



Monitoring value of MRI in the diagnosis and treatment of growth hormone deficiency in children
-
摘要:
目的 探究MRI对生长激素缺乏症患儿的诊断及治疗的监测价值。 方法 回顾性分析2018年1月~2019年4月本院就诊的100例生长激素缺乏症患者的临床资料,比较患者的血清生长激素水平,采用8通道颅脑线圈对所有患者进行核磁共振平面扫描,比较分析患者治疗前后垂体MRI图像变化。 结果 在100例生长激素缺乏症患者中,45例患者生长激素峰值低于5~10 μg/L,55例生长激素峰值在5 μg/L以下。100例生长激素缺乏症的患者垂体病变以垂体前叶发育不良为主,共42例(42%),再者是垂体柄中断综合征25例(25%);空蝶鞍综合征14例(14%),郎格汉斯细胞组织增多症侵袭垂体12例(12%)以及颅咽管瘤7例(7%)。生长激素缺乏症的患儿垂体的矢状高径、矢状后径等指标大于正常儿童,且差异具有统计学意义(P < 0.05),经生长激素替代治疗后,各个年龄的垂体都有不同程度的变小,其中以3~10岁和11~16岁的变化更加显著(P < 0.05)。 结论 MRI能够准确发现由于垂体病变导致的生长激素缺乏症,同时也能准确的监测生长激素替代治疗后垂体大小的改变。 Abstract:Objective To explore the monitoring value of MRI in the diagnosis and treatment of growth hormone deficiency in children. Methods We retrospectively analyzed the clinical data of 100 patients with growth hormone deficiency in our hospital from January 2018 to April 2019. The serum growth hormone levels of all patients were analyzed. The changes of pituitary MRI images before and after treatment were compared. Results Among the 100 cases of growth hormone deficiency, 45 cases had the peak value of growth hormone less than 5-10 μg/L and 55 cases had the peak value of growth hormone less than 5 μg/L. In the 100 patients with growth hormone deficiency, the main pituitary lesion was anterior pituitary dysplasia (n= 42, 42%), and pituitary stalk interrupt syndrome (n=25, 25%). In addition, 14 cases of empty sella syndrome (14%), long disease of grow in quantity of Hans cells invasive pituitary 12 cases (12%) and 7 cases of craniopharyngioma (7%). Children with growth hormone deficiency of pituitary high sagittal diameter, sagittal diameter after index greater than normal children, and the difference was statistically significant (P < 0.05). After growth hormone replacement therapy, The pituitary gland was smaller in different degrees at all ages, and the change was more significant at 3 - 10 years old and 11 - 16 years old (P < 0.05). Conclusion MRI can accurately detect growth hormone deficiency caused by pituitary disease, and can also accurately monitor the change of pituitary size after growth hormone replacement therapy. -

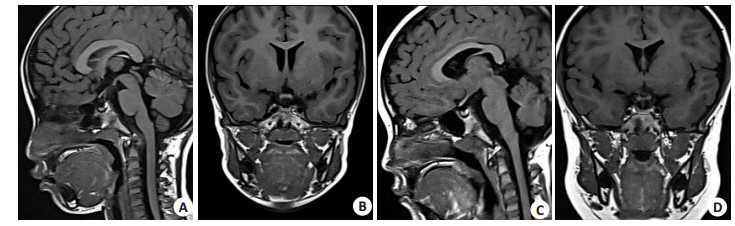
图 1 垂体前叶发育不良影像学特征
A: 生长激素缺乏症患儿矢状位图; B: 生长激素缺乏症患儿冠状位图.
Figure 1. Imaging features of anterior pituitary hypoplasia.

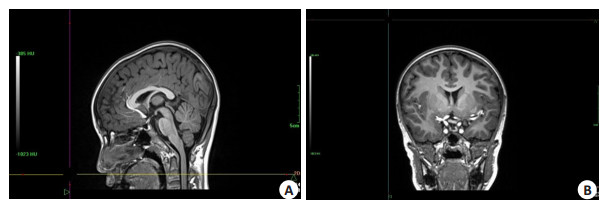
图 2 生长激素缺乏症患儿治疗前后垂体的变化
A: 生长激素缺乏症患儿治疗前矢状位图; B: 生长激素缺乏症患儿治疗前冠状位图; C: 生长激素缺乏症患儿治疗后矢状位图; D: 生长激素缺乏症患儿治疗后冠状位图.
Figure 2. Changes of pituitary in children with growth hormone deficiency before and after treatment.
表 1 生长激素治疗前后垂体大小比较
Table 1. Comparison of pituitary size before and after growth hormone treatment (Mean±SD)
经线 治疗前 治疗后 3~10岁 11~16岁 17~21岁 3~10岁 11~16岁 17~21岁 矢状高径 3.81±0.18# 3.71±0.23# 3.86±0.11# 3.41±0.12* 3.01±0.11* 3.11±0.01* 矢状后径 7.23±1.11# 7.26±1.32# 7.93±1.47# 7.03±1.01* 7.06±0.42* 7.01±1.01* 冠状高径 3.87±0.23# 3.65±0.24# 3.47±0.39# 3.21±0.17* 3.45±0.21 3.21±0.11* 冠状宽径 10.23±1.21# 10.8±1.26# 9.21±1.31# 10.03±1.23 9.74±1.01* 8.21±1.11* #P < 0.05 vs正常儿童; *P < 0.05 vs治疗前.  下载: 导出CSV
下载: 导出CSV
-
[1] 张琪, 王宇, 林祥涛, 等. 完全性生长激素缺乏患儿中央沟形态变化的磁共振诊断价值[J]. 中华医学杂志, 2020, 7(3): 182-6. [2] 陈伟伟, 刘焕欣, 刘晶, 等. 儿童身材矮小的病因分析及遗传学诊断[J]. 中国当代儿科杂志, 2019, 21(4): 381-6. https://www.cnki.com.cn/Article/CJFDTOTAL-DDKZ201904018.htm [3] 中华医学会内分泌学分会. 成人生长激素缺乏症诊治专家共识(2020版)[J]. 中华内分泌代谢杂志, 2020, 36(12): 995-1002. [4] 赵诸慧, 奚立, 程若倩, 等. 生长激素治疗生长激素缺乏症儿童对骨代谢的影响及其相关性研究[J]. 临床和实验医学杂志, 2016, 15 (22): 2246-9. https://www.cnki.com.cn/Article/CJFDTOTAL-SYLC201622024.htm [5] 张彧, 吴安华, 韩帅, 等. MRI影像三维重建在垂体瘤质地的术前评估中的应用[J]. 中国医科大学学报, 2019, 48(3): 220-4, 229. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGYK201903006.htm [6] 王梦珂, 白岩, 冯芹, 等. 磁共振成像技术在垂体瘤检出、诊断及疗效评估中的研究进展[J]. 磁共振成像, 2021, 12(1): 85-8. https://www.cnki.com.cn/Article/CJFDTOTAL-CGZC202101021.htm [7] 林丽君, 陈鹏, 吕芳滨. 垂体MRI形态测量对中枢性性早熟女性患儿的临床诊断价值[J]. 中国妇幼保健, 2021, 36(24): 5825-8. https://www.cnki.com.cn/Article/CJFDTOTAL-ZFYB202124065.htm [8] 王波, 戴敏方. 儿童中枢性尿崩症的垂体MRI表现分析[J]. 中国医学影像技术, 2002, 18(8): 751-2. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYXX200208011.htm [9] 林光武, 杨宁, 张涛. 正常垂体MRI改变与激素水平变化相关性研究[J]. 实用全科医学, 2005, 3(1): 68-9. https://www.cnki.com.cn/Article/CJFDTOTAL-SYQY200501066.htm [10] 高雅君, 徐和平, 何四平. 原发垂体性生长激素缺乏儿童垂体形态学的MRI研究[J]. 医学临床研究, 2008(9): 1566-8. https://www.cnki.com.cn/Article/CJFDTOTAL-HNYZ200809011.htm [11] 徐超, 张欣贤, 李成龙, 等. 生长激素缺乏矮小儿童垂体的MR1表现及常见病因分析[J]. 实用放射学杂志, 2019(4): 621-5. [12] 牛庆玲, 夏宏伟. 重组人生长激素对生长激素缺乏症儿童生长及骨代谢的影响[J]. 中国妇幼保健, 2016, 31(8): 1638-40. https://www.cnki.com.cn/Article/CJFDTOTAL-ZFYB201608026.htm [13] 刘应科, 张知新. 生长激素替代治疗前后生长激素缺乏症患儿脂代谢变化的研究进展[J]. 中日友好医院学报, 2009, 23(6): 370-2. https://www.cnki.com.cn/Article/CJFDTOTAL-ZRYH200906017.htm [14] 刘卉, 张强, 杭伟, 等. 侵袭性垂体腺瘤磁共振成像特征与预后相关性分析[J]. 中华耳鼻咽喉头颈外科杂志, 2020, 55(10): 926-33. [15] 杨小燕, 叶明伟, 苏文达, 等. 垂体MRI及骨龄X线评估与儿童中枢性早熟的相关性研究及对临床诊治方案指导的研究[J]. 现代医用影像学, 2019, 28(6): 1331-2, 1354. https://www.cnki.com.cn/Article/CJFDTOTAL-XDYY201906048.htm [16] Huang J, Sarma A, Gupta N, et al. Noncontrast MRI protocol for selected pediatric pituitary endocrinopathies: a procedure with high diagnostic yield and potential to reduce anesthesia and gadoliniumbased contrast exposure[J]. AJNR Am J Neuroradiol, 2021, 42(10): 1884-90. [17] Almaghraby A, Jaju A, Ryan ME, et al. Is gadolinium contrast necessary for pituitary MRI in the evaluation of pediatric short stature and growth hormone deficiency?[J]. Horm Res Paediatr, 2021, 94(5/6): 201-10. [18] Sheldon BL, O'Brien MW, Adamo MA. Growth hormone replacement therapy: is it safe to use in children with asymptomatic pituitary lesions?[J]. J Pediatr Endocrinol Metab, 2021, 34(12): 1525-9. [19] Obara-Moszyńska M, Budny B, Kałużna M, et al. CDON gene contributes to pituitary stalk interruption syndrome associated with unilateral facial and abducens nerve palsy[J]. J Appl Genet, 2021, 62 (4): 621-9. [20] Hosseinirad H, Yadegari P, Mohanazadeh Falahieh F, et al. Disorders of sex development and female reproductive capacity: a literature review[J]. Syst Biol Reprod Med, 2021, 67(5): 323-36. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 142
- HTML全文浏览量: 149
- PDF下载量: 6
- 被引次数: 0