



Logistic regression analysis of correlation between ultrasonic signs and expression of multiple immunohistochemical factors in 524 cases of invasive ductal carcinoma of breast
-
摘要:
目的 探索乳腺浸润性导管癌超声征象与多种免疫组化因子表达的相关性。 方法 回顾性分析我院2019年1月~2021年12月经手术病理证实为乳腺原发性浸润性导管癌患者524例,术前进行超声检查并留存有标准的超声声像图,采用单因素分析χ2检验和二元Logistic回归分析超声声像图征象与雌激素受体(ER)、孕激素受体(PR)、人类表皮因子受体2(HER-2)、P53、细胞核增殖因子Ki-67、DNA拓扑异构酶IIa(TOPIIa)、细胞角蛋白CK5/6免疫组化因子表达的相关性,并构建Logistic回归方程。 结果 Logistic回归分析发现ER的阳性表达与肿块形状、肿块边缘、后方回声、高回声晕、血供丰富之间存在相关性(P < 0.05);PR的阳性表达与肿块边缘、高回声晕、直径 > 2 cm存在相关性;HER-2的阳性表达与内部微钙化、纵横比 > 1之间存在相关性(P < 0.05);Ki-67的高表达与淋巴结转移、后方回声减低之间存在相关性(P < 0.05);P53的阳性表达与内部钙化、淋巴结转移、肿块形状、高回声晕之间存在相关性(P < 0.05);CK5/6的阳性表达与内部微钙化和高回声晕之间存在相关性(P < 0.05);TOPIIa的阳性表达与淋巴结转移、后方回声、肿块直径 > 2 cm存在相关性(P < 0.05),得出相应的回归方程并以ROC曲线检验方程效能。 结论 不同免疫组化表达的浸润性导管癌的征象具有一定的差异,这些超声征象可为乳腺癌的诊断、临床治疗和预后评估提供重要参考依据。 -
关键词:
- 浸润性导管癌 /
- 超声征象 /
- Logistic回归方程
Abstract:Objective To explore the correlation between ultrasonographic signs of invasive ductal carcinoma of breast and the expression of immunohistochemical factors. Methods We retrospectively analyzed 524 patients with primary invasive ductal carcinoma of breast confirmed by surgical pathology in our hospital from January 2019 to December 2021. Preoperative ultrasound examination was performed and standard ultrasound images were retained. Univariate analysis χ2 test and binary logistic regression were used to analyze the correlation between ultrasonographic signs and the expression of ER, PR, HER-2, P53, Ki-67, TOPIIa and CK5/6 immunohistochemical factors. The logistic regression equation was established. Results Logistic regression analysis showed that positive expression of ER was correlated with tumor shape, tumor margin, posterior echo, hyperecho halo and abundant blood supply (P < 0.05). The positive expression of PR was associated with tumor margin, hyperechoic halo, diameter > 2 cm. Positive HER-2 expression and internal microcalcification, aspect ratio diameter greater than 1 (P < 0.05). The high expression of Ki-67 was correlated with lymph node metastasis and posteriorechogenicity (P < 0.05). The positive expression of P53 was correlated with internal calcification, lymph node metastasis, tumor shape and hyperechoic halo (P < 0.05). The positive expression of CK5/6 was correlated with internal microcalcification and hyperechoic halo (P < 0.05). The positive expression of TOPIIa was associated with lymph node metastasis, posterior echo, and tumor diameter > 2 cm (P < 0.05). The corresponding regression equation was obtained and ROC curve was used to test the efficiency of the equation. Conclusion There are some differences in the signs of invasive ductal carcinoma with different immunohistochemical expressions. These ultrasound signs can provide important reference for the diagnosis, clinical treatment and prognosis assessment of breast cancer, and further link imaging and pathology together. -

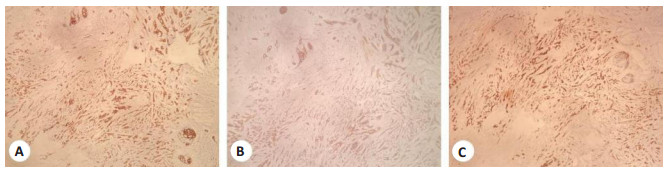
图 1 免疫组化染色
Figure 1. Immunohistochemical staining (Original magnification: × 40).
A: ER; B: HER-2; C: PR.

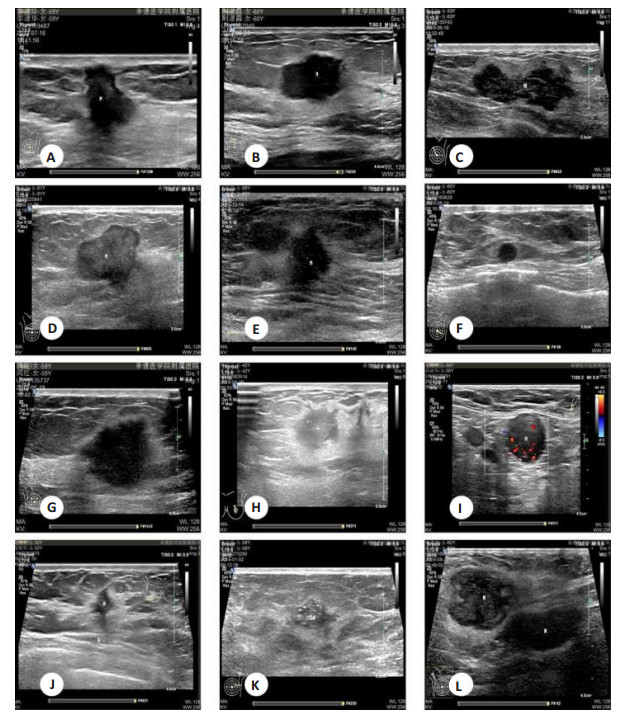
图 2 浸润性导管癌超声声像图征象
A: 肿块后方回声减低; B: 肿块后方回声增强; C: 肿块后方回声无变化; D: 肿块边缘光整; E: 肿块边缘毛刺成角; F: 肿块形态规则; G: 肿块形态不规则; H: 肿块高回声晕; I: 肿块血供丰富; J: 肿块纵横比 > 1; K: 肿块内部微钙化; L: 淋巴结转移.
Figure 2. The ultrasonographic appearance of an infiltrating ductal carcinoma.
表 1 组间免疫组化表达结果
Table 1. Immunohistochemical expression results between groups (n)
免疫组化 阳性 阴性 ER 379 145 PR 323 201 HER-2 190 334 Ki-67 454 70 P53 191 333 TOPIIa 387 137 CK5/6 154 370 ER: 雌激素受体; PR: 孕激素受体; HER-2: 人类表皮因子受体2; TOPIIa: DNA拓扑异构酶IIa.  下载: 导出CSV
下载: 导出CSV
表 2 ER、PR的表达与超声征象之间的联系
Table 2. Relationship between the expression of ER and PR and ultrasonic signs (n)
超声特点 ER PR 阳性 阴性 χ2 P 阳性 阴性 χ2 P 边缘 61.914 < 0.001 37.722 < 0.001 毛刺成角 358 100 305 153 光整 21 45 18 48 形状 25.404 < 0.001 7.160 0.007 不规则 265 67 219 113 规则 114 78 104 88 后方回声 56.596 < 0.001 28.382 < 0.001 减低 175 24 148 51 无变化 131 51 109 73 增强 71 70 66 77 微钙化 11.233 0.001 5.425 0.020 有 243 112 201 145 无 145 33 122 56 高回声晕 157.41 < 0.001 98.185 < 0.001 有 334 49 285 98 无 45 96 38 103 血流 5.776 0.016 1.103 0.294 丰富 207 96 181 122 不丰富 172 49 142 79 淋巴结 0.031 0.859 0.007 0.935 转移 151 59 129 81 未转移 228 86 194 120 纵横比 4.108 0.128 2.619 0.270 > 1 192 60 164 89 < 1 186 85 159 112 最大直径(cm) 6.690 0.010 8.772 0.003 > 2 209 98 173 134 < 2 170 47 150 67
下载: 导出CSV
表 3 P53、Ki-67的表达与超声征象之间的联系
Table 3. Association between expression of P53, Ki-67 and ultrasonic signs (n)
超声特点 P53 Ki-67 阳性 阴性 χ2 P 阳性 阴性 χ2 P 边缘 8.961 0.003 3.475 0.062 毛刺成角 156 302 392 66 光整 35 31 62 4 形状 15.673 < 0.001 1.535 0.215 不规则 100 232 283 49 规则 91 101 171 21 后方回声 11.899 0.003 20.488 < 0.001 减低 65 134 156 43 无变化 57 125 163 19 增强 69 74 135 8 微钙化 16.106 < 0.001 7.680 0.006 有 147 199 310 36 无 44 134 144 34 高回声晕 31.921 < 0.001 6.545 0.011 有 112 271 323 60 无 79 62 131 10 血流 1.928 0.165 2.028 0.154 丰富 118 185 268 35 不丰富 73 148 186 35 淋巴结 7.167 0.007 6.939 0.008 转移 91 119 192 18 未转移 100 214 262 52 纵横比 6.188 0.045 0.677 0.411 > 1 79 174 216 37 < 1 112 159 218 33 最大直径(cm) 5.825 0.016 13.342 < 0.001 > 2 125 182 280 27 < 2 66 151 174 43
下载: 导出CSV
表 4 TOPIIa与CK5/6的表达与超声征象之间的联系
Table 4. Association between expression of TOPIIa and CK5/6 and ultrasound signs (n)
超声特点 TOPIIa CK5/6 阳性 阴性 χ2 P 阳性 阴性 χ2 P 边缘 6.119 0.013 3.642 0.056 毛刺成角 330 128 128 330 光整 57 9 26 40 形状 4.428 0.035 2.272 0.123 不规则 235 97 90 242 规则 152 40 64 128 后方回声 24.692 < 0.001 0.845 0.655 减低 124 75 54 145 无变化 141 41 55 127 增强 122 21 45 98 微钙化 10.534 0.001 7.267 0.007 有 271 75 115 231 无 116 62 39 139 高回声晕 5.931 0.015 11.322 0.001 有 272 111 97 286 无 115 26 57 84 血流 2.112 0.146 0.588 0.443 丰富 231 72 93 210 不丰富 156 65 61 160 淋巴结 9.140 0.002 0.283 0.595 转移 170 40 59 151 未转移 217 97 95 219 纵横比 1.859 0.173 3.223 0.073 > 1 180 73 65 188 < 1 207 64 89 182 最大直径(cm) 15.119 < 0.001 0.292 0.589 > 2 246 61 93 214 < 2 141 76 61 156
下载: 导出CSV
表 5 HER-2的表达与超声征象之间的联系
Table 5. Association between expression of Her-2 and ultrasound signs (n)
超声特点 HER-2 阳性 阴性 χ2 P 边缘 0.644 0.422 毛刺成角 169 289 光整 21 45 形状 1.123 0.289 不规则 126 206 规则 64 128 后方回声 2.981 0.225 减低 63 136 无变化 72 110 增强 55 88 微钙化 49.157 <0.001 有 162 184 无 28 150 高回声晕 5.919 0.015 有 127 256 无 63 78 血流 2.095 0.148 丰富 102 201 不丰富 88 133 淋巴结 4.051 0.044 转移 87 123 未转移 103 211 纵横比 9.263 0.002 > 1 75 178 < 1 115 156 最大直径(cm) 11.880 0.001 > 2 130 177 < 2 60 157
下载: 导出CSV
表 6 ER表达与超声征象的多因素Logistic回归分析
Table 6. Multiple Logistic regression analysis of ER expression and ultrasonic signs
超声征象 回归系数 标准误 Wald P OR 95% CI 形状不规则 0.653 0.266 6.013 0.014 1.921 1.140~3.236 后方回声减低 0.950 0.332 8.185 0.004 2.586 1.349~4.957 边缘光整 -1.287 0.357 13.003 < 0.001 0.276 0.137~0.556 高回声晕 2.512 0.264 90.548 < 0.001 12.324 7.346~20.673 血流丰富 -0.700 0.267 6.891 0.009 0.497 0.294~0.837
下载: 导出CSV
表 7 PR表达与超声征象的多因素Logistic回归分析
Table 7. Multivariate Logistic regression analysis of PR expression and ultrasonic signs
超声征象 回归系数 标准误 Wald P OR 95% CI 肿块直径 > 2 cm -0.592 0.212 7.762 0.005 0.553 0.365~0.839 边缘光整 -1.143 0.323 12.485 < 0.001 0.319 0.169~0.601 高回声晕 1.948 0.232 70.507 < 0.001 7.015 4.452~11.053
下载: 导出CSV
表 8 P53表达与超声征象的多因素Logistic回归分析
Table 8. Multivariate Logistic regression analysis of P53 expression and ultrasonic signs
超声征象 回归系数 标准误 Wald P OR 95% CI 形状不规则 -0.671 0.199 11.367 0.001 0.511 0.346~0.755 高回声晕 -1.117 0.212 27.868 < 0.001 0.327 0.216~0.495 淋巴结转移 0.565 0.199 8.054 0.005 1.760 1.191~2.599 钙化 0.632 0.216 8.544 0.003 1.881 1.231~2.874
下载: 导出CSV
表 9 Ki-67表达与超声征象的多因素Logistic回归分析
Table 9. Multivariate Logistic regression analysis of Ki-67 expression and ultrasonic signs
超声征象 回归系数 标准误 Wald P OR 95% CI 淋巴结转移 0.847 0.296 8.182 0.004 2.333 1.306~4.170 后方回声减低 -1.597 0.406 15.499 < 0.001 0.203 0.091~0.448
下载: 导出CSV
表 10 HER-2表达与超声征象的多因素Logistic回归分析
Table 10. Multivariate Logistic regression analysis of HER-2 expression and ultrasonic signs
超声征象 回归系数 标准误 Wald P OR 95% CI 钙化 1.509 0.234 41.734 0.000 4.522 2.861~7.147 纵横比 > 1 -0.447 0.193 5.350 0.021 0.639 0.438~0.934
下载: 导出CSV
表 11 TOPIIa表达与超声征象的多因素Logistic回归分析
Table 11. Multivariate Logistic regression analysis of TOPIIa expression and ultrasonic signs
超声征象 回归系数 标准误 Wald P OR 95% CI 淋巴结转移 0.651 0.224 8.454 0.004 1.917 1.236~2.973 后方回声减低 -1.166 0.288 16.409 0.000 0.312 0.177~0.548 肿块直径 > 2 cm 0.575 0.214 7.220 0.007 1.777 1.168~2.704
下载: 导出CSV
表 12 CK5/6表达与超声征象的多因素Logistic回归分析
Table 12. Multivariate Logistic regression analysis of CK5/6 expression and ultrasonic signs
超声征象 回归系数 标准误 Wald P OR 95% CI 钙化 0.536 0.216 6.153 0.013 1.710 1.119~2.612 高回声晕 -0.662 0.209 9.998 0.002 0.516 0.342~0.777
下载: 导出CSV
-
[1] Zujewski JA, Dvaladze AL, Ilbawi A, et al. Knowledge summaries for comprehensive breast cancer control[J]. J Glob Oncol, 2018, 4: 1-7. [2] Ali Y, Hamid SA. Human topoisomerase Ⅱ alpha as a prognostic biomarker in cancer chemotherapy[J]. Tumor Biol, 2016, 37(1): 47-55. doi: 10.1007/s13277-015-4270-9 [3] 时兆婷, 李佳伟, 盛丹丽, 等. 浸润性乳腺癌的超声影像学特征对分子亚型的预测价值[J]. 中华超声影像学杂志, 2021, 30(12): 1064-70. doi: 10.3760/cma.j.cn131148-20210509-00316 [4] Adler DD, Carson PL, Rubin JM, et al. Doppler ultrasound color flow imaging in the study of breast cancer: preliminary findings[J]. Ultrasound Med Biol, 1990, 16(6): 553-9. doi: 10.1016/0301-5629(90)90020-D [5] Stavros AT. 乳腺超声经典诊断学. 中文翻译版[M]. 北京: 科学出版社, 2017. [6] Reinert T, de Paula B, Shafaee MN, et al. Endocrine therapy for ER-positive/HER2-negative metastatic breast cancer[J]. Chin Clin Oncol, 2018, 7(3): 25. doi: 10.21037/cco.2018.06.06 [7] Bansal C, Sharma A, Pujani M, et al. Correlation of hormone receptor and human epidermal growth factor Receptor-2/neu expression in breast cancer with various clinicopathologic factors[J]. Indian J Med Paediatr Oncol, 2017, 38(4): 483. doi: 10.4103/ijmpo.ijmpo_98_16 [8] Penault-Llorca F, Radosevic-Robin N. Ki67 assessment in breast cancer: an update[J]. Pathology, 2017, 49(2): 166-71. doi: 10.1016/j.pathol.2016.11.006 [9] 帅萍. 乳腺癌组织中HER2和Topo Ⅱα的表达及其临床意义[J]. 中南大学学报(医学版), 2016, 41(11): 1143-7. doi: 10.11817/j.issn.1672-7347.2016.11.005 [10] Delgado JL, Hsieh CM, Chan NL, et al. Topoisomerases as anticancer targets[J]. Biochem J, 2018, 475(2): 373-98. doi: 10.1042/BCJ20160583 [11] Fadare O, Wang SA, Hileeto D. The expression of cytokeratin 5/6 in invasive lobular carcinoma of the breast: evidence of a "basal-like" subset?[J]. Hum Pathol, 2008, 39(3): 331-6. doi: 10.1016/j.humpath.2007.07.014 [12] 曾红艳, 曹永政, 彭格红, 等. 乳腺癌超声征象与ER、PR、C-erbB-2表达的相关性研究[J]. 中国医学影像技术, 2007, 23(12): 1827-30. doi: 10.3321/j.issn:1003-3289.2007.12.021 [13] 郑伟伟, 佘铜生, 杨杰, 等. 乳腺浸润性导管癌直接超声征象与ER、PR表达之间的关系分析[J]. 检验医学与临床, 2018, 15(14): 2058-60, 2064. doi: 10.3969/j.issn.1672-9455.2018.14.010 [14] 陈燕, 张江宇, 王丽敏, 等. 非特殊型浸润性乳腺癌超声征象与分子生物学指标关系分析[J]. 广东医学, 2019, 40(11): 1579-83. doi: 10.13820/j.cnki.gdyx.20191080 [15] 唐恩红, 杨少玲, 王凤翎, 等. 分子亚型乳腺癌的超声特征对照研究[J]. 中国超声医学杂志, 2022, 38(1): 22-5. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGCY202201006.htm [16] 朱萍, 刘俊, 梁喜. 绝经前后三阴性乳腺癌超声特征的对比研究[J]. 临床超声医学杂志, 2021, 23(9): 711-3. doi: 10.3969/j.issn.1008-6978.2021.09.023 [17] 张瑾晖, 王丹, 姜珏, 等. 非特殊型浸润性乳腺癌声像图特征与P53表达的相关性分析[J]. 中国超声医学杂志, 2021, 37(8): 862-5. doi: 10.3969/j.issn.1002-0101.2021.08.007 [18] 毛羡仪, 梁伟翔, 蒋殿虎, 等. 乳腺癌高回声晕超声特征与ER、PR表达水平的相关性分析[J]. 医学影像学杂志, 2020, 30(6): 1001-4, 1013. https://www.cnki.com.cn/Article/CJFDTOTAL-XYXZ202006022.htm [19] 李晶, 姜罗, 史铁梅. 乳腺癌超声恶性晕病理基础[J]. 中华超声影像学杂志, 2012, 21(9): 787-90. doi: 10.3760/cma.j.issn.1004-4477.2012.09.017 [20] 曹长军, 陈东风, 何敬海, 等. 乳腺癌超声影像学表现与分子生物学相关性研究[J]. 中国全科医学, 2011, 14(30): 3435-8, 3441. doi: 10.3969/j.issn.1007-9572.2011.30.005 [21] Cha H, Chang YW, Lee EJ, et al. Ultrasonographic features of pure ductal carcinoma in situ of the breast: correlations with pathologic features and biological markers[J]. Ultrasonography, 2018, 37(4): 307-14. doi: 10.14366/usg.17039 [22] Pang JMB, Byrne DJ, Takano EA, et al. Breast tissue composition and immunophenotype and its relationship with mammographic density in women at high risk of breast cancer[J]. PLoS One, 2015, 10(6): e0128861. doi: 10.1371/journal.pone.0128861 [23] 王冠朝. 乳腺癌超声征象与雌激素受体、孕激素受体及C-erbB-2表达的相关性分析[J]. 癌症进展, 2021, 19(16): 1651-4. https://www.cnki.com.cn/Article/CJFDTOTAL-AZJZ202116010.htm [24] 李宏, 李德华, 胡波. 乳腺癌超声征象与Ki67、p53表达的相关性及临床意义[J]. 中国临床医学影像杂志, 2015, 26(5): 321-4. https://www.cnki.com.cn/Article/CJFDTOTAL-LYYX201505009.htm [25] 邹璐璐, 周军. 乳腺肿瘤血供的超声评价方法及研究进展[J]. 中国医学影像学杂志, 2013, 21(10): 795-7. doi: 10.3969/j.issn.1005-5185.2013.10.021 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 241
- HTML全文浏览量: 85
- PDF下载量: 4
- 被引次数: 0