



Clinical effect of percutaneous transluminal coronary intervention in the treatment of very elderly patients with acute coronary syndrome with multivessel disease under the guidance of quantitative flow ratio
-
摘要:
目的 探究定量血流分数(QFR)指导下经皮腔内冠状动脉介入(PCI)治疗伴多支血管病变超高龄急性冠状动脉综合征(ACS)患者的临床效果。 方法 选取2019年3月~2020年4月在我院接受治疗并符合纳入标准拟行急性冠状动脉综合征超高龄患者(90~110岁)80例为研究对象,根据患者意愿分为研究组及对照组,40例/组。对照组采用单纯冠状动脉造影诊断PCI手术治疗;研究组采用QFR指导PCI。检测术前及术后1月患者血浆脑利钠肽、氨基末端B型利钠肽前体、心肌肌钙蛋白I水平,心脏功能指标(左心室射血分数、左心室舒张末期内径、左心室收缩末期内径、射血分数)、纽约心脏病协会分级变化及不良事件发生情况。 结果 研究组冠状动脉造影血管直径狭窄程度≥50%共83支,其中QFR≤0.8阳性43支(51.81%),阴性40支(48.19%),其中阳性41支、阴性7支行PCI联合冠状动脉旁路移植术治疗,与QFR分析结果相符率分别为95.35%、82.50%;对照组冠状动脉造影血管直径狭窄程度≥50%共79支,其中70支病变血管行PCI联合冠状动脉旁路移植术治疗。术后1月研究组血浆脑利钠肽、氨基末端B型利钠肽前体水平、左心室收缩末期内径、左心室舒张末期内径均低于对照组,射血分数值高于对照组(P < 0.05);研究组术后1月内不良事件发生率低于对照组(27.50% vs 50.00%,P < 0.05)。 结论 QFR指导外科PCI手术治疗超高龄多支血管病变的急性冠状动脉综合征安全可行,可降低术后不良事件发生率,但其有效性仍需进一步扩大样本和进行前瞻性临床研究验证。 -
关键词:
- 定量血流分数 /
- 经皮腔内冠状动脉介入 /
- 急性冠状动脉综合征 /
- 超高龄
Abstract:Objective To explore the clinical effects of percutaneous transluminal coronary intervention (PCI) under the guidance of quantitative blood flow fraction (QFR) in the treatment of very elderly patients with acute coronary syndrome with multivessel disease. Methods Eighty super-aged patients who were treated in our hospital from March 2019 to April 2020 and met the inclusion criteria and planned to undergo acute coronary syndrome were selected as the research objects. They were divided into observation group and control group, with 40 cases in each group. The control group used coronary angiography alone to diagnose PCI surgery. The observation group used QFR to guide PCI. The plasma brain natriuretic peptide, NT-proBNP, cardiac troponin I levels, changes in cardiac function indicators before and after surgery (left ventricular ejection fraction, left ventricular end diastolic diameter, left ventricular end systolic diameter, ejection fraction), NYHA grading changes and adverse events were detected. Results The observation group had 83 coronary angiography vessel diameter stenosis≥50%, of which 43 were positive for QFR≤0.8 (51.81%) and 40 were negative (48.19%). Among them, 41 positive and 7 negative were treated with PCI combined with coronary artery revascularization surgery, which was consistent with the results of QFR analysis. The rates were 95.35% and 82.50%, respectively. The control group had 79 vessels with coronary angiography vessel diameter stenosis≥50%, 70 of which were treated with PCI combined with coronary artery revascularization. The plasma brain natriuretic peptide of the observation group was 1 month after the operation. The levels of NT- proBNP, left ventricular end systolic diameter and left ventricular end diastolic diameter were significantly lower than those of the control group, and the ejection fraction value was higher than that of the control group (P < 0.05). The adverse event rate of 27.50% (n=11) in observation group was significantly lower than that of control group within 1 month after surgery 50.00% (n=20, P < 0.05). Conclusion Quantitative blood flow scores are safe and feasible to guide surgical percutaneous coronary intervention in the treatment of acute coronary syndrome in very elderly patients with multivessel disease. It can reduce the incidence of postoperative adverse events. However, its effectiveness still needs to be further expanded and validated by prospective clinical studies. -

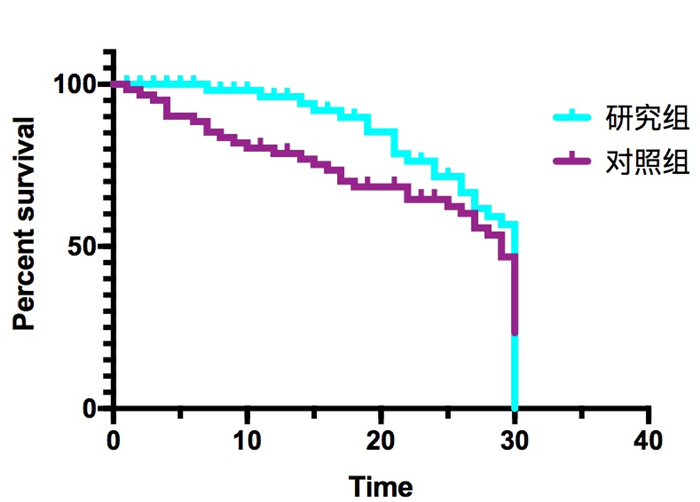
图 1 两组患者预后不良事件的Kaplan-Meier分析
Figure 1. Kaplan-Meier analysis of adverse events in the prognosis of patients in the two groups.
表 1 两组患者一般资料比较
Table 1. Comparison of general data of the two groups of patients[n=40, n (%)]
指标 研究组 对照组 χ2/t P 性別(男/女,n) 21/19 18/22 0.450 0.502 年龄(岁, Mean±SD) 99.52±6.56 100.04±7.03 0.342 0.733 BMI(kg/m2, Mean±SD) 25.03±3.54 25.11±3.03 0.109 0.914 发病至人院时间(h,Mean±SD) 12.63±5.56 11.93±6.08 0.537 0.593 主要冠心病史 1.147 0.563 冠状动脉性心脏病 16(40.00) 14(35.00) 原发瓣膜性心脏病 17(42.50) 15(37.50) 肥厚型梗阻性心肌病 3(7.50) 6(15.00) 大血管病 2(5.00) 4(10.00) 先天性心脏病 2(5.00) (2.50) 合并病史 PCI治疗史 29(72.50) 30(75.00) 0.065 0.799 高血压 34(85.00) 32(80.00) 0.346 0.556 糖尿病 18(45.00) 2(52.50) 0.450 0.502 吸烟史 20(50.00) 15(37.50) 1.270 0.260 钦洒史 25(62.50) 23(57.50) 0.208 0.648 PCI:经皮冠状动脉介入治疗.  下载: 导出CSV
下载: 导出CSV
表 2 研究组QFR分析
Table 2. QFR analysis of study groups[n(%)]
指标 CAG≥50% QFR≤0.8 病变血管的狭窄程度(目测法) 50%~69% 39(46.99) 9/39(23.08) 70%~89% 30(36.14) 20/30(66.67) 90%以上 14(16.87) 14/14(100%) 病变血管区域 前降支 32(38.55) 22/32(68.75) 回旋支 22(26.51) 14/22(63.64) 右冠状动脉 29(34.94) 7/29(24.14)
下载: 导出CSV
表 3 两组患者术前及手术1月后血液及心脏功能指标比较
Table 3. Comparison of blood and cardiac function indexes between the two groups of patients before surgery and 1 month after surgery (n=40, Mean±SD)
指标 研究组 对照组 术前χ2/t P 术后χ2/t P 术前 术后1月 术前 术后1月 BNP(pg/L) 587.32±90.28 235.16±77.29 570.09±92.31 272.05±80.01 0.844 0.401 2.268 0.026 NT-proBNP(ng/L) 803.10±82.23 287.21±80.07 794.50±79.77 352.71±94.28 0.475 0.636 3.349 0.001 心肌肌钙蛋白I(ng/mL) 0.05±0.03 0.12±0.10 0.05±0.02 0.15±0.09 0.000 1 1.410 0.162 左心室射血分数(%) 41.70±3.55 46.21±2.79 40.91±3.64 45.20±2.92 0.983 0.329 1.582 0.118 左心室收缩末期内径(mm) 48.50±3.15 44.15±2.78 48.35±2.90 45.90±2.27 0.222 0.825 3.084 0.003 左心室舒张末期内径(mm) 50.35±2.40 41.35±1.75 50.15±2.30 42.70±2.00 0.381 0.705 3.213 0.002 射血分数(%) 63.52±11.21 74.36±12.08 64.07±12.11 73.08±11.00 0.211 0.834 0.496 0.622 纽约心脏病协会分级[n(%)] 0.052 0.820 3.731 0.053 Ⅰ~Ⅱ级 17(42.50) 29(72.50) 16(40.00) 20(50.00) Ⅲ~Ⅳ级 23(57.50) 8(20.00) 24(60.00) 15(37.50) BNP:脑利钠肽;NT-proBNP:氨基末端B型利钠肽前体.
下载: 导出CSV
表 4 两组患者预后不良事件的Kaplan-Meier分析
Table 4. Kaplan-Meier analysis of prognostic adverse events in the two groups of patients[n=40, n(%)]
分组 心肌梗死 脑卒中 死亡 新发肾衰 总发生率(%) χ2 P 研究组 4(10.00) 2(5.00) 3(7.50) 2(5.00) 27.50 4.266 0.039 对照组 8(20.00) 3(7.50) 5(12.50) 4(10.00) 50.00
下载: 导出CSV
-
[1] 胡盛寿, 高润霖, 刘力生, 等. 《中国心血管病报告2018》概要[J]. 中国循环杂志, 2019, 34(3): 209-20. doi: 10.3969/j.issn.1000-3614.2019.03.001 [2] 李东枝, 侯永超, 张晓红, 等. 急性冠状动脉综合征患者确诊前症状体验的质性研究[J]. 中国实用护理杂志, 2021, 37(29): 2261-7. [3] 谢志江, 李敏, 程瑞丽, 等. 血清MDA-LDL、ALP与急性冠脉综合征患者PCI术后不良心血管事件的关系[J]. 国际检验医学杂志, 2021, 42(22): 2729-34. doi: 10.3969/j.issn.1673-4130.2021.22.009 [4] 张瑞涛, 徐昕晔, 何立芸, 等. 瞬时无波形比值和定量血流分数评价冠状动脉临界病变准确性的对比研究[J]. 中国介入心脏病学杂志, 2021, 29(3): 148-53. doi: 10.3969/j.issn.1004-8812.2021.03.007 [5] 中华医学会, 中华医学会杂志社, 中华医学会全科医学分会, 等. 非ST段抬高型急性冠状动脉综合征基层诊疗指南(2019年)[J]. 中华全科医师杂志, 2021, 20(1): 6-13. doi: 10.3760/cma.j.cn114798-20201030-01112 [6] 王静, 周云英. 急性心肌梗死急诊PCI术后护理风险预警模型的构建与应用[J]. 介入放射学杂志, 2021, 30(2): 196-200. doi: 10.3969/j.issn.1008-794X.2021.02.020 [7] 赵娟, 涂腾灿, 杨梅君, 等. 急性冠状动脉综合征患者早期冠状动脉病变的评估[J]. 昆明医科大学学报, 2021, 42(12): 47-50. doi: 10.12259/j.issn.2095-610X.S20211219 [8] 陈晓杰, 于洁, 谢宇端, 等. 血管内超声显像在经皮冠状动脉介入治疗冠心病左主干病变中的应用价值[J]. 中西医结合心脑血管病杂志, 2021, 19(4): 650-2. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYYY202104032.htm [9] Timbadia D, Ler A, Sazzad F, et al. FFR- guided versus coronary angiogram- guided CABG: a review and meta- analysis of prospective randomized controlled trials[J]. J Cardiac Surg, 2020, 35(10): 2785-93. doi: 10.1111/jocs.14880 [10] Tian X, Tang Z. A comparison of fractional flow reserve determination and coronary angiography results in patients with unstable angina and analysis of related factors[J]. J Thorac Dis, 2019, 11(2): 549- 56. doi: 10.21037/jtd.2019.01.20 [11] 刘莉莉, 沈迎, 涂圣贤, 等. 慢性完全闭塞病变行经皮冠状动脉介入治疗对供血动脉定量血流分数的影响[J]. 中国介入心脏病学杂志, 2021, 29(3): 133-7. doi: 10.3969/j.issn.1004-8812.2021.03.004 [12] 陈晓会, 闫兆红, 闫冰, 等. 瞬时无波形比率(iFR)、微循环阻力指数(IMR)和血流储备分数(FFR)在诊断冠状动脉功能性狭窄中的应用[J]. 中国实验诊断学, 2020, 24(5): 870-3. doi: 10.3969/j.issn.1007-4287.2020.05.045 [13] 陈聪, 赵洋, 张魁, 等. 定量血流分数临床研究进展及应用[J]. 中华胸心血管外科杂志, 2021, 37(1): 59-62. doi: 10.3760/cma.j.cn112434-20200820-00380 [14] 柳杨, 田峰, 荆晶, 等. 三维定量冠脉造影在冠心病介入治疗中的作用综述[J]. 解放军医学院学报, 2019, 40(7): 695-8. doi: 10.3969/j.issn.2095-5227.2019.07.023 [15] 高瑜, 蔡兴赳, 方小丽. 急性冠状动脉综合征超高龄伴多支血管病变患者经皮冠状动脉介入治疗不同策略的疗效对比[J]. 中国心血管病研究, 2018, 16(5): 438-41. doi: 10.3969/j.issn.1672-5301.2018.05.015 [16] 叶绍东, 吴永健, 李琳, 等. 75岁以上ST段抬高心肌梗死患者再灌注治疗进展[J]. 中华老年心脑血管病杂志, 2015, 17(4): 436-7. doi: 10.3969/j.issn.1009-0126.2015.04.030 [17] 朱云鹏, 朱嘉希, 张嵬, 等. 定量血流分数指导冠状动脉外科血运重建的研究[J]. 上海交通大学学报: 医学版, 2020, 40(7): 937-42, 936. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 155
- HTML全文浏览量: 140
- PDF下载量: 2
- 被引次数: 0