



Value of miR-3934 combined with MRI to assess the benefit of simultaneous radiotherapy for stage IIB~III cervical cancer
-
摘要:
目的 探究微小核糖核酸-3934(miR-3934)联合MRI评估ⅡB~Ⅲ期宫颈癌同步放化疗获益的价值。 方法 选取2019年8月~2021年9月在华北理工大学附属医院确诊的142例ⅡB~Ⅲ期宫颈癌患者作为研究对象,给予同步放化疗,并根据治疗获益情况将其分为获益组(n = 67)和非获益组(n = 75)。通过实时荧光定量PCR法检测miR-3934水平;采用ROC曲线评价miR-3934判断ⅡB~Ⅲ期宫颈癌同步放化疗获益的价值;采用Logistic回归分析ⅡB~Ⅲ期宫颈癌同步放化疗获益的风险因素,并构建风险因素的列线图回归模型;采用一致性指数、校准曲线和决策曲线分析法评价模型价值。 结果 获益组同步放化疗前(t0)、第2天(t1)和第8天(t2)的miR-3934水平均低于非获益组(P < 0.05);两组的miR-3934水平随时间进展均呈降低趋势,获益组和非获益组t2时点的miR-3934水平均低于t0(P < 0.05)。获益组的回流速率常数值、容积转运常数(Ktrans)值和血管外细胞外间隙容积比值均低于非获益组(P < 0.05),表观弥散系数(ADC)值高于非获益组(P < 0.05)。t2时点的miR-3934判断ⅡB~Ⅲ期宫颈癌同步放化疗获益的ROC曲线下面积高于t0和t1(P < 0.05)。国际妇产科联盟(FIGO)Ⅲ期、淋巴结转移、分化程度低、t2时点的miR-3934> 2.66和Ktrans值>0.59是ⅡB~Ⅲ期宫颈癌同步放化疗的独立危险因素(P < 0.05),ADC值>0.52是ⅡB~Ⅲ期宫颈癌同步放化疗的独立保护因素(P < 0.05)。模型A(由FIGO分期、淋巴结转移、分化程度、Ktrans值和ADC值组成)的一致性指数为0.969,低于模型B(由FIGO分期、淋巴结转移、分化程度、t2时点的miR-3934、Ktrans值和ADC值组成,0.986)。模型A的均方误差和平均绝对误差均低于模型B。当阈值概率在0.88~0.92时,模型A的临床应用价值大于模型B;当阈值概率在0~0.88或0.92~1.00时,模型B的临床应用价值大于模型A。 结论 由FIGO分期、淋巴结转移、分化程度、t2时点的miR-3934、Ktrans值和ADC值组成的模型B评估ⅡB~Ⅲ期宫颈癌同步放化疗获益的价值较高,可辅助医生决策。 Abstract:Objective To investigate the value of microRNA-3934 (miR-3934) combined with MRI to assess the benefit of concurrent chemoradiotherapy in stage IIB~III cervical cancer. Methods A total of 142 patients with stage IIB~III cervical cancer diagnosed at the Affiliated Hospital of North China University of Technology from August 2019 to September 2021 were selected as the study subjects, given concurrent chemoradiotherapy and divided into the benefit group (n = 67) and non-beneficiary group (n = 75) according to the treatment benefit. The miR-3934 level was detected by real-time fluorescent quantitative PCR. Receiver operating characteristic (ROC) curve was used to evaluate the value of miR-3934 in determining the benefit of concurrent chemoradiotherapy for stage IIB~III cervical cancer. Logistic regression was used to analyze the risk factors for the benefits of concurrent chemoradiotherapy in stage IIB~III cervical cancer, and nomogram regression model of risk factors was constructed. The consistency index, calibration curve and decision curve analysis were used to evaluate the value of the model. Results The miR-3934 levels in the beneficiary group were lower than in the non-beneficiary group before (t0), on day 2th (t1) and on day 8th (t2) of concurrent chemoradiotherapy (2.71±0.30 vs 3.05±0.40, 2.64±0.28 vs 2.97±0.35, 2.44± 0.24 vs 2.91±0.36, P < 0.05). The miR-3934 levels in both groups tended to decrease with time progression, and miR-3934 levels at time point t2 were lower than t0 in both the benefit and non-benefit groups (P < 0.05). The values of reflux rate constant, volume transfer constant (Ktrans) and extravascular extracellular gap volume ratio in the beneficiary group were lower than those in the non-beneficiary group [(1.17±0.11)/min vs (1.22±0.11)/min, (0.50±0.15)/min vs (0.67±0.12)/min, (0.37±0.09)% vs (0.47±0.12)%, P < 0.05], and the apparent diffusion coefficient (ADC) value was higher than that in the non-beneficiary group [(0.55±0.06)×10-3 mm2/s vs (0.48±0.07)×10-3 mm2/s, P < 0.05]. The miR-3934 at time point t2 determined the benefit of synchronous radiotherapy for stage IIB~III cervical cancer under the ROC curve area was higher than t0 and t1 (P < 0.05). International Federation of Gynecology and Obstetrics (FIGO) stage III, lymph node metastasis, low differentiation, miR-3934>2.66 at t2 and Ktrans>0.59 were independent risk factors for concurrent chemoradiotherapy of stage IIB~III cervical cancer(P < 0.05). ADC>0.52 was an independent protective factor for concurrent chemoradiotherapy of stage IIB~III cervical cancer (P < 0.05). The C-index of model A (consisting of FIGO staging, lymph node metastasis, differentiation, Ktrans and ADC) was 0.969, which was lower than that of model B (consisting of FIGO staging, lymph node metastasis, differentiation, miR-3934 at t2, Ktrans and ADC, 0.986). The mean square error and mean absoluteerror of model A were 0.00046 and 0.02, respectively, which were lower than those of model B (0.00098 and 0.03). When the threshold probability was 0.88~0.92, the clinical application value of model A was greater than that of model B. When the threshold probability was 0~0.88 or 0.92~1.00, the clinical application value of model B was greater than that of model A. Conclusion Model B consisting of FIGO stage, lymph node metastasis, differentiation, miR-3934 at t2, Ktrans and ADC has high value in assessing the benefits of concurrent chemoradiotherapy for stage IIB~III cervical cancer, which can assist physicians in decision making. -
Key words:
- miR-3934 /
- MRI /
- stage IIB~III cervical cancer /
- concurrent chemoradiotherapy
-

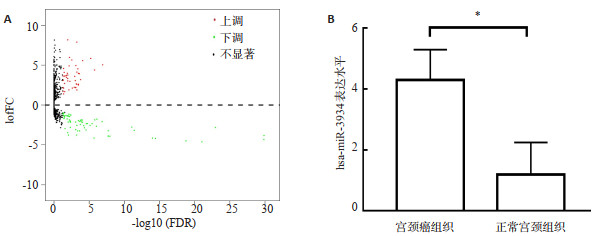
图 2 TCGA-CESC差异miRNAs表达结果
A:CESC中miRNAs表达结果;B:宫颈癌组织和正常宫颈组织中hsa-miR-3934表达水平比较. *P<0.05.
Figure 2. Results of differential miRNAs expression in TCGA-CESC.

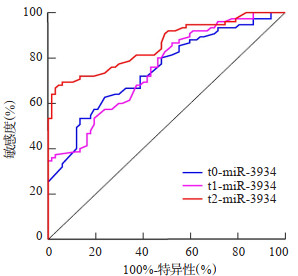
图 3 miR-3934判断ⅡB~Ⅲ期宫颈癌同步放化疗获益的ROC曲线
Figure 3. ROC curve of miR-3934 in judging the benefit of concurrent chemoradiotherapy for stage IIB~III cervical cancer.

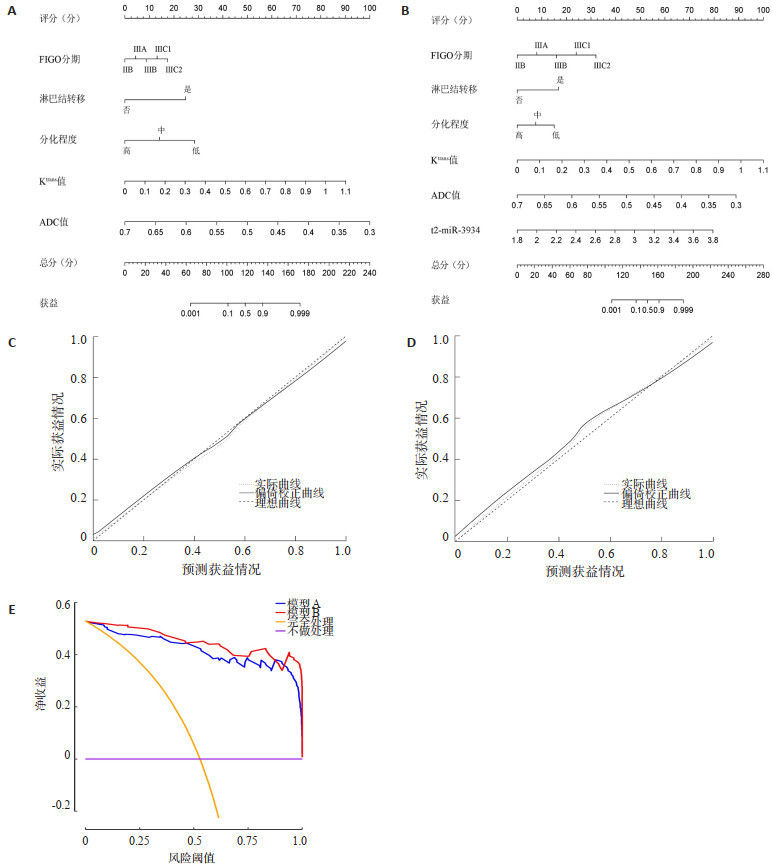
图 4 ⅡB~Ⅲ期宫颈癌同步放化疗获益的模型构建及评价
A:列线图回归模型A; B:列线图回归模型B; C:模型A的校准曲线; D:模型B的校准曲线; E:模型A和模型B的决策曲线分析结果.
Figure 4. Model construction and evaluation of the benefit of concurrent chemoradiotherapy for stage IIB~III cervical cancer.
表 1 两组的临床特征比较
Table 1. Comparison of clinical characteristics of the two groups
临床特征 获益组(n=67) 非获益组(n=75) t/χ2 P 年龄(岁,Mean±SD) 55.06±8.06 54.36±8.06 0.517 0.606 BMI(kg/m2,Mean±SD) 23.41±2.58 23.40±2.49 0.020 0.984 FIGO分期(n) 23.794 < 0.001 ⅡB 26 4 Ⅲ 41 71 淋巴结转移(n) 48.285 < 0.001 是 2 43 否 65 32 病理类型(n) 0.537 0.464 腺癌 16 22 鳞状细胞癌 51 53 肿瘤直径(cm,Mean±SD) 5.43±0.91 5.55±0.93 0.775 0.439 分化程度(n) 23.267 < 0.001 低分化 3 26 中分化 24 27 高分化 40 22 FIGO:国际妇产科联盟.  下载: 导出CSV
下载: 导出CSV
表 2 两组的miR-3934水平比较
Table 2. Comparison of miR-3934 in the two groups (Mean±SD)
组别 t0-miR-3934 t1-miR-3934 t2-miR-3934 获益组(n=67) 2.71±0.30* 2.64±0.28* 2.44±0.24*#& 非获益组(n=75) 3.05±0.40 2.97±0.35# 2.91±0.36# *P < 0.05 vs非获益组同时点;#P < 0.05 vs t0时点;&P < 0.05 vs t1时点.
下载: 导出CSV
表 3 两组的影像学参数比较
Table 3. Comparison of imaging parameters between the two groups(Mean±SD)
分组 Kep值(/min) Ktrans值(/min) Ve值(%) ADC值(×10-3 mm2/s) 获益组(n=67) 1.17±0.11 0.50±0.15 0.37±0.09 0.55±0.06 非获益组(n=75) 1.22±0.11 0.67±0.12 0.47±0.12 0.48±0.07 t 3.020 7.729 5.265 6.012 P 0.003 < 0.001 < 0.001 < 0.001 ADC:表观弥散系数.
下载: 导出CSV
表 4 miR-3934判断ⅡB~Ⅲ期宫颈癌同步放化疗获益的价值比较
Table 4. Comparative value of miR-3934 in determining the benefit of concurrent chemoradiotherapy for stage IIB~III cervical cancer
指标 AUC值 95% CI 最佳截断点 敏感度(%) 特异性(%) t0-miR-3934 0.747 0.667~0.826 2.97 53.33 86.57 t1-miR-3934 0.751 0.673~0.829 3.10 34.67 100.00 t2-miR-3934 0.857 0.796~0.918 2.80 66.67 97.01 AUC:曲线下面积.
下载: 导出CSV
表 5 变量赋值
Table 5. Variable assignment
变量 赋值 FIGO分期 ⅡB期=0,Ⅲ期=1 淋巴结转移 否=0,是=1 分化程度 高分化=0,中分化=1,低分化=2 t2-miR-3934 ≤2.66=0,>2.66=1 Kep值(/min) ≤1.16=0,>1.16=1 Ktrans值(/min) ≤0.59=0,>0.59=1 Ve值 ≤0.42=0,>0.42=1 ADC值(×10-3 mm2/s) ≤0.52=0,>0.52=1 获益 是=0,否=1
下载: 导出CSV
表 6 ⅡB~Ⅲ期宫颈癌同步放化疗获益的logistic回归分析结果
Table 6. Logistic regression analysis results of benefits of concurrent chemoradiotherapy for stage IIB~III cervical cancer
变量 β SE Wald P OR(95%CI) FIGO分期 2.610 0.908 8.270 0.004 13.600(2.296~80.558) 淋巴结转移 2.997 1.092 7.529 0.006 20.035(2.355~170.460) 分化程度 0.927 0.458 4.100 0.043 2.526(1.030~6.195) t2-miR-3934 2.064 0.716 8.308 0.004 7.880(1.936~32.072) Kep 0.610 0.624 0.957 0.328 1.841(0.542~6.249) Ktrans 2.195 0.638 11.835 0.001 8.984(2.572~31.379) Ve 0.214 0.645 0.111 0.739 1.239(0.350~4.382) ADC -2.243 0.790 8.058 0.005 0.106(0.023~0.499)
下载: 导出CSV
-
[1] Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2018, 68(6): 394-424. doi: 10.3322/caac.21492 [2] Torre LA, Siegel RL, Ward EM, et al. Global cancer incidence and mortality rates and trends: an update[J]. Cancer Epidemiol Biomarkers Prev, 2016, 25(1): 16-27. doi: 10.1158/1055-9965.EPI-15-0578 [3] 郑小敏, 董江宁, 钱立庭. IVIM-DWI与DCE-MRI在局部晚期宫颈癌同步放化疗疗效评价中的研究进展[J].国际医学放射学杂志, 2020, 43(3): 322-5. https://www.cnki.com.cn/Article/CJFDTOTAL-GWLC202003017.htm [4] Sadri Nahand J, Moghoofei M, Salmaninejad A, et al. Pathogenic role of exosomes and microRNAs in HPV-mediated inflammation and cervical cancer: a review[J]. Int J Cancer, 2020,146(2): 305-20. doi: 10.1002/ijc.32688 [5] Yerukala Sathipati S, Ho SY. Identifying the miRNA signature associated with survival time in patients with lung adenocarcinoma using miRNA expression profiles[J]. Sci Rep, 2017, 7(1): 7507. doi: 10.1038/s41598-017-07739-y [6] Ye W, Liang FL, Ying C, et al. Downregulation of microRNA- 3934-5p induces apoptosis and inhibits the proliferation of neuroblastoma cells by targeting TP53INP1[J]. Exp Ther Med, 2019, 18(5): 3729-36. [7] Fu CY, Zhang Q, Wang AN, et al. EWI-2 controls nucleocytoplasmic shuttling of EGFR signaling molecules and miRNA sorting in exosomes to inhibit prostate cancer cell metastasis[J]. Mol Oncol, 2021, 15(5): 1543-65. doi: 10.1002/1878-0261.12930 [8] Schernberg A, Kumar T, Achkar S, et al. Incorporating magnetic resonance imaging (MRI) based radiation therapy response prediction into clinical practice for locally advanced cervical cancer patients[J]. Semin Radiat Oncol, 2020, 30(4): 291-9. doi: 10.1016/j.semradonc.2020.05.007 [9] Bhatla N, Denny L. FIGO cancer report 2018[J]. Int J Gynaecol Obstet, 2018,143(Suppl 2): 2-3. [10] Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1)[ J]. Eur J Cancer, 2009, 45(2): 228-47. doi: 10.1016/j.ejca.2008.10.026 [11] 何陈伟, 陈亚君, 邹靖, 等.动态对比增强磁共振成像在局部晚期宫颈癌同步放化疗效果评估中的价值[J].分子影像学杂志, 2021, 44(1): 74-7. doi: 10.12122/j.issn.1674-4500.2021.01.14 [12] Cosper PF, McNair C, González I, et al. Decreased local immune response and retained HPV gene expression during chemoradiotherapy are associated with treatment resistance and death from cervical cancer[J]. Int J Cancer, 2020,146(7): 2047-58. doi: 10.1002/ijc.32793 [13] Matsuo K, Machida H, Mandelbaum RS, et al. Validation of the 2018 FIGO cervical cancer staging system[J]. Gynecol Oncol, 2019,152(1): 87-93. doi: 10.1016/j.ygyno.2018.10.026 [14] Xiao Y, Ren YK, Cheng HJ, et al. Modified Glasgow prognostic score is an independent prognostic factor in patients with cervical cancer undergoing chemoradiotherapy[J]. Int J Clin Exp Pathol, 2015, 8(5): 5273-81. [15] Lima GM, Matti A, Vara G, et al. Prognostic value of posttreatment 18F-FDG PET/CT and predictors of metabolic response to therapy in patients with locally advanced cervical cancer treated with concomitant chemoradiation therapy: an analysis of intensity- and volume-based PET parameters[J]. Eur J Nucl Med Mol Imaging, 2018, 45(12): 2139-46. doi: 10.1007/s00259-018-4077-1 [16] 张禹, 张茜, 张雪健, 等. 3.0T动态对比增强MRI定量参数在鉴别FIGOⅡ期宫颈癌宫旁浸润中的应用价值[J].临床放射学杂志, 2018, 37(7): 1163-7. https://www.cnki.com.cn/Article/CJFDTOTAL-LCFS201807026.htm [17] Simonsen TG, Lund KV, Hompland T, et al. DCE-MRI-derived measures of tumor hypoxia and interstitial fluid pressure predict outcomes in cervical carcinoma[J]. Int J Radiat Oncol Biol Phys, 2018,102(4): 1193-201. doi: 10.1016/j.ijrobp.2018.04.035 [18] Liu B, Sun Z, Ma WL, et al. DCE-MRI quantitative parameters as predictors of treatment response in patients with locally advanced cervical squamous cell carcinoma underwent CCRT[J]. Front Oncol, 2020, 10: 585738. doi: 10.3389/fonc.2020.585738 [19] Meng J, Liu SL, Zhu LJ, et al. Texture Analysis as Imaging Biomarker for recurrence in advanced cervical cancer treated with CCRT[J]. Sci Rep, 2018, 8(1): 11399. doi: 10.1038/s41598-018-29838-0 [20] Meng YF, Chu T, Lin ST, et al. Clinicopathological characteristics and prognosis of cervical cancer with different histological types: a population-based cohort study[J]. Gynecol Oncol, 2021,163(3): 545-51. doi: 10.1016/j.ygyno.2021.10.007 [21] Ren AJ, Wen ZZ, Zheng LJ. Downregulation of miR-3934-5p enhances A549 cell sensitivity to cisplatin by targeting TP53INP1 [J]. Exp Ther Med, 2019, 18(3): 1653-60. -

 点击查看大图
点击查看大图

计量
- 文章访问数: 157
- HTML全文浏览量: 90
- PDF下载量: 6
- 被引次数: 0