



Effect of intracranial arterial calcification on the clinical prognosis of thrombolytic therapy in patients with acute cerebral infarction
-
摘要:
目的 探讨颅内动脉钙化程度对接受溶栓治疗的急性脑梗死患者临床预后的影响。 方法 回顾性收集接受静脉溶栓治疗的急性前循环脑梗死患者共124例。采用90 d改良Rankin量表,把患者分为预后良好组(n=87)及预后不良组(n=37)。收集患者就诊时完善的颅脑CT,用图像处理软件ImageJ测量责任动脉侧颅内段颈内动脉虹吸段的钙化容积,并收集可能影响患者预后的其他临床指标,进行单因素分析,对影响患者预后的因素进一步应用Logistic回归分析,明确颅内动脉钙化是否为患者预后不良的独立危险因素。最后,计算钙化容积及溶栓前美国国立卫生研究院卒中量表(NIHSS)评分的联合预测因子,采用Medcalc 18.2.1统计软件,绘制溶栓前NIHSS评分的曲线及联合预测因子的ROC曲线,计算两者曲线下面积,比较两种指标间曲线下面积的差异显著性。 结果 钙化容积是接受静脉溶栓治疗的急性前循环脑梗死患者预后不良的独立危险因素(OR=1.10,95%CI=1.05~1.21)。溶栓前NIHSS评分的曲线下面积为0.77,95%CI为0.69~0.85,截点值为5分,敏感度为75.7%,特异性为72.4%;溶栓前NIHSS评分联合钙化容积的曲线下面积为0.83,95%CI为0.75~0.89,敏感度为75.7%,特异性为80.5%。相较于单独应用溶栓前NIHSS评分,联合预测因子对患者预后情况的预测价值更高,两者间差异有统计学意义(Z=2.21,P=0.027)。 结论 钙化容积与急性前循环脑梗死患者溶栓后预后不良独立相关,可以构成判断患者溶栓后预后情况的指标,且溶栓前NIHSS评分联合钙化容积对患者预后情况的预测价值优于单独应用溶栓前NIHSS评分。 Abstract:Objective To investigate the effect of intracranial artery calcification on the clinical prognosis of patients with acute cerebral infarction who received thrombolytic therapy, in order to predict the prognosis positively. Methods A total of 124 patients with acute anterior circulation cerebral infarction were retrospectively collected. The 90-day modified Rankin scale was used to divide the patients into a good prognosis group (n=87) and a poor prognosis group (n=37). We collected the perfect brain CT at the time of the patient's visit, and used the image processing software ImageJ to measure the calcification volume of the siphon segment of the intracranial carotid artery on the side of the responsible artery. Logistic regression analysis was further applied to the factors affecting the prognosis of patients to determine whether intracranial artery calcification was an independent risk factor for poor prognosis of patients. Finally, the combined predictors of the calcification volume and the NIHSS score before thrombolysis were calculated. ROC curve was drawn by the predictor and pre-thrombolysis NIHSS scores, AUCs were calculated, and the significance of the difference in AUC between two indicators was compared. Results Calcified volume was an independent risk factor for patients with acute anterior circulation cerebral infarction treated with intravenous thrombolysis (OR=1.10, 95%CI=1.05-1.21). The pre-thrombolytic NIHSS score showed that AUC was 0.77, 95%CI was 0.69-0.85, cut-off value was 5, sensitivity was 75.7% and specificity was 72.4%. The pre-thrombolytic NIHSS score combined with calcified volume showed that AUC was 0.83, 95% CI was 0.75-0.89, sensitivity was 75.7% and specificity was 80.5%. The combined predictor was more predictive of patient prognosis than the pre-thrombolysis NIHSS score alone (Z=2.21, P=0.027). Conclusion Calcification volume is independently associated with poor prognosis in patients with acute anterior circulation cerebral infarction receiving thrombolysis, which can constitute an indicator for judging the prognosis of patients after thrombolysis. The pre-thrombotic NIHSS score combined with the calcification volume has a better predictive value than the pre-thrombotic NIHSS score alone. -

图 1 颈内动脉钙化容积的计算过程示例
本例为左侧大脑半球脑梗死患者. A:调整窗宽窗位后所示的垂体窝层面处左侧颈内动脉虹吸部;B:调整窗宽窗位后所示的床突层面处左侧颈内动脉虹吸部;C:标记后所示的垂体窝层面处左侧颈内动脉虹吸部半环状钙化灶;D:标记后所示的床突层面处左侧颈内动脉虹吸部(本例所示无钙化灶).
Figure 1. Example of the calculation process of the internal carotid artery calcification volume.

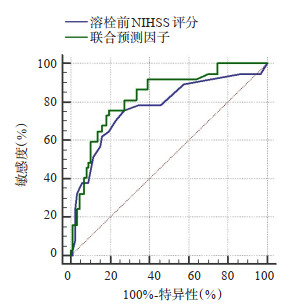
图 2 溶栓前NIHSS评分及联合预测因子预测患者预后情况的ROC曲线
Figure 2. ROC curve of NIHSS score and combined predictors before thrombolysis to predict the prognosis of patients.
表 1 预后良好组和预后不良组患者的基本资料及钙化容积的比较
Table 1. Comparison of basic data and calcification volume between patients with good prognosis and poor prognosis
项目 预后良好组(n=87) 预后不良组(n=37) t/x2/Z P 一般资料 年龄(岁, Mean±SD) 66.75±9.17 71.95±10.59 -2.757 0.007 男性[n(%)] 53(60.9) 25(67.6) 0.492 0.483 BMl(kg/m2)* 25.07(23.30, 27.78) 24.00(22.03, 26.44) -2.007 0.045 吸烟[n(%)] 46(52.9) 19(51.4) 0.024 0.877 钦洒[n(%)] 32(36.8) 18(48.6) 1.519 0.218 发病至溶栓时间(min)* 152.00(109.00, 234.00) 134.00(102.00, 196.00) -1.111 0.266 溶栓前NIHSS评分(分)* 3.00(2.00, 6.00) 11.00(5.50, 15.50) -4.858 <0.001 既往病史及用药史[n(%)] 高血压病 70(80.5) 28(75.7) 0.359 0.549 糖尿病 3(35.6) 16(43.2) 0.639 0.424 脑卒中 18(20.7) 9(24.3) 0.201 0.654 冠心病 9(10.3) 6(16.2) 0.380 0.538 房颤 8(9.2) 1(29.7) 8.436 0.004 既往应用抗凝药物 2(2.3) 3(8.1) 1.012 0.315 既往应用抗板药物 13(14.9) 8(21.6) 0.823 0.364 实验室指标 WBC(109/L, Mean±SD) 7.28±1.84 8.52±2.49 -2.744 0.008 NLR* 2.48(1.93, 3.63) 4.34(2.81, 7.28) -4.055 <0.001 Hb (g/L, Mean±SD) 137.62±19.15 139.95±17.68 -0.633 0.528 Plt(109/L, Mean±SD) 217.10±50.32 192.57±45.00 2.561 0.012 INR* 1.03(0.98, 1.08) 1.09(0.99, 1.16) -2.290 0.022 ALT(U/L)* 15.57(12.73, 20.68) 15.37(11.22, 24.74) -0.175 0.861 ALP (U/L)* 67.00(56.27, 77.10) 63.98(55.92, 78.10) -0.814 0.416 Hcy(μmol/L* 11.12(9.33, 15.57) 12.44(10.08, 16.84) -1.103 0.270 空腹血糖(mmol/L)* 5.94(5.15, 6.96) 6.71(5.57, 9.11) -2.340 0.019 LDL(mmol/L)* 2.76(2.23, 3.23) 2.65(2.13, 3.23) -0.363 0.716 肌酐/尿素氮比值* 13.4(11.15, 6.94) 12.65(9.32, 15.35) -1.625 0.104 UA(μmol/L, Mean±SD) 338.16±84.52 320.03±111.32 0.888 0.379 血磷(mmol/L)* 1.15(1.01, 1.28) 1.02(0.92, 1.17) -3.002 0.003 血钙(mmol/L)* 2.25(2.16, 2.31) 2.21(2.14, 2.28) -1.334 0.182 钙磷乘积(mmol2/L2)* 2.56(2.22, 2.83) 2.30(1.99, 2.59) -3.206 0.001 钙化情况 钙化容积(mm3)* 11.89(0.00, 65.55) 106.16(26.74, 197.09) -4.398 <0.001 *以中位数(四分位数间距)表示. WBC:白细胞计数;NLR:中性粒细胞/淋巴细胞比值;Hb:血红蛋白;Plt:血小板计数;INR:国际标准化比值;ALT:谷丙转氨酶;ALP:碱性磷酸酶;Hcy:同型半胱氨酸;LDL:低密度脂蛋白;UA:尿酸.  下载: 导出CSV
下载: 导出CSV
表 2 预后良好组和预后不良组患者的结局指标的比较
Table 2. Comparison of outcome between patients with good prognosis and poor prognosis
结局指标 预后良好组(n=87) 预后不良组(n=37) Z P 住院时间(d)* 7.00(6.00,7.00) 8.00(7.00,11.00) -5.074 <0.001 出院时NIHSS评分(分)* 1.00(0.00,2.00) 10.00(3.00,12.00) -6.871 <0.001 *以中位数(四分位数间距)表示. NIHSS: 国立卫生研究院卒中量表.
下载: 导出CSV
表 3 患者预后不良影响因素的Logistic回归分析
Table 3. Logistic regression analysis of factors influencing the poor prognosis of patients
因素 P OR OR值的95%CI 钙化容积 0.020 1.10 1.05~1.21 年龄 0.990 1.00 0.94~1.07 BMI 0.215 0.91 0.78~1.06 溶栓前NIHSS评分 0.745 0.98 0.84~1.13 房颤史 0.821 1.20 0.24~5.95 WBC 0.557 1.13 0.75~1.69 NLR 0.427 1.12 0.85~1.48 Pit 0.188 0.99 0.98~1.01 INR 0.127 36.60 0.36 ~3714.01 空腹血糖 0.040 1.29 1.01~1.66 血磷 0.986 0.95 0.000~308.22 钙磷乘积 0.357 0.27 0.02~4.45 NIHSS:国立卫生研究院卒中量表.
下载: 导出CSV
表 4 溶栓前NIHSS评分及溶栓前NIHSS评分联合钙化容积的预测价值分析
Table 4. Predictive value of NIHSS score before thrombolysis and NIHSS score combined with calcification volume before thrombolysis
变量 AUC(95%CI) 敏感度(%) 特异性(%) 约登指数 截点值 溶栓前NIHSS评分 0.77(0.69~0.85) 75.7 72.4 0.48 >5 溶栓前NIHSS评分+转化容积 0.83(0.75~0.89) 75.7 80.5 0.56 -
下载: 导出CSV
-
[1] Roth GA, Mensah GA, Johnson CO, et al. Global burden ofcardiovascular diseases and risk factors, 1990- 2019[J]. J Am Coll Cardiol, 2020, 76(25): 2982-3021. [2] Caprio FZ, Sorond FA. Cerebrovascular disease[J]. Med Clin N Am, 2019, 103(2): 295-308. doi: 10.1016/j.mcna.2018.10.001 [3] Jiang CX, Zhang J, Zhu JB, et al. Association between coexisting intracranial artery and extracranial carotid artery atherosclerotic diseases and ipsilateral cerebral infarction: a Chinese Atherosclerosis Risk Evaluation (CARE- Ⅱ) study[J]. Stroke Vasc Neurol, 2021, 6(4): 595-602. doi: 10.1136/svn-2020-000538 [4] Berliner JA, Navab M, Fogelman AM, et al. Atherosclerosis: basic mechanisms. Oxidation, inflammation, and genetics[J]. Circulation, 1995, 91(9): 2488-96. [5] Koton S, Tashlykov V, Schwammenthal Y, et al. Cerebral artery calcification in patients with acute cerebrovascular diseases: determinants and long- term clinical outcome[J]. Eur J Neurol, 2012, 19(5): 739-45. doi: 10.1111/j.1468-1331.2011.03620.x [6] Bugnicourt JM, Leclercq C, Chillon JM, et al. Presence of intracranial artery calcification is associated with mortality and vascular events in patients with ischemic stroke after hospital discharge: a cohort study[J]. Stroke, 2011, 42(12): 3447-53. doi: 10.1161/STROKEAHA.111.618652 [7] 中华医学会神经病学分会, 中华医学会神经病学分会脑血管病学组, 彭斌, 等. 中国急性缺血性脑卒中诊治指南2018[J]. 中华神经科杂志, 2018, 51(9): 666-82. doi: 10.3760/cma.j.issn.1006-7876.2018.09.004 [8] Rha JH, Saver JL. The impact of recanalization on ischemic stroke outcome: a meta-analysis[J]. Stroke, 2007, 38(3): 967-73. doi: 10.1161/01.STR.0000258112.14918.24 [9] 张佳, 朱海峰, 马运萍. 核磁共振脑灌注成像及DWI联合应用在诊断早期脑梗死缺血半暗带中的临床价值[J]. 卒中与神经疾病, 2018, 25 (3): 252-5. doi: 10.3969/j.issn.1007-0478.2018.03.003 [10] Bartstra JW, van den Beukel TC, Van Hecke W, et al. Intracranial arterial calcification: prevalence, risk factors, and consequences: JACC review topic of the week[J]. J Am Coll Cardiol, 2020, 76 (13): 1595-604. doi: 10.1016/j.jacc.2020.07.056 [11] Madhavan MV, Tarigopula M, Mintz GS, et al. Coronary artery calcification[J]. J Am Coll Cardiol, 2014, 63(17): 1703-14. doi: 10.1016/j.jacc.2014.01.017 [12] 李宏霞, 吕文涛, 赵子霞, 等. 冠状动脉钙化积分对PCI患者临床预后预测价值的研究[J]. 中国当代医药, 2015, 22(13): 60-2. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGUD201513018.htm [13] Hernández- Pérez M, Bos D, Dorado L, et al. Intracranial carotid artery calcification relates to recanalization and clinical outcome after mechanical thrombectomy[J]. Stroke, 2017, 48(2): 342-7. doi: 10.1161/STROKEAHA.116.015166 [14] Tábuas- Pereira M, Sargento- Freitas J, Silva F, et al. Intracranial internal carotid artery wall calcification in ischemic strokes treated with thrombolysis[J]. Eur Neurol, 2018, 79(1-2): 21-6. doi: 10.1159/000477901 [15] de Weert TT, Cakir H, Rozie S, et al. Intracranial internal carotid artery calcifications: association with vascular risk factors and ischemic cerebrovascular disease[J]. AJNR Am J Neuroradiol, 2009, 30(1): 177-84. doi: 10.3174/ajnr.A1301 [16] Kassab MY, Gupta R, Majid A, et al. Extent of intra- arterial calcification on head CT is predictive of the degree of intracranial atherosclerosis on digital subtraction angiography[J]. Cerebrovasc Dis, 2009, 28(1): 45-8. doi: 10.1159/000219296 [17] Woodcock RJ Jr, Goldstein JH, Kallmes DF, et al. Angiographic correlation of CT calcification in the carotid siphon[J]. AJNR Am J Neuroradiol, 1999, 20(3): 495-9. [18] 惠鑫, 张利军, 陈旺, 等. 颅内动脉钙化与缺血性脑卒中关系的研究进展[J]. 中华神经医学杂志, 2020, 19(9): 902-8. doi: 10.3760/cma.j.cn115354-20200312-00181 [19] Wu XH, Chen XY, Fan YH, et al. High extent of intracranial carotid artery calcification is associated with downstream microemboli in stroke patients[J]. J Stroke Cerebrovasc Dis, 2017, 26(2): 442-7. [20] Lee SJ, Lee IK, Jeon JH. Vascular calcification-new insights into its mechanism[J]. Int J Mol Sci, 2020, 21(8): 2685. doi: 10.3390/ijms21082685 [21] Zhang F, Yang L, Gan L, et al. Spotty calcium on cervicocerebral computed tomography angiography associates with increased risk of ischemic stroke[J]. Stroke, 2019, 50(4): 859-66. doi: 10.1161/STROKEAHA.118.023273 [22] Chung PW, Park KY, Kim JM, et al. Carotid artery calcification is associated with deep cerebral microbleeds[J]. Eur Neurol, 2014, 72 (1/2): 60-3. [23] Compagne KCJ, Clephas PRD, Majoie CBLM, et al. Intracranial carotid artery calcification and effect of endovascular stroke treatment[J]. Stroke, 2018, 49(12): 2961-8. -

 点击查看大图
点击查看大图

计量
- 文章访问数: 348
- HTML全文浏览量: 114
- PDF下载量: 4
- 被引次数: 0