



Conventional MRI signal changes and quantitative susceptibility mapping to assess potential brain damage in neonates with hyperbilirubinemia
-
摘要:
目的 探究常规MRI信号改变及定量磁敏感加权图像(QSM)定量评估足月新生儿高胆红素血症患儿潜在脑损伤的价值。 方法 回顾性分析2019年1月~2020年12月我院收治的临床综合诊断为高胆红素血症的足月新生儿50例(Ⅰ组),另选48例胆红素不高的无脑相关疾病的足月新生儿作为对照组(Ⅱ组)。再根据血清总胆红素水平将Ⅰ组分为轻中度升高组和重度及极重度升高组。所有患儿均行治疗前MR平扫、扩散加权成像扫描,其中38例患儿行QSM检查,对比不同组别患儿MR信号强度之间差异及其与血清总胆红素水平的相关性;比较胆红素升高患儿与对照组患儿不同核团磁化率之间的差异,及其与血清总胆红素水平之间的相关性。 结果 胆红素升高患儿更容易出现苍白球(GP)T1WI高信号表现(36/12 vs 13/37,P < 0.001);3组之间GP的T1WI信号强度(SI1)/T2WI信号强度(SI2)比值的差异有统计学意义(P=0.034),但SI1GP、SI2GP、SI1P、SI2P、SI1FWM、SI2FWM、SI1FGM、SI2FGM、SI1GP/SI1P、SI1GP/SI1FWM、SI1GP/SI1FGM、△SI1(GP-P)、△SI1(GP-FGM)、△SI1(GP-P)/SI1GP、△SI1(GP-P)/△SI1(GP-FGM)、△SI1(GP-P)/△SI1(GP-FWM)的差异均无统计学意义(P > 0.05);SI1 GP/SI2GP与血清总胆红素水平呈极弱相关关系(r=0.261,P=0.009),当日龄与出生体质量控制时,SI1 GP/SI2GP、△SI1(GP-P)/△SI1(GP-FGM)与血清总胆红素仍呈极弱相关(r=0.230,P=0.014;r=-0.184,P=0.014)。胆红素升高组与对照组之间苍白球、壳核、丘脑底核及脑干的磁化率之间的差异均有统计学意义(P < 0.05);且壳核及丘脑底核与血清总胆红素水平呈轻度相关(r=-0.419,P= 0.011;r=-0.391,P=0.018),而苍白球及脑干与血清胆红素呈中度相关(r=-0.620,P < 0.001;r=-0.630,P < 0.001)。 结论 高胆红素血症新生儿单纯评价苍白球T1WI高信号有一定的诊断意义,但是常规MR信号强度与血清胆红素是否升高没有明确相关性;而苍白球、壳核、丘脑底核及脑干QSM测定的磁化率可能可以更早的发现高胆红素血症新生儿潜在脑损伤。 Abstract:Objective To explore the value of conventional MRI signal changes and quantitative susceptibility mapping (QSM) in quantitative assessment of potential brain injury in neonates with hyperbilirubinemia. Methods Fifty neonates (group Ⅰ) who were clinically diagnosed with neonatal hyperbilirubinemia in our hospital were retrospectively analyzed from January 2019 to December 2020. Forty-eight neonates without hyperbilirubinemia and brain-related diseases were the control group (group Ⅱ). All children underwent MR plain scan and diffusion weighted imaging scan before treatment, and 38 children underwent QSM examination. The differences between the MR signal intensities of children in different groups and their correlation with serum total bilirubin levels were compared. The differences between the magnetic susceptibility of different nuclei in children with elevated bilirubin and the control group were compared, and their correlation with serum total bilirubin levels were analyzed. Results Children with hyperbilirubinemia were more inclined to have high signal intensity of the globus pallidus on T1WI (36/12 vs 13/37, P < 0.001). The difference of SI1GP/SI2GP was statistically significant (P=0.034), while the difference of other indicators were not statistically significant (P > 0.05). There was a very weak correlation between the SI1GP/SI2GP with serum total bilirubin level (r=0.261, P=0.009).When the age and birth weight were controlled, the SI1 GP/SI2GP, ΔSI1(GP-P)/ΔSI1(GP-FGM) was a very weak correlated(r=0.230, P=0.014; r=-0.184, P=0.014). There were statistically significant differences in the magnetic susceptibility of the globus pallidus, putamen, subthalamic nucleus and brainstem between the elevated bilirubin group and the control group(P < 0.05).The magnetic susceptibility of putamen and subthalamic nucleus were slightly correlated with serum total bilirubin levels (r=-0.419, P=0.011; r=-0.391, P=0.018), while there was a moderate correlation between the magnetic susceptibility of globus pallidus and brainstem and serum bilirubin levels (r=-0.620, P < 0.001; r=-0.630, P < 0.001). Conclusion The evaluating signal intensity of the globus pallidus on T1WI is helpful for thediagnosis of neonates with hyperbilirubinemia. There is no clear correlation between the signal intensity of conventional MR and the increase of serum bilirubin. The magnetic susceptibility measured by QSM in the globus pallidus, putamen, subthalamic nucleus and brainste may earlier indicate the potential brain damage in neonates with hyperbilirubinemia. -

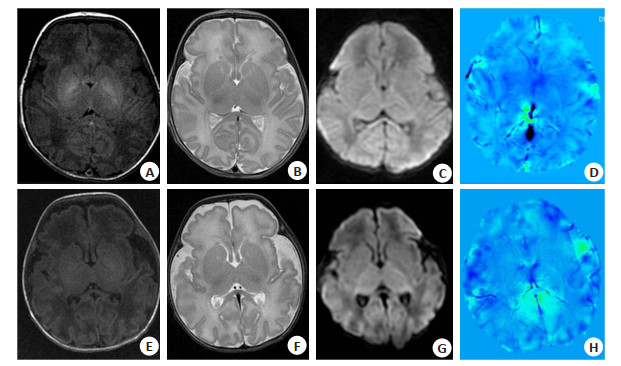
图 1 两患儿的T1WI/T2WI/DWI平扫图像及QSM后处理图像
A~D: 高胆红素血症患儿, 男, 日龄19 d, 出生孕周38周3 d; 血清总胆红素425.6 μmol/L; 常规MR平扫示苍白球对称性T1WI高信号; E~H:正常对照组新生儿, 女, 日龄10 d, 出生孕周39周3 d;血清总胆红素77.7 μmol/L; 常规MR平扫未见异常信号. D、H均为QSM重建后图像.
Figure 1. The T1WI/T2WI/DWI plain scan images and QSM post-processed images of two children.
表 1 各组患儿常规MR信号强度及各计算值之间的差异
Table 1. Differences between conventional MRI signal intensity and the calculated values of children in each group (Mean±SD)
指标 所有患者 Ⅰa组 Ⅰb组 Ⅱ组 F/Z P SI1GP 1233.65±726.26 1184.16±659.41 1148.54±729.17 1173.68±761.97 1.294 0.279 SI2GP 1905.37±863.77 1910.54±882.79 1880.64±832.10 1911.19±880.38 0.009 0.991 SI1P 910.79±529.61 886.77±486.27 1097.38±521.21 856.84±555.06 1.411 0.249 SI2P 2051.64±973.31 2056.60±1000.18 2021.72±911.91 2059.60±997.06 0.010 0.990 SI1FWM 763.39±422.58 735.15±386.86 901.64±404.47 730.38±449.08 1.186 0.310 SI2FWM 2046.70±994.21 2047.79±1004.65 2089.12±958.43 2030.07±1020.31 0.023 0.978 SI1FGM 548.60±338.29 513.39±300.37 686.62±354.95 520.32±349.49 1.872 0.159 SI2FGM 2698.55±1387.83 2747.05±1501.95 2696.23±1190.37 2667.09±1404.28 0.031 0.969 SI1GP/SI1P 1.36±0.15 1.34±0.14 1.34±0.09 1.37±0.17 0.740 0.480 SI1GP/SI1FWM 2.15(1.33, 5.27) 2.28(1.43, 5.11) 2.09(1.61, 3.23) 2.12(1.33, 5.27) 2.097 0.350 SI1GP/SI1FGM 1.59±0.28 1.60±0.29 1.59±0.25 1.59±0.28 0.002 0.998 ΔSI1(GP-FGM) 685.05±454.09 670.78±425.70 794.95±433.90 653.36±481.82 0.655 0.522 ΔSI1(GP-P) 322.86±233.89 297.39±207.55 384.17±234.30 316.85±250.43 0.821 0.443 SI1GP/SI2GP 0.64±0.27 0.63±0.266 0.78±0.22 0.59±0.28 3.493 0.034 ΔSI1(GP-P)/SI1GP 0.25±0.08 0.24±0.08 0.25±0.06 0.26±0.08 0.577 0.564 ΔSI1(GP-P)/ΔSI1(GP-FGM) 1.43±0.38 1.52±0.41 1.47±0.46 1.35±0.32 2.082 0.130 ΔSI1(GP-P)/ΔSI1(GP-FWM) 2.25±0.55 2.38±0.57 2.13±0.48 2.20±0.54 1.602 0.207 组Ⅰa: 轻中度升高组; 组Ⅰb: 重度及极重度升高组; 组Ⅱ: 对照组. SI1: T1WI信号强度; SI2: T2WI信号强度; GP: 苍白球; P: 壳核; FWM: 额叶白质; FGM: 额叶灰质.  下载: 导出CSV
下载: 导出CSV
表 2 常规MR信号强度及各计算值与血清总胆红素水平的相关性研究
Table 2. The correlation between the conventional MR signal intensity and the calculated values with serum total bilirubin level
指标 r P r1* P1* SI1GP 0.132 0.194 0.124 0.120 SI2GP -0.028 0.787 0.001 0.498 SI1P 0.149 0.143 0.129 0.112 SI2P -0.031 0.760 0.003 0.487 SI1FWM 0.136 0.181 0.126 0.117 SI2FWM -0.010 0.926 0.019 0.430 SI1FGM 0.165 0.104 0.156 0.070 SI2FGM -0.012 0.903 0.018 0.434 SI1GP/SI1P -0.093 0.361 -0.014 0.447 SI1GP/SI1FWM -0.117 0.253 -0.065 0.270 SI1GP/SI1FGM -0.016 0.878 0.011 0.458 ΔSI1(GP-FGM) 0.089 0.385 0.083 0.216 ΔSI1(GP-P) 0.074 0.471 0.096 0.182 SI1GP/SI2GP 0.261 0.009 0.230 0.014 ΔSI1(GP-P)/SI1GP -0.062 0.547 0.032 0.380 ΔSI1(GP-P)/ΔSI1(GP-FGM) 0.108 0.292 0.018 0.434 ΔSI1(GP-P)/ΔSI1(GP-FWM) -0.064 0.530 -0.184 0.041 *r1为纠正日龄及体质量后的r值,P1为对应的P值.
下载: 导出CSV
表 3 胆红素升高组与对照组之间各核团磁化率的差异
Table 3. Differences in the magnetic susceptibility of each nucleus between the elevated bilirubin group and the control group (Mean±SD)
指标 总体 胆红素升高组 对照组 T P 苍白球 156.35±105.70 253.39±75.52 94.60±69.41 6.468 < 0.001 壳核 255.04±172.53 364.00±207.47 185.70±100.08 3.466 0.001 内囊后肢 253.42±133.07 260.14±114.63 249.14±146.05 0.239 0.813 内囊前肢 198.59±128.65 231.20±149.28 177.84±112.38 1.222 0.230 丘脑底核 304.74±165.63 379.29±204.36 257.30±117.51 2.280 0.029 丘脑背侧核 293.01±157.79 325.14±158.77 272.57±157.37 0.974 0.337 大脑脚 254.52±165.47 290.18±151.07 231.82±173.56 1.032 0.309 小脑齿状核 265.89±143.20 299.73±205.34 244.36±82.63 1.136 0.264 桥臂 371.14±217.84 432.21±150.74 332.27±246.89 1.358 0.183 红核黑质 244.20±209.80 203.21±110.20 270.29±252.99 -0.934 0.357 脑干 325.95±151.98 451.00±116.59 246.37±114.10 5.202 < 0.001
下载: 导出CSV
表 4 所有进行QSM检查的患儿各核团磁化率与血清总胆红素水平之间的相关性研究
Table 4. The correlation between the magnetic susceptibility of each nucleus and the serum total bilirubin level in all children who underwent QSM examination
指标 r P 苍白球 -0.620 < 0.001 壳核 -0.419 0.011 内囊后肢 0.267 0.115 内囊前肢 -0.104 0.545 丘脑底核 -0.391 0.018 丘脑背侧核 -0.018 0.916 大脑脚 0.091 0.598 小脑齿状核 -0.163 0.343 桥臂 -0.300 0.076 红核黑质 0.304 0.072 脑干 -0.630 < 0.001
下载: 导出CSV
-
[1] 康志雷, 刘朝艳, 马永倩, 等. 常规MRI和~1H-MRS在新生儿期黄疸病情评估中的价值[J]. 放射学实践, 2020, 35(8): 1054-8. https://www.cnki.com.cn/Article/CJFDTOTAL-FSXS202008023.htm [2] 曹静, 刘光耀, 李丽, 等. 新生儿胆红素脑病早期诊断的MR研究进展[J]. 磁共振成像, 2019, 10(4): 303-7. https://www.cnki.com.cn/Article/CJFDTOTAL-CGZC201904016.htm [3] 于金红, 王静石, 苗延巍, 等. DWI及3D SWAN提高新生儿胆红素脑病病理生理机制的认识[J]. 磁共振成像, 2020, 11(11): 994-8. doi: 10.12015/issn.1674-8034.2020.11.008 [4] 荆彦平, 强孔俊, 骆宾, 等. 急、慢性胆红素脑病MRI特征及鉴别诊断[J]. 临床放射学杂志, 2018, 37(11): 1906-9. https://www.cnki.com.cn/Article/CJFDTOTAL-LCFS201811034.htm [5] 程卓, 唐世龙, 周瑜, 等. 定量磁化率成像在孤独症儿童脑铁含量的应用研究[J]. 中国临床医学影像杂志, 2022, 33(2): 77-81. https://www.cnki.com.cn/Article/CJFDTOTAL-LYYX202202001.htm [6] 宁宁, 金超, 张卫善, 等. 0~6岁儿童脑深部灰质核团铁的变化: 定量磁敏感图与R2*的比较[J]. 磁共振成像, 2021, 12(6): 22-6. https://www.cnki.com.cn/Article/CJFDTOTAL-CGZC202106005.htm [7] Biondetti E, Rojas-Villabona A, Sokolska M, et al. Investigating the oxygenation of brain arteriovenous malformations using quantitative susceptibility mapping[J]. NeuroImage, 2019, 199: 440-53. [8] 孟小丽, 张雷, 王晓虎, 等. 新生儿重度高胆红素血症的MRI信号特征分析[J]. 磁共振成像, 2018, 9(10): 768-72. https://www.cnki.com.cn/Article/CJFDTOTAL-CGZC201810013.htm [9] 李豪刚, 张玉忠, 陈凯, 等. MRI在新生儿胆红素脑病中诊断价值[J]. 放射学实践, 2013, 28(10): 1062-5. https://www.cnki.com.cn/Article/CJFDTOTAL-FSXS201310024.htm [10] 中华医学会儿科学分会新生儿学组, 《中华儿科杂志》编辑委员会. 新生儿高胆红素血症诊断和治疗专家共识[J]. 中华儿科杂志, 2014, 52 (10): 745-8. [11] 吴武林, 张平, 娄明武, 等. DWI及常规MR在新生儿高胆红素血症及胆红素脑病诊断中的应用[J]. 实用放射学杂志, 2011, 27(8): 1242-4, 1248. [12] 易明岗, 姜忠强, 赵建设, 等. 苍白球与壳核T1WI信号强度比值在新生儿急性胆红素脑病分级及预后中的价值[J]. 中华放射学杂志, 2017, 51(3): 214-8. [13] Taoka T, Aida N, Ochi T, et al. Transient hyperintensity in the subthalamic nucleus and globus pallidus of newborns on T1-weighted images[J]. AJNRAm J Neuroradiol, 2011, 32(6): 1130-7. [14] 李文, 任转勤, 田宏哲. MR T1 mapping成像在诊断新生儿高胆红素血症脑损伤中的应用价值[J]. 实用放射学杂志, 2022, 38(5): 818-21. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYXX202106032.htm [15] 翁淑萍, 施跃全, 方如旗, 等. 新生儿急性胆红素脑病的磁共振成像表现及其诊断价值[J]. 福建医科大学学报, 2012, 46(1): 64-7. https://www.cnki.com.cn/Article/CJFDTOTAL-FJYD201201021.htm [16] 尹家瑜, 申炜, 许梅海, 等. 苍白球与壳核T1WI信号比值在足月儿急性高胆红素相关脑病的临床研究[J]. 实用放射学杂志, 2019, 35(3): 433-6. [17] 张钊, 马永倩, 张捷宇, 等. 头颅磁共振G/P值、GP/CSF值在新生儿急性胆红素脑病早期的预测价值[J]. 临床放射学杂志, 2022, 41(2): 325-9. https://www.cnki.com.cn/Article/CJFDTOTAL-LCFS202202024.htm [18] 靳金岩, 李洪义. MRI及功能成像改变对新生儿高胆红素脑病临床价值分析[J]. 中国CT和MRI杂志, 2019, 17(1): 12-4, 24. https://www.cnki.com.cn/Article/CJFDTOTAL-CTMR201901004.htm [19] 李俊, 李雅丽, 高敏, 等. 新生儿胆红素脑病磁共振波谱成像在苍白球的特征分析[J]. 临床放射学杂志, 2018, 37(6): 1025-9. https://www.cnki.com.cn/Article/CJFDTOTAL-LCFS201806036.htm [20] Sarı S, Yavuz A, Batur A, et al. Brain magnetic resonance imaging and magnetic resonance spectroscopy findings of children with kernicterus[J]. Pol J Radiol, 2015, 80: 72-80. [21] 邓敏, 何四平, 伍光春, 等. 胆红素脑病所致听力受损患儿听觉通路纤维束的DTI研究: 各向异性分数和其他扩散系数的变化[J]. 临床放射学杂志, 2017, 36(11): 1679-83. https://www.cnki.com.cn/Article/CJFDTOTAL-LCFS201711035.htm [22] 许欢, 孟庆林, 樊文萍, 等. 正常人脑皮层下灰质核团定量磁敏感成像的可重复性分析[J]. 南方医科大学学报, 2020, 40(12): 1810-5. https://www.cnki.com.cn/Article/CJFDTOTAL-DYJD202012018.htm [23] Zhang YY, Shi JJ, Wei HJ, et al. Neonate and infant brain development from birth to 2 years assessed using MRI-based quantitative susceptibility mapping[J]. NeuroImage, 2019, 185: 349-60. [24] Barateiro A, Chen SJ, Yueh MF, et al. Reduced myelination and increased Glia reactivity resulting from severe neonatal hyperbilirubinemia[J]. Mol Pharmacol, 2016, 89(1): 84-93. [25] 廖继研, 李木兰, 张桂花. 新生儿高胆红素血症对脑干听觉诱发电位影响的相关性研究[J]. 中国医药科学, 2017, 7(16): 54-7. https://www.cnki.com.cn/Article/CJFDTOTAL-GYKX201716018.htm [26] 郭莉莉, 王德杭, 张辉, 等. 磁敏感加权成像在新生儿高胆红素血症颅内出血的应用研究[J]. 中国临床医学影像杂志, 2018, 29(11): 764-70. https://www.cnki.com.cn/Article/CJFDTOTAL-LYYX201811004.htm [27] Tortora D, Severino M, Sedlacik J, et al. Quantitative susceptibility map analysis in preterm neonates with germinal matrixintraventricular hemorrhage[J]. J Magn Reson Imaging, 2018, 48 (5): 1199-207. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 190
- HTML全文浏览量: 72
- PDF下载量: 9
- 被引次数: 0