



Clinical value of 3D-STIR magnetic resonance sequence in the diagnosis of cervical spondylotic radiculopathy
-
摘要:
目的 探讨三维反转恢复快速自旋回波(3D-STIR)序列在显示颈部节前神经根受压情况,以及颈椎间盘突出与颈部神经根关系的临床应用价值,并评估该技术在不同节段(C6神经根及C7神经根)的诊断价值。 方法 收集2021年9月~2022年3月于牡丹江医学院附属红旗医院就诊的有颈部疼痛、上肢麻木等有神经根受压症状并且临床高度怀疑神经根型颈椎病的100例患者,分别行磁共振常规序列(矢状位T2WI、T1WI、STIR,轴位T2WI)、3D-STIR序列扫描以及结合两种扫描方式判断神经根是否受压,分别统计C5~7单侧单节段神经根传导功能障碍的患者有无神经根受压的影像学表现。3D-STIR序列所有图像采用3D最大信号强调投影与曲面重组等后处理,由2名中高级职称磁共振诊断医师通过对重建后图像显示的神经根形态、走行、受压情况以及椎间盘与神经根关系的影像表现,评价3D-STIR序列在诊断神经根型颈椎病的临床应用价值。 结果 按C6/C7神经根是否受压分为两组,常规核磁平扫、3D-STIR序列以及常规核磁平扫与3D-STIR序列结合诊断结果显示,按C6神经根是否受压,得出一致性分别为0.578、0.758、0.838。按C7神经根是否受压,统计方法同C6神经根,一致性分别为0.559、0.779、0.839。两组常规序列扫描一致性均大于0.40且小于0.75,为中度一致性,3D-STIR及与常规序列相结合一致性均大于0.75,为一致性较高,两组差异有统计学意义(P < 0.05)。3D-STIR序列比常规磁共振序列在显示神经根受压情况上有明显优势。 结论 3.0T磁共振3D-STIR序列以及常规核磁结合3D-STIR在诊断C6/C7神经根受压较仅用常规MRI平扫有一定优势。 -
关键词:
- 三维反转恢复快速自旋回波序列 /
- 磁共振成像 /
- 神经根型颈椎病
Abstract:Objective To investigate the three-dimensional spin echo with short time inversion recovery (3D-STIR) sequence for detecting compression of cervical anterior ganglia nerve roots. To evaluate the diagnostic value of this technique in different segments (C6 nerve root and C7 nerve root). Methods From September 2021 to March 2022, we selected 100 patients with cervical spondylotic radiculopathy with neck pain and upper limb numbness and clinically highly suspected cervical spondylotic radiculopathy. The patients underwent conventional magnetic resonance imaging (sagittal T2WI, T1WI, STIR, Axial T2WI) and 3D-STIR sequence scanning, as well as the combination of the two scanning methods to determine whether nerve root compression, and the imaging manifestations of nerve root compression in patients with C5-7 unilateral and single-segment nerve root conduction dysfunction. All images in the 3D-STIR sequence were postprocessed by 3D maximum signal emphasis projection and surface reconstruction. The images were reconstructed by two MRI diagnostic physicians with intermediate and senior professional title, and the images showed the morphology, movement, compression and intervertebral disc and nerve root relationship. To evaluate the clinical application value of 3D-STIR sequence in the diagnosis of cervical spondylotic radiculopathy. Results The C6/C7 nerve roots were divided into two groups according to whether the nerve roots were compressed or not. The diagnostic results of conventional MRI, 3D-STIR sequence and conventional MRI combined with 3D-STIR sequence were counted. The consistency was 0.578, 0.758 and 0.838 according to whether the nerve roots were compressed or not. According to whether C7 nerve root was compressed or not, the statistical method was the same as that of C6 nerve root, and the consistency was 0.559, 0.779 and 0.839, respectively. The consistency of conventional sequence scanning in both groups was greater than 0.40 and less than 0.75, indicating moderate consistency. The consistency of 3D-STIR and combination with conventional sequence was greater than 0.75, indicating high consistency. The final significance test of the two groups showed statistically significant difference (P < 0.05). 3D-STIR sequences have a significant advantage over conventional MR sequences in revealing nerve root compression. Conclusion 3.0 T MR 3D-STIR sequence and conventional MRI combined with 3D-STIR have some advantages in the diagnosis of C6/C7 nerve root compression compared with conventional MRI plain scan. -

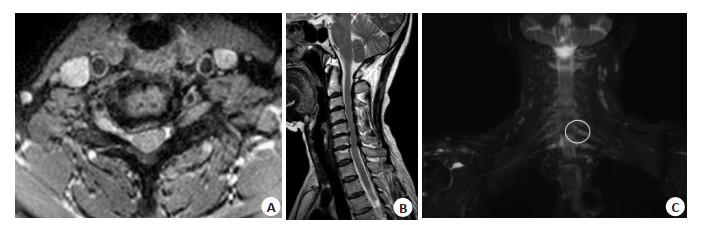
图 1 C6神经根常规MRI扫描及3D-STIR序列扫描
患者男, 58岁, 前臂桡侧放射性疼痛及麻木. A~B: 常规MRI扫描未见椎间盘突出; C: 3D-STIR扫描MIP图像可见C6神经根受压变窄(圆圈所示), 并且可见椎间盘信号减低, 为椎间盘变性.
Figure 1. Conventional MRI and 3D-stir sequence scans of C6 nerve roots.

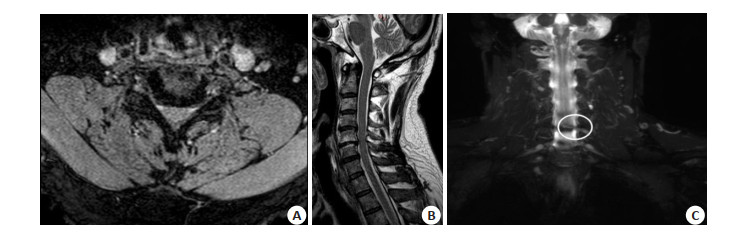
图 2 C7神经根常规MRI扫描及3D-STIR序列扫描
患者女, 55岁, 左手麻木. A~B: 常规MRI扫描未见椎间盘突出, 轴位可见双侧对称,形态正常; C: 3D-STIR扫描MIP图像可见C7神经根受压变窄(圆圈所示), 并且可见椎间盘信号减低,为椎间盘变性
Figure 2. Conventional MRI and 3D-stir sequence scans of C7 nerve roots.
表 1 临床诊断C6时常规MRI扫描、3D-STIR序列及3D-STIR+常规MRI扫描诊断结果
Table 1. Diagnostic results of conventional MRI scan, 3D-STIR sequence and 3D-STIR + conventional MRI scan at clinical diagnosis of C6 (n)
方法 临床诊断定位阳性 临床诊断定位阴性 总计 Kappa P MRI常规扫描 0.578 < 0.01 C6神经根受压 43 10 53 C6神经根未受压 11 36 47 3D-STIR序列 0.758 < 0.01 C6神经根受压 48 6 54 C6神经根未受压 6 40 46 常规MRI结合3D-STIR 0.838 < 0.01 C6神经根受压 50 4 54 C6神经根未受压 4 42 46 总计 54 46 100 < 0.05 3D-STIR: 三维反转恢复快速自旋回波序列.  下载: 导出CSV
下载: 导出CSV
表 2 临床诊断C7时常规MRI扫描、PROSET序列及PROSET+常规MRI扫描诊断结果
Table 2. Diagnostic results of conventional MRI scan, PROSET sequence and PROSET + conventional MRI scan at clinical diagnosis of C7 (n)
方法 临床诊断定位阳性 临床诊断定位阴性 总计 Kappa P MRI常规扫描 0.559 < 0.01 C7神经根受压 36 12 48 C7神经根未受压 10 42 52 3D-STIR序列 0.779 < 0.01 C7神经根受压 41 6 47 C7神经根未受压 5 48 53 常规MRI结合3D-STIR 0.839 < 0.01 C7神经根受压 42 4 46 C7神经根未受压 4 50 54 总计 46 54 100 < 0.05
下载: 导出CSV
表 3 MRI常规扫描、3D-STIR及3D-STIR序列+MRI常规扫描对责任受压神经根诊断能力(以临床定位诊断结果为标准)
Table 3. Diagnostic ability of conventional MRI scan, 3D-STIR and 3D-STIR sequence + conventional MRI scan on nerve roots with responsibility compression (based on clinical location diagnosis) (%)
方法 敏感度 特异性 阳性预测值 阴性预测值 准确度 C6神经根MRI常规序列 79.6 78.3 81.1 76.6 79.0 C6神经根3D-STIR序列 88.9 86.7 88.9 87.0 88.0 C6神经根常规扫描结合PROSET序列 92.6 91.3 92.6 91.3 92.0 C7神经根MRI常规序列 78.2 77.8 75.0 80.8 78.0 C7神经根3D-STIR序列 89.1 88.9 87.2 90.6 89.0 C7神经根常规扫描结合PROSET序列 91.3 92.6 91.3 92.6 95.0
下载: 导出CSV
-
[1] 宋超一, 邵翠娟. 神经根型颈椎病椎间孔狭窄特点及多层螺旋CT (MSCT)诊断价值[J]. 影像研究与医学应用, 2021, 5(7): 207-8. doi: 10.3969/j.issn.2096-3807.2021.07.102 [2] Yang F, Li WX, Liu Z, et al. Balance chiropractic therapy for cervical spondylotic radiculopathy: study protocol for a randomized controlled trial[J]. Trials, 2016, 17(1): 1-6. doi: 10.1186/s13063-015-1128-9 [3] Eguchi Y, Oikawa Y, Suzuki M, et al. Diffusion tensor imaging of radiculopathy in patients with lumbar disc herniation[J]. Bone Jt J, 2016, 98-B(3): 387-94. doi: 10.1302/0301-620X.98B3.36036 [4] 王晓雯, 王鹏, 陈怡楠, 等. 不同磁共振腰骶丛神经成像序列的临床研究[J]. 现代生物医学进展, 2016, 16(10): 1862-6. https://www.cnki.com.cn/Article/CJFDTOTAL-SWCX201610015.htm [5] Hashimoto K, Tanaka Y, Tsubakino T, et al. Imaging diagnosis of lumbar foraminal stenosis in the fifth lumbar nerve root: reliability and reproducibility of T1-weighted three-dimensional lumbar MRI [J]. J Spine Surg, 2021, 7(4): 502-9. doi: 10.21037/jss-21-63 [6] Grasso D, Borreggine C, Melchionda D, et al. Role of 3D MRI with proset technique in the evaluation of lumbar radiculopathy[J]. J Biol Regul HomeostAgents, 2013, 27(3): 817-25. [7] 王祺, 李会侠, 冯琳, 等. 3.0 T MRI 3种扫描序列对颈神经根成像的对比研究[J]. 磁共振成像, 2018, 9(10): 759-63. doi: 10.12015/issn.1674-8034.2018.10.008 [8] Ditunno JF, Young W, Donovan WH, et al. The international standards booklet for neurological and functional classification of spinal cord injury[J]. Spinal Cord, 1994, 32(2): 70-80. doi: 10.1038/sc.1994.13 [9] 孙宇, 陈琪福. 第二届颈椎病专题座谈会纪要[J]. 中华外科杂志, 1993, 31(8): 472-6. doi: 10.3760/j:issn:0529-5815.1993.08.012 [10] 李曙明, 尹战海, 王莹. 神经根型颈椎病的影像学特点和分型[J]. 中国矫形外科杂志, 2013, 21(1): 7-11. https://www.cnki.com.cn/Article/CJFDTOTAL-ZJXS201301003.htm [11] Scarabino T, Pollice S. Imaging spine after treatment. A case-based atlas[M]. Milan: Springer, 2013 [12] 曾秀君, 何海龙, 陈锋. 枢经推拿联合针刺治疗神经根型颈椎病的疗效分析[J]. 现代医学与健康研究电子杂志, 2022, 6(10): 95-8. https://www.cnki.com.cn/Article/CJFDTOTAL-XYJD202210029.htm [13] Theodore N. Degenerative cervical spondylosis[J]. N Engl J Med, 2020, 383(2): 159-68. doi: 10.1056/NEJMra2003558 [14] 贾雁, 邱祖云, 孙小洁, 等. 颈源性头痛的影像学特征分析[J]. 中华中医药杂志, 2021, 36(6): 3644-7. https://www.cnki.com.cn/Article/CJFDTOTAL-BXYY202106140.htm [15] 吴志钧. 臂丛神经应用DWIBS序列与3D-STIR序列增强检查的成像质量对比研究[J]. 现代医用影像学, 2021, 30(6): 1070-2. https://www.cnki.com.cn/Article/CJFDTOTAL-XDYY202106023.htm [16] Liu YT, Li JM, Li H, et al. AMP-activated protein kinase activation in dorsal root ganglion suppresses mTOR/p70S6K signaling and alleviates painful radiculopathies in lumbar disc herniation rat model [J]. Spine, 2019, 44(15): E865-E872. [17] 吕银章, 孔祥泉, 刘定西, 等. 3D-STIR序列增强扫描在腰骶丛神经成像中的应用研究[J]. 临床放射学杂志, 2011, 30(2): 231-4. https://www.cnki.com.cn/Article/CJFDTOTAL-LCFS201102031.htm [18] 于杰, 朱立国, 房敏, 等. 神经根型颈椎病压痛部位分布及其与神经节段的关系[J]. 环球中医药, 2011, 4(4): 250-2. https://www.cnki.com.cn/Article/CJFDTOTAL-HQZY201104006.htm [19] 杨传红, 邱光, 杨骁驰, 等. 腰椎间盘水信号分数在椎间盘退变及突出的应用价值[J]. 临床放射学杂志, 2020, 39(11): 2326-9. https://www.cnki.com.cn/Article/CJFDTOTAL-LCFS202011041.htm [20] Chhabra A, Zhao LX, Carrino JA, et al. MR neurography: advances [J]. Radiol Res Pract, 2013, 2013: 809568. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 255
- HTML全文浏览量: 92
- PDF下载量: 9
- 被引次数: 0