



Evaluation of left atrial function in essential hypertensive patients with left ventricular hypertrophy based on four-dimensional echocardiographic quantitative analysis
-
摘要:
目的 基于超声四维左房定量分析(4DLAQ)技术评价原发性高血压(EH)左心室肥厚(LVH)患者的左房功能。 方法 选择EH患者80例,根据LVH的新标准将患者分为LVH组无LVH(NLVH)组,同时选取36例健康体检者作为对照组,3组均采用二维超声心动图测量得到二维超声数据,采用4DLAQ技术测量及分析得到左房容积参数包括左房最小容积(LAVmin)、左房最大容积(LAVmax)、左房收缩前容积(LAVpreA)、左房整体射血分数(LAEF);左房应变参数包括左房储备期长轴应变、左房管道期长轴应变、左房收缩期长轴应变、左房储备期环形应变、左房管道期环形应变、左房收缩期环形应变,比较3组二维和四维技术所得数据的差异。 结果 3组收缩压及舒张压的差异有统计学意义(P < 0.05)。3组左心房内径、双平面左室射血分数、室间隔厚度、左心室舒张末期内径、左心室后壁厚度、E/e’的差异均有统计学意义(P < 0.05)。3组LAVmin、LAVpreA、LAEF、左心房被动射血分数、左心房主动射血分数的差异有统计学意义(P < 0.05),而LVAmax的差异无统计学意义(P > 0.05)。3组左房应变参数的差异均有统计学意义(P < 0.05)。观察者间和观察者内的一致性较好(组内相关系数 > 0.90)。 结论 EH患者左房内径增大早于左室收缩功能受损,随着疾病进展左房容积升高,储存功能、管道功能受损,泵血功能处于NLVH时增加,随着LVH程度加重,左房泵血功能减低。4DLAQ能发现EH患者左房功能细微的改变,其应变参数评价左房功能更敏感,其中环形应变在表达左房管道功能上比纵向应变更具优势。 Abstract:Objective To evaluate left atrial function in essential hypertensive (EH) patients with left ventricular hypertrophy (LVH) based on four-dimensional echocardiographic quantitative (4DLAQ). Methods Eighty EH patients were selected and divided into NLVH group and LVH group according to the new LVH standard. At the same time, 36 healthy subjects were selected as the control group. The participants in the three groups were measured by two-dimensional echocardiography, and the left atrial volume parameters were measured and analyzed by 4DLAQ technology, including left atrial minimum volume (LAVmin), left atrial maximum volume (LAVmax), left atrial pre systolic volume (LAVpreA) and left atrial global ejection fraction (LAEF). The left atrial strain parameters include left atrial reserve long axial strain, left atrial conduit long axial strain, left atrial systolic long axial strain, left atrial reserve circular strain, left atrial conduit circular strain and left atrial systolic circular strain. The differences between the two-dimensional and four-dimensional data of the three groups of participants were compared. Results There were significant differences in mean systolic blood pressure and mean diastolic blood pressure among the three groups (P < 0.05). There were significant differences in left atrial diameter, Biplane LVEF, interventricular septal thickness, left ventricular end-diastolic diameter, left ventricular posterior wall thickness and E/e' among the three groups (P < 0.05). There was significant difference in LAVmin, LAVpreA, LAEF, left atrial passive ejection fraction and left atrial active ejection fraction among the three groups (P < 0.05), but there was no significant difference in LAVmax (P > 0.05). There were significant differences in left atrial strain parameters among the three groups (P < 0.05). The consistency between and within observers was good (ICC > 0.90). Conclusion The increase of left atrial diameter in EH patients is earlier than the impairment of left ventricular systolic function. With the progress of the disease, the left atrial volume increases, the storage function and pipeline function are damaged, and the blood pumping function increases when the blood pumping function is in NLVH. With the aggravation of LVH, the blood pumping function of the left atrium decreases. 4DLAQ can find subtle changes in the left atrial function of EH patients and supplement the technical weakness of the current left atrial research. Its strain parameters are more sensitive to evaluate the left atrial function. Among them, the circular strain is more advantageous than the longitudinal strain in indicating the left atrial conduit function. -

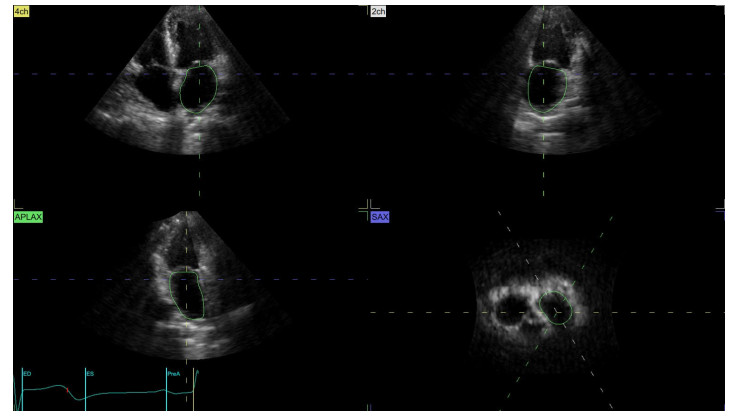
图 2 EchoPAC204软件自动识别并描记左心房心内膜
Figure 2. Echopac204 software automatically identifies and traces the endocardium of left atrium.

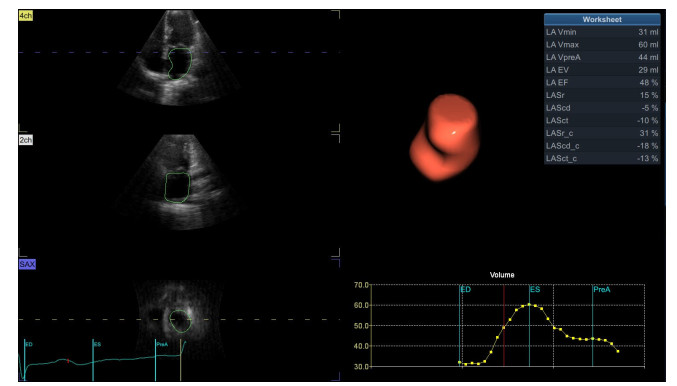
图 3 4DLAQ所测得的左心房容积及应变参数值
Figure 3. Left atrial volume and strain parameter values measured by 4DLAQ.

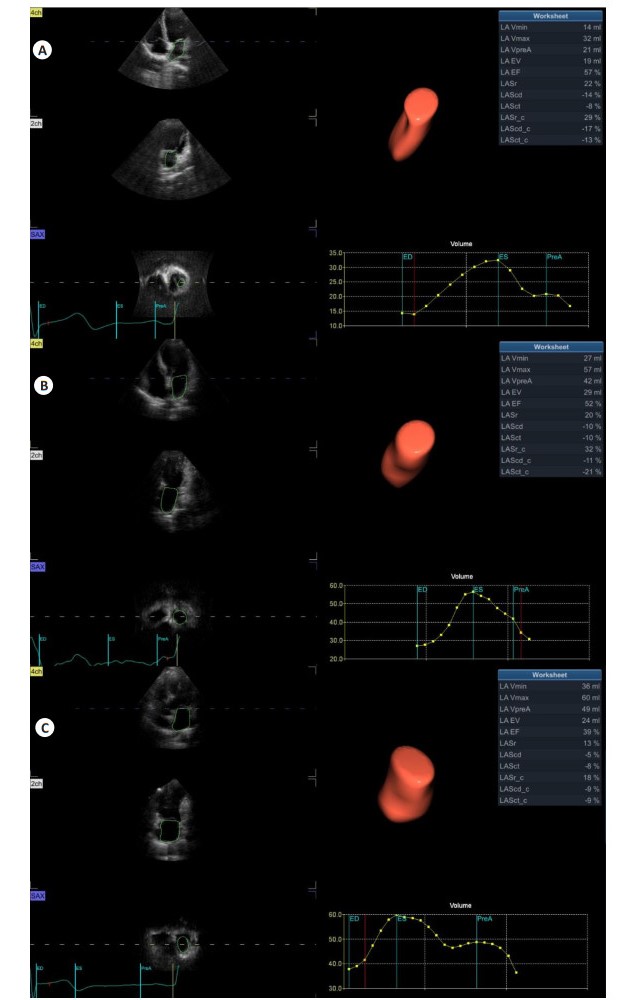
图 4 4D LAQ所测得的三组参与者左房容积和应变结果
A: 对照组; B: NLVH组; C: LVH组.
Figure 4. Left atrial volume and strain results of three groups of participants measured by 4DLAQ.
表 1 三组参与者的临床资料对比
Table 1. Comparison of clinical data of three groups of participants
一般资料 对照组(n=36) NLVH组(n=40) LVH组(n=40) χ2/F/H P 性别[n(%)] 2.566 0.277 男 15(42.00) 24(60.00) 20(50.00) 女 21(58.00) 16(40.00) 20(50.00) 年龄(岁, Mean±SD) 62.72±8.14 61.30±9.14 68.00(54.50, 74.50) 1.805 0.406 心率[次/min, Median (P25, P75)] 73.00(65.25, 79.00) 72.00(68.00, 78.00) 73.00±10.26 0.166 0.920 BMI(kg/m2, Mean±SD) 25.66±3.08 24.95±3.19 26.32±2.94 1.992 0.141 收缩压[mmHg, Median (P25, P75)] 110.00(100.00, 120.00) 130.00(120.00, 142.00) 145.00(130.00, 152.00) 67.393 < 0.001 舒张压[mmHg, Median (P25, P75)] 80.00(75.00, 80.00) 90.00(80.00, 100.00) 100.00(91.25, 110.00) 50.536 < 0.001 空腹血糖[mmol/L, Median (P25, P75)] 5.11(4.12,5.76) 5.20±0.73 4.96(4.37,5.54) 1.162 0.559 总胆固醇[mmol/L, Median (P25, P75)] 3.11(2.84,4.10) 3.45(2.76,4.36) 3.62(2.78,4.46) 2.195 0.334 高密度脂蛋白[mmol/L, Median (P25, P75)] 1.31(1.23,1.46) 1.44(1.26, 1.48) 1.31(1.24,1.45) 5.426 0.066 低密度脂蛋白(mmol/L, Mean±SD) 1.78±0.36 1.64±0.55 1.56(1.45,1.89) 2.525 0.283 甘油三酯[mmol/L, Median (P25, P75)] 1.36(1.04,1.79) 1.22(0.48,1.72) 1.26(0.91,1.59) 4.657 0.097 血肌酐(μmol/L, Mean±SD) 66.89±13.26 63.80±13.51 67.00(59.00,82.25) 3.320 0.190 B型脑钠肽[pg/mL, Median (P25, P75)] 31.76(26.06,36.17) 33.05(10.11) 33.73(26.19,36.57) 0.111 0.946 LVH组: 左心室肥厚组; NLVH组: 无左心室肥厚组.  下载: 导出CSV
下载: 导出CSV
表 2 三组参与者二维超声心动图数据对比
Table 2. Comparison of two-dimensional echocardiography data of three groups of participants
参数 对照组(n=36) NLVH组(n=40) LVH组(n=40) H P LAD(mm, Mean±SD) 35.33±3.98 39.75±2.89* 40.00(38.00, 42.00)* 22.613 < 0.001 Biplane LVEF [%, Median (P25, P75)] 65.00(64.00, 66.00) 63.65±2.19 64.50(63.25, 65.00)* 8.997 0.011 IVST [mm, Median (P25, P75)] 9.00(8.00, 10.00) 10.00(9.00, 11.75)* 12.00(11.00, 13.00)*# 57.671 < 0.001 LVEDD [mm, Median (P25, P75)] 47.00(45.00, 48.00) 47.73±3.71 49.40±3.56* 8.324 0.016 LVPWT [mm, Median (P25, P75)] 9.00(8.00, 9.00) 9.00(9.00, 10.00)* 11.00(10.00, 12.00)*# 42.310 < 0.001 E/e’(Mean±SD) 9.20±2.84 11.38(9.30, 13.64)* 12.71±4.48* 14.957 0.001 *P < 0.05 vs对照组; #P < 0.05 vs NLVH组. LAD: 左心房内径; IVST: 室间隔厚度; Biplane LVEF: 双平面左室射血分数; LVEDD: 左心室舒张末期内径; LVPWT: 左心室后壁厚度.
下载: 导出CSV
表 3 三组参与者4DLAQ左房容积参数对比
Table 3. Comparison of 4DLAQ left atrial volume parameters of three groups of participants
参数 对照组(n=36) NLVH组(n=40) LVH组(n=40) H/F P LAVmin(mL) 18.00(15.25, 24.75) 23.63(8.95) 29.50(20.00, 45.25)*# 16.038 < 0.001 LAVmax(mL) 39.50(32.50, 55.00) 46.58(12.64) 50.50(16.85) 4.571 0.102 LAVpreA(mL) 27.00(21.25, 36.50) 35.00(11.63) 39.30(14.58)* 9.300 0.010 LAEF(%) 52.91±10.50 50.16±9.23 37.52±14.47*# 22.326 < 0.001 LAPEF(%) 30.19±13.56 25.62±10.23 22.50±10.61* 4.281 0.016 LAAEF(%) 32.26±9.13 32.76±10.03 18.24±18.52*# 14.950 < 0.001 LAVmin: 左房最小容积; LAVmax: 左房最大容积; LAVpreA: 左房收缩前容积; LAEF: 左房整体射血分数; LAPEF: 左心房被动射血分数; LAAEF: 左心房主动射血分数. *P < 0.05 vs对照组; #P < 0.05 vs NLVH组.
下载: 导出CSV
表 4 三组参与者4DLAQ左房应变参数对比
Table 4. Comparison of 4DLAQ left atrial strain parameters of three groups of participants (%)
参数 对照组(n=36) NLVH组(n=40) LVH组(n=40) H/F P LASr 24.83±3.00 18.70±4.82* 14.30±3.52*# 69.932 < 0.001 LAScd -15.00(-13.25, -18.75) -10.33±4.42* -7.90±3.80* 48.125 < 0.001 LASct -11.25±3.58 -14.00(-11.25, -17.00)* -9.00(-5.00, -10.00)*# 40.002 < 0.001 LASr_c 34.50(30.00, 39.00) 29.00±5.97* 22.98±5.48*# 51.446 < 0.001 LAScd_c -18.00(-15.00, -22.00) -12.33±6.80* -8.00(-4.25, -10.00)*# 52.186 < 0.001 LASct_c -14.00(-12.00, -18.00) -22.63±5.89* -9.53±3.79*# 73.059 < 0.001 LASr: 左房储备期长轴应变; LAScd: 左房管道期长轴应变; LASct: 左房收缩期长轴应变; LASr_c: 左房储备期环形应变; LAScd_c: 左房管道期环形应变; LASct_c: 左房收缩期环形应变. *P < 0.05 vs对照组; #P < 0.05 vs NLVH组.
下载: 导出CSV
表 5 观察者间及观察者内一致性检验
Table 5. Inter observer and intra observer consistency test
参数 观察者间 观察者内 ICC 95% CI ICC 95% CI LAVmin(mL) 0.971 0.832~0.992 0.973 0.798~0.993 LAVmax(mL) 0.989 0.664~0.998 0.990 0.895~0.998 LAVpreA(mL) 0.994 0.982~0.998 0.996 0.983~0.999 LASr_c(%) 0.982 0.912~0.995 0.988 0.932~0.997 LAScd_c(%) 0.989 0.948~0.997 0.994 0.958~0.998 LASct_c(%) 0.986 0.958~0.995 0.988 0.964~0.996 ICC: 组内相关系数.
下载: 导出CSV
-
[1] 张桂珍, 和渝斌, 黄九延, 崔吉君. 高血压病对心脏左心房结构的影响[J]. 高血压杂志, 1999, 7(3): 219-21. doi: 10.3969/j.issn.1673-7245.1999.03.010 [2] Overvad TF, Nielsen PB, Larsen TB, et al. Left atrial size and risk of stroke in patients in sinus rhythm. A systematic review[J]. Thromb Haemost, 2016, 116(2): 206-19. [3] 徐明媛, 欧艳梅, 李丕宇, 等. 四维自动左房定量技术评估原发性高血压病患者左房功能的价值[J]. 临床超声医学杂志, 2022, 24(6): 401-5. https://www.cnki.com.cn/Article/CJFDTOTAL-LCCY202206001.htm [4] Badano LP, Miglioranza MH, Mihăilă S, et al. Left atrial volumes and function by three-dimensional echocardiography: reference values, accuracy, reproducibility, and comparison with twodimensional echocardiographic measurements[J]. Circ Cardiovasc Imaging, 2016, 9(7): e004229. doi: 10.1161/CIRCIMAGING.115.004229 [5] 中国高血压联盟《动态血压监测指南》委员会, 王继光. 2020中国动态血压监测指南[J]. 中国医学前沿杂志: 电子版, 2021, 13(3): 34-51. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGXH202104001.htm [6] Haeusler KG, Huttner HB, Kuramatsu JB. Comment on 2018 ESC/ ESH Guidelines for the management of arterial hypertension[J]. Eur Heart J, 2019, 40(25). [7] Nagueh SF, Smiseth OA, Appleton CP, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: an update from the American society of echocardiography and the European association of cardiovascular imaging[J]. JAm Soc Echocardiogr, 2016, 29(4): 277-314. doi: 10.1016/j.echo.2016.01.011 [8] 刘虹宏, 田国祥, 林运. 心房功能的再认识[J]. 中国循证心血管医学杂志, 2020, 12(10): 1153-5. https://www.cnki.com.cn/Article/CJFDTOTAL-PZXX202010001.htm [9] 张瑞, 朱慧珍, 黄丹青, 等. 四维自动左心房定量分析技术评价原发性高血压患者左心房功能的应用价值[J]. 中华超声影像学杂志, 2021, 30(8): 655-60. [10] Karakurt A, Yildiz C, Yildiz A, et al. Early detection strain/strain rate and time to strain/strain rate abnormalities for left atrial mechanical function in hypertensive patients[J]. Acta Cardiol, 2019, 74(2): 141-51. [11] Ran H, Schneider M, Wan LL, et al. Four-dimensional volume-strain expression in asymptomatic primary hypertension patients presenting with subclinical left atrium-ventricle dysfunction[J]. Cardiology, 2020, 145(9): 578-88. [12] Inaba Y, Yuda S, Kobayashi N, et al. Strain rate imaging for noninvasive functional quantification of the left atrium: comparative studies in controls and patients with atrial fibrillation[J]. J Am Soc Echocardiogr, 2005, 18(7): 729-36. [13] Morris DA, Belyavskiy E, Aravind-Kumar R, et al. Potential usefulness and clinical relevance of adding left atrial strain to left atrial volume index in the detection of left ventricular diastolic dysfunction[J]. JACC Cardiovasc Imaging, 2018, 11(10): 1405-15. [14] Thomas L, Marwick TH, Popescu BA, et al. Left atrial structure and function, and left ventricular diastolic dysfunction[J]. J Am Coll Cardiol, 2019, 73(15): 1961-77. [15] 王玲玲, 张平洋, 董静, 等. 基于彩色多普勒超声四维容积应变技术的原发性高血压病左心室重构患者左心房功能评价[J]. 山东医药, 2021, 61(33): 53-6. https://www.cnki.com.cn/Article/CJFDTOTAL-SDYY202133012.htm [16] 彭红兵, 王春梅, 王秀玲, 等. 2D-STI技术评价原发性高血压患者早期左心房功能的临床研究[J]. 系统医学, 2019, 4(3): 107-10. https://www.cnki.com.cn/Article/CJFDTOTAL-XTYX201903045.htm [17] 刘海兰, 宋嫣, 张芳. 三维斑点追踪技术与实时三维超声心动图对冠心病同步性研究[J]. 中国医学创新, 2019, 16(10): 10-4. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYCX201910005.htm [18] Fei MY, Li M, Ran H, et al. Four-dimensional quantification on left atrial volume-strain in coronary heart disease patients without regional wall motion abnormalities: correlation with the severity of coronary stenosis[J]. Echocardiography, 2022, 39(6): 758-67. [19] Chen LL, Zhang CQ, Wang JT, et al. Left atrial strain measured by 4D Auto LAQ echocardiography is significantly correlated with high risk of thromboembolism in patients with non-valvular atrial fibrillation[J]. Quant Imaging Med Surg, 2021, 11(9): 3920-3. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 177
- HTML全文浏览量: 96
- PDF下载量: 11
- 被引次数: 0