 分叶征 37.171 < 0.001 有 20(24.39) 31(77.50) 无 62(75.61) 9(22.50) 空气支气管征 17.191 < 0.001 有 6(7.32) 15(37.50) 无 76(92.68) 25(62.50) 胸膜凹陷症 0.002 0.943 有 16(19.51) 8(20.00) 无 66(80.49) 32(80.00) 病灶直径(cm, Mean±SD) 1.03±0.24 1.41±0.21 8.944 < 0.001 CT值(Hu, Mean±SD) 240.76±5.47 320.25±5.99 70.762 < 0.001
下载: 导出CSV
表 3 AIS以及MIA组患者的影像学特征分析
Table 3. Imaging characteristics of patients in the AIS and MIA groups [n(%)]
CT征象 AIS组(n=39) MIA组(n=43) χ2 P 瘤肺界面 1.481 0.224 清晰 33(45.21) 40(54.79) 模糊 6(66.67) 3(33.33) 毛刺征 0.021 0.901 有 3(50.00) 3(50.00) 无 36(47.37) 40(52.63) 空泡征 4.371 0.037 有 1(12.50) 7(87.50) 无 38(51.35) 36(48.65) 三维形状 0.021 0.881 球体 5(45.45) 6(54.55) 非球体 34(47.89) 37(52.11) 分叶征 5.401 0.020 有 5(25.00) 15(75.00) 无 34(54.84) 28(45.16) 空气支气管征 0.532 0.469 有 2(33.33) 4(66.67) 无 37(48.68) 39(51.32) 胸膜凹陷症 0.122 0.734 有 7(43.75) 9(56.25) 无 32(48.48) 34(51.52) 病灶直径(cm, Mean±SD) 1.01±0.19 1.07±0.17 1.501 0.137 CT值(Hu, Mean±SD) 220.56±6.01 282.17±6.79 43.583 < 0.001 AIS: 原位腺癌; MIA: 微浸润性腺癌.
下载: 导出CSV
表 4 不同病理情况患者的影像学特征分析
Table 4. Imaging characteristics of patients with different pathological conditions [n (%
CT征象 良性组(n=80) 恶性组(n=42) χ2 P 瘤肺界面 6.612 < 0.001 清晰 79(71.82) 31(28.18) 模糊 1(8.33) 11(91.67) 毛刺征 5.312 0.021 有 5.312 4(15.38) 无 58(60.42) 38(39.58) 空泡征 1.981 0.160 有 8(50.00) 8(50.00) 无 72(67.92) 34(32.08) 三维形状 0.221 0.639 球体 12(70.59) 5(29.41) 非球体 68(64.76) 37(35.24) 分叶征 8.521 0.004 有 41(80.39) 10(19.61) 无 39(54.93) 32(45.07) 空气支气管征 4.558 0.033 有 18(85.71) 3(14.29) 无 62(61.39) 39(38.61) 胸膜凹陷症 3.212 0.073 有 12(50.00) 12(50.00) 无 68(69.39) 30(30.61) 病灶直径(cm, Mean±SD) 1.44±0.19 0.60±0.12 29.808 < 0.001 CT值(Hu, Mean±SD) 289.63±6.97 223.37±7.85 46.004 < 0.001
下载: 导出CSV
表 5 联合检测效能分析
Table 5. Joint detection efficiency analysis
诊断方法 真阳例数(n) 假阳例数(n) 真阴例数(n) 假阴例数(n) 准确率(%) 敏感度(%) 特异性(%) 阳性预测值(%) 阴性预测值(%) 侵袭 毛刺征 15 51 31 25 37.70 37.50 37.80 22.73 55.36 分叶征 14 55 27 26 33.61 35.00 32.93 20.29 50.94 空气支气管征 11 52 30 29 33.61 27.50 36.59 17.46 50.85 病灶直径 12 45 37 28 40.16 30.00 45.12 21.05 56.92 CT值 16 21 61 24 63.11 40.00 74.39 43.24 71.76 联合检测 35 30 52 5 71.31 87.50 63.41 53.85 91.23 恶性 毛刺征 11 55 25 31 29.51 26.19 31.25 16.67 44.64 分叶征 12 49 31 30 35.25 28.57 38.75 19.67 50.82 空气支气管征 10 48 32 32 34.43 23.81 40.00 17.24 50.00 病灶直径 11 47 33 31 36.07 26.19 41.25 18.97 51.56 CT值 15 41 39 27 44.26 35.71 48.75 26.79 59.09 联合检测 30 35 45 12 61.48 71.43 56.25 46.15 78.95
下载: 导出CSV
表 6 ROC曲线分析
Table 6. ROC curve analysis
诊断方法 标准误 AUC AUC(95% CI) P 恶性 毛刺征 11.231 0.775 0.520~0.872 < 0.001 分叶征 12.564 0.552 0.412~0.599 < 0.001 空气支气管征 9.885 0.415 0.332~0.985 < 0.001 病灶直径 10.635 0.552 0.322~0.785 < 0.001 CT值 8.754 0.523 0.123~0.663 < 0.001 联合检测 9.252 0.803 0.600~0.946 < 0.001 浸润 毛刺征 12.362 0.632 0.441~0.965 < 0.001 分叶征 11.584 0.523 0.321~0.577 < 0.001 空气支气管征 10.522 0.417 0.210~0.995 < 0.001 病灶直径 9.882 0.332 0.222~0.587 < 0.001 CT值 9.852 0.775 0.296~0.779 < 0.001 联合检测 7.889 0.889 0.521~0.936 < 0.001
下载: 导出CSV
-
[1] 张磊, 谢晓东, 沈文荣, 等. CT征象在预测肺纯磨玻璃结节侵袭风险中的价值[J]. 实用放射学杂志, 2020, 36(2): 207-10, 213. doi: 10.3969/j.issn.1002-1671.2020.02.009 [2] 余烨, 张莹, 张凤, 等. CT征象对pGGN样肺腺癌浸润性的诊断价值[J]. 国际医学放射学杂志, 2020, 43(6): 639-43. doi: 10.19300/j.2020.L18025 [3] 汪琼, 伍建林. 基于长期CT随访的肺纯磨玻璃结节演变规律及其危险因素[J]. 放射学实践, 2022, 37(3): 398-401. https://www.cnki.com.cn/Article/CJFDTOTAL-FSXS202203024.htm [4] 刘强, 娄豪, 陈德一, 等. 肺肿瘤性磨玻璃结节平均CT值测量相关技术的影响因素研究[J]. 重庆医学, 2021, 50(20): 3482-6. doi: 10.3969/j.issn.1671-8348.2021.20.014 [5] 车思雨, 蒋依宁, 韩广庆, 等. 基于CT图像的神经网络模型鉴别纯磨玻璃样微浸润性腺癌和浸润性腺癌[J]. 实用医学杂志, 2020, 36 (23): 3273-8. doi: 10.3969/j.issn.1006-5725.2020.23.022 [6] 武卫杰, 岳松伟, 王会霞, 等. 能谱CT虚拟平扫评估肺纯磨玻璃结节的可行性研究[J]. 放射学实践, 2020, 35(3): 346-51. doi: 10.13609/j.cnki.1000-0313.2020.03.018 [7] 李鲁, 舒锦尔, 陈真伟, 等. 磨玻璃结节表现的肺腺癌侵犯脏层胸膜的超高分辨率CT评价[J]. 中国医学计算机成像杂志, 2020, 26(3): 223-9. doi: 10.3969/j.issn.1006-5741.2020.03.006 [8] 周丽娜, 吴宁, 赵世俊, 等. 基于高分辨率CT特征鉴别同时多原发肺腺癌与肺腺癌伴肺内转移[J]. 中华肿瘤杂志, 2020, 42(6): 449-55. doi: 10.3760/cma.j.cn112152-20200227-00126 [9] 李敏, 王娅菲, 姜文蓁, 等. 双层探测器光谱CT平扫定性联合定量参数预测肺纯磨玻璃结节侵袭性的价值[J]. 中华放射学杂志, 2022, 56 (3): 248-53. [10] Chu ZG, Li WJ, Fu BJ, et al. CT characteristics for predicting invasiveness in pulmonary pure ground-glass nodules[J]. AJR Am J Roentgenol, 2020, 215(2): 351-8. doi: 10.2214/AJR.19.22381 [11] Qiu TC, Ru XS, Yin K, et al. Two nomograms based on CT features to predict tumor invasiveness of pulmonary adenocarcinoma and growth in pure GGN: a retrospective analysis[J]. Jpn J Radiol, 2020, 38(8): 761-70. doi: 10.1007/s11604-020-00957-x [12] Zhao MM, Deng JJ, Wang TT, et al. Impact of computed tomography window settings on clinical T classifications and prognostic evaluation of patients with subsolid nodules[J]. Eur J Cardiothorac Surg, 2020, 59(6): 1295-303. [13] Sun YL, Li C, Jin L, et al. Radiomics for lung adenocarcinoma manifesting as pure ground-glass nodules: invasive prediction[J]. Eur Radiol, 2020, 30(7): 3650-9. doi: 10.1007/s00330-020-06776-y [14] Zhang T, Pu XH, Yuan M, et al. Histogram analysis combined with morphological characteristics to discriminate adenocarcinoma in situ or minimally invasive adenocarcinoma from invasive adenocarcinoma appearing as pure ground- glass nodule[J]. Eur J Radiol, 2019, 113: 238-44. [15] Yang Y, Wang WW, Ren Y, et al. Computerized texture analysis predicts histological invasiveness within lung adenocarcinoma manifesting as pure ground-glass nodules[J]. Acta Radiol, 2019, 60 (10): 1258-64. [16] 韩旭健, 李振家, 窦卫涛, 等. CT引导下肺小结节(≤1.5cm)穿刺活检结果研究[J]. 医学影像学杂志, 2018, 28(2): 229-32. https://www.cnki.com.cn/Article/CJFDTOTAL-XYXZ201802018.htm [17] 杨文魁, 周志刚, 张琼, 等. CT影像特征及定量参数对肺腺癌纯磨玻璃结节侵袭性的评估价值[J]. 现代临床医学, 2021, 47(6): 412-5. https://www.cnki.com.cn/Article/CJFDTOTAL-YYCD202106004.htm [18] Yang HH, Lv YL, Fan XH, et al. Factors distinguishing invasive from pre-invasive adenocarcinoma presenting as pure ground glass pulmonary nodules[J]. Radiat Oncol, 2020, 15(1): 186. [19] Ko KH, Huang TW, Chang WC, et al. Differentiating focal interstitial fibrosis from adenocarcinoma in persistent pulmonary subsolid nodules (>5 mm and < 20 mm): the role of coronal thin-section CT images[J]. Eur Radiol, 2021, 31(11): 8326-34. [20] Kim YW, Kwon BS, Lim SY, et al. Lung cancer probability and clinical outcomes of baseline and new subsolid nodules detected on low-dose CT screening[J]. Thorax, 2021, 76(10): 980-8. [21] 辛玉静, 刘青, 童卫玲, 等. 肺腺癌的CT征象及病理分析[J]. 实用医学影像杂志, 2020, 21(5): 473-6. https://www.cnki.com.cn/Article/CJFDTOTAL-SYXY202005011.htm -

 点击查看大图
点击查看大图
计量
- 文章访问数: 188
- HTML全文浏览量: 54
- PDF下载量: 10
- 被引次数: 0