



Establishment of diffusion tensor imaging in cervical nerve root ROI outline method and analysis of clinical relevance
-
摘要:
目的 建立可靠的颈神经根感兴趣区(ROI)勾画方法,并对其临床相关性进行验证。 方法 选取20例健康志愿者和20例单节段神经型颈椎病患者,由2名影像科医师应用4种ROI勾画方法,分别测量健康志愿者双侧颈5~8神经根的各向异性分数(FA)值和表观弥散系数(ADC)值,以及患者的患侧病变节段和健侧相应神经根FA值和ADC值,确定一致性最好的颈神经根ROI勾画方法,同时记录每位受试者的年龄、性别、BMI以及患者的VAS评分和ISNCSCI评分,然后采用最佳方法测量得到的弥散张量成像值,分析其临床特征相关性。 结果 最大圆法的一致性最佳;健康者颈神经根FA值与ADC值与患者健侧颈神经根FA值和ADC值差异无统计学意义(P>0.05),与患侧颈神经根FA值和ADC值,差异有统计学意义(P < 0.05);患者健康侧FA值和ADC值与患侧差异有统计学意义(P < 0.05);对于健康志愿者,测得FA值与ADC值,与年龄有相关性(P < 0.05),年龄越大,FA值越小,ADC值越大,但是与BMI无相关性;对于患者,VAS评分与患侧ADC值呈正相关(P < 0.05),与患侧FA/患侧ADC比值呈负相关(P < 0.05),ISNCSCI评分与患侧FA值呈正相关(P < 0.05)。 结论 最大圆ROI勾画方法是可靠的颈神经根弥散张量成像测量方法;患者神经根性痛越明显,则ADC值越大,FA/患侧ADC比值越小;颈椎神经功能越好,则FA值越大。 Abstract:Objective To establish a reliable method for the region-of-interest (ROI) mapping of cervical nerve roots and to verify its clinical relevance. Methods Twenty healthy volunteers and 20 patients with single-segment neurological cervical spondylopathy were selected. Four ROI mapping methods were applied by two imaging physicians to measure the fractional anisotropy (FA) and apparent diffusion coefficient (ADC) values of bilateral cervical 5-8 nerve roots in healthy volunteers as well as the FA and ADC values of the corresponding nerve roots on the affected lesioned segment and the healthy side of the patient to determine the best consistent method for the ROI mapping of the cervical nerve roots, while recording each subject's age, gender, BMI, the patient's VAS score and ISNCSCI score, and then analyzed the clinical characteristic correlations using the best method to measure the obtained diffusion tensor imaging values. Results The maximum circle method had the best consistency. The difference between FA and ADC values of the cervical nerve roots in healthy patients had no statistical significance compared with those of the healthy side of the patients (P>0.05), but had statistical significance compared with those of the affected side. The difference between FA and ADC values on the healthy side of patients and on the affected side was statistically significant (P < 0.05); measured FA and ADC values were correlated with age (P < 0.05), and the older the age, the smaller the FA value and the larger the ADC value, but there was no correlation with BMI. In terms of patients, VAS scores were positively correlated with ADC values on the affected side (P < 0.05) and negatively correlated with FA/ADC ratio on the affected side (P < 0.05), and ISNCSCI scores were positively correlated with FA values (P < 0.05). Conclusion The maximum circle ROI mapping method is a reliable method for diffusion tensor imaging measuring cervical nerve roots. The more obvious the radicular pain, the greater the ADC value and the smaller affected side FA/ ADC ratio. The better the cervical nerve function, the greater the FA value. -

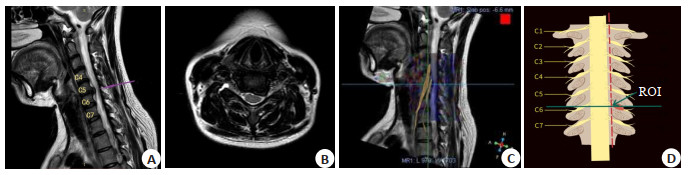
图 1 ROI定位图
A:磁共振成像(矢状面)显示C5~C6颈椎椎间盘突出;B:MRI(轴位面)显示左侧椎间孔狭窄;C:DTI序列,矢状面位于C5~C6;D:ROI在椎间孔入口的位置.
Figure 1. The diagram of ROI positioning.

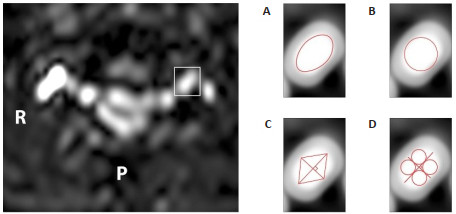
图 2 4种ROI勾画方法
A:轮廓法;B:最大圆法;C:矩形法;D:多中心平均值法.
Figure 2. Four kinds of ROI mapping methods.

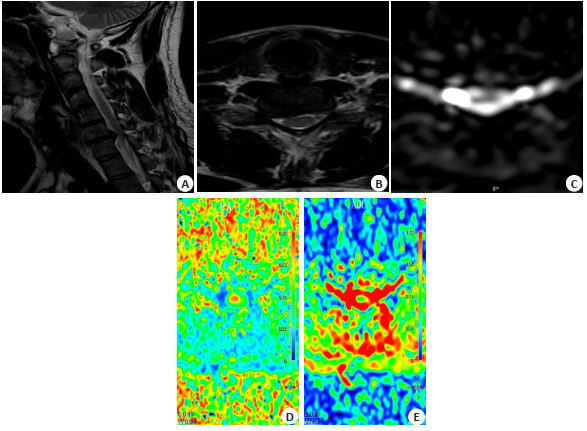
图 3 颈椎间盘突出症患者的MR-DTI图像
男,35岁,右上肢疼痛麻木6月. A:矢状T2加权图像显示颈椎C6~7椎间盘突出;B:C6~7横断面图像显示右侧神经根受压;C:DTI扫描C6~7轴位像:双侧C7神经根呈高亮圆形区域;D:FA图,左侧神经根的FA值高于右侧神经根;E:ADC图,左侧神经根的ADC值低于右侧神经根.
Figure 3. MR-DTI images of patients with cervical disc herniation.
表 1 健康组和颈椎病组的一般资料
Table 1. Baseline characteristics of healthy and cervical spondylosis groups
基本信息 健康组 颈椎病组 年龄(岁,Mean±SD) 44.50±9.57 45.10±9.89 性别[n(%)] 男 11 (55) 11(55) 女 9 (45) 9(45) 受压侧别[n(%)] 左 - 10(50) 右 - 10(50) 受压神经根[n(%)] C4 0(0) 0(0) C5 0(0) 5(0.25) C6 0(0) 9(0.45) C7 0(0) 4(0.20) C8 0(0) 2(0.10) VAS评分(分,Mean±SD) - 8.15±0.33 ISNCSCI评分(分,Mean±SD) - 6.60±0.26 VAS:视觉模拟量表;ISNCSCI:脊髓损伤神经学分类国际标准.  下载: 导出CSV
下载: 导出CSV
表 2 C5神经根采用4种ROI方法健康者DTI测量值
Table 2. DTI measurements of C5 nerve roots in healthy subjects using four ROI methods (n = 20,Mean±SD)
方法 医师A 医师B FA ADC FA ADC 轮廓法 0.363±0.044 1.245±0.039 0.393±0.043 1.214±0.040 最大圆法 0.3834±0.044 1.239±0.047 0.364±0.044 1.259±0.047 矩形法 0.415±0.046 1.232±0.044 0.318±0.059 1.305±0.050 多中心法 0.415±0.046 1.265±0.039 0.364±0.057 1.324±0.040 FA:各向异性分数; ADC:表观弥散系数.
下载: 导出CSV
表 3 C6神经根采用4种ROI方法健康者DTI测量值
Table 3. DTI measurements of C6 nerve roots in healthy subjects using four ROI methods (n = 20,Mean±SD)
方法 医师A 医师B FA ADC FA ADC 轮廓法 0.397±0.063 1.244±0.343 0.371±0.065 1.214±0.045 最大圆法 0.386±0.065 1.236±0.068 0.366±0.0649 1.256±0.067 矩形法 0.378±0.062 1.223±0.053 0.298±0.062 1.296±0.054 多中心法 0.422±0.063 1.267±0.053 0.361±0.063 1.328±0.053
下载: 导出CSV
表 4 C7神经根采用4种ROI方法健康者DTI测量值
Table 4. DTI measurements of C7 nerve roots in healthy subjects using four ROI methods (n = 20,Mean±SD)
方法 医师A 医师B FA ADC FA ADC 轮廓法 0.396±0.060 1.243±0.044 0.365±0.061 1.214±0.044 最大圆法 0.393±0.067 1.236±0.049 0.373±0.067 1.256±0.049 矩形法 0.396±0.060 1.244±0.044 0.365±0.061 1.214±0.044 多中心法 0.421±0.061 1.269±0.044 0.359±0.059 1.529±1.256
下载: 导出CSV
表 5 C8神经根采用4种ROI方法健康者DTI测量值
Table 5. DTI measurements of C8 nerve roots in healthy subjects using 4 ROI methods (n = 20,Mean±SD)
方法 医师A 医师B FA ADC FA ADC 轮廓法 0.404±0.067 1.231±0.053 0.374±0.067 1.201±0.053 最大圆法 0.401±0.075 1.234±0.069 0.381±0.075 1.254±0.069 矩形法 0.383±0.065 1.211±0.053 0.308±0.067 1.281±0.053 多中心法 0.420±0.068 1.535±1.860 0.359±0.069 1.302±0.059
下载: 导出CSV
表 6 2名医师采用4种不同ROI方法健康志愿者DTI测量值一致性(C5~C6)
Table 6. Consistency of DTI values of healthy volunteers using four different ROI methods by two physicians (C5-C6)
方法 C5 C6 ICC 95%CI ICC 95%CI FA ADC FA ADC FA ADC FA ADC 轮廓法 0.789 0.744 0.637, 0.882 0.568, 0.856 0.872 0.796 0.773, 0.930 0.647, 0.886 最大圆法 0.905 0.912 0.828, 0.948 0.840, 0.952 0.955 0.921 0.917, 0.976 0.856, 0.957 矩形法 0.104 0.222 -0.208, 0.398 -0.208, 0.398 0.463 0.161 0.183, 0.674 0.151, 0.446 多中心法 0.546 0.276 0.289, 0.731 -0.033, 0.537 0.542 -0.021 0.284, 0.728 -0.325, 0.287
下载: 导出CSV
表 7 2名医师采用4种不同ROI方法健康志愿者DTI测量值一致性(C7~C8)
Table 7. Consistency of DTI values of healthy volunteers using four different ROI methods by two physicians (C7-C8)
方法 C7 C8 ICC 95%CI ICC 95%CI FA ADC FA ADC FA ADC FA ADC 轮廓法 0.888 0.850 0.799, 0.939 0.736, 0.918 0.903 0.854 0.825, 0.947 0.742, 0.920 最大圆法 0.951 0.957 0.930, 0.967 0.920, 0.977 0.965 0.960 0.935, 0.981 0.927, 0.979 矩形法 0.410 0.344 0.120, 0.637 0.043, 0.589 0.505 0.397 0.235, 0.703 0.104, 0.628 多中心法 0.623 0.504 0.392, 0.781 0.235, 0.702 0.664 0.017 0.449, 0.806 -0.291, 0.322
下载: 导出CSV
表 8 2名医师采用4种不同ROI方法神经根型颈椎病者DTI测量值一致性(C7~C8)
Table 8. Consistence of DTI measurement values of two physicians using four different ROI methods for cervical spondylotic radiculopathy (C7-C8)
方法 ICC 95%CI FA ADC FA ADC 轮廓法 0.967 0.991 0.938, 0.982 0.982, 0.995 最大圆法 0.993 0.998 0.987, 0.996 0.996, 0.999 矩形法 0.993 0.998 0.878, 0.964 0.977, 0.993 多中心法 0.952 0.986 0.912, 0.975 0.973, 0.992
下载: 导出CSV
表 9 DTI值与影响因素相关性
Table 9. Correlation between DTI value and influencing factors
因素 健侧FA 健侧ADC 患侧FA 患侧ADC 患侧/健侧FA 患侧/健侧ADC 患侧FA/ADC 年龄 -0.804* 0.756* - - - - - BMI -0.804 0.125 - - - - - VAS评分 - - -0.423 0.456* -0.321 -0.009 0.434* ISNCSCI评分 - - 0.400* -0.423 0.342 0.009 0.434 *P<0.05.
下载: 导出CSV
-
[1] Childress MA, Becker BA. Nonoperative management of cervical radiculopathy[J]. Am Fam Physician, 2016, 93(9): 746-54. [2] Lee HD, Jeon CH, Chung NS, et al. Is the severity of cervical foraminal Stenosis related to the severity and sidedness of symptoms?[J]. Healthcare (Basel), 2021, 9(12): 1743. [3] Kim SJ, Lee TH, Lim SM. Prevalence of disc degeneration in asymptomatic Korean subjects. Part 1: lumbar spine[J]. J Korean Neurosurg Soc, 2013, 53(1): 31-8. doi: 10.3340/jkns.2013.53.1.31 [4] Kim BY, Concannon TA, Barboza LC, et al. The role of diagnostic injections in spinal disorders: a narrative review[J]. Diagnostics (Basel), 2021, 11(12): 2311. doi: 10.3390/diagnostics11122311 [5] Lannon M, Kachur E. Degenerative cervical myelopathy: clinical presentation, assessment, and natural history[J]. J Clin Med, 2021, 10(16): 3626. doi: 10.3390/jcm10163626 [6] Landman BA, Bogovic JA, Wan HL, et al. Resolution of crossing fibers with constrained compressed sensing using diffusion tensor MRI[J]. Neuroimage, 2012, 59(3): 2175-86. doi: 10.1016/j.neuroimage.2011.10.011 [7] Soldatos T, Andreisek G, Thawait GK, et al. High-resolution 3-T MR neurography of the lumbosacral plexus[J]. Radiographics, 2013, 33(4): 967-87. doi: 10.1148/rg.334115761 [8] Maki S, Koda M, Kitamura M, et al. Diffusion tensor imaging can predict surgical outcomes of patients with cervical compression myelopathy[J]. Eur Spine J, 2017, 26(9): 2459-66. doi: 10.1007/s00586-017-5191-7 [9] Hakulinen U, Brander A, Ilvesmäki T, et al. Reliability of the freehand region-of-interest method in quantitative cerebral diffusion tensor imaging[J]. BMC Med Imaging, 2021, 21(1): 144. doi: 10.1186/s12880-021-00663-8 [10] Ma XD, Han X, Jiang W, et al. A follow-up study of postoperative DCM patients using diffusion MRI with DTI and NODDI[J]. Spine (Phila Pa 1976), 2018, 43(15): E898-E904. doi: 10.1097/BRS.0000000000002541 [11] Nogueira L, Brandão S, Matos E, et al. Region of interest demarcation for quantification of the apparent diffusion coefficient in breast lesions and its interobserver variability[J]. Diagn Interv Radiol, 2015, 21(2): 123-7. doi: 10.5152/dir.2014.14217 [12] Han X, Suo ST, Sun YW, et al. Apparent diffusion coefficient measurement in glioma: influence of region-of-interest determination methods on apparent diffusion coefficient values, interobserver variability, time efficiency, and diagnostic ability[J]. J Magn Reson Imaging, 2017, 45(3): 722-30. doi: 10.1002/jmri.25405 [13] Wako Y, Nakamura J, Eguchi Y, et al. Diffusion tensor imaging and tractography of the sciatic and femoral nerves in healthy volunteers at 3T[J]. J Orthop Surg Res, 2017, 12(1): 184. doi: 10.1186/s13018-017-0690-0 [14] Kotaki S, Sakamoto J, Kretapirom K, et al. Diffusion tensor imaging of the inferior alveolar nerve using 3T MRI: a study for quantitative evaluation and fibre tracking[J]. Dentomaxillofac Radiol, 2016, 45(8): 20160200. doi: 10.1259/dmfr.20160200 [15] Inoue C, Fujii S, Kaneda S, et al. Apparent diffusion coefficient (ADC) measurement in endometrial carcinoma: effect of region of interest methods on ADC values[J]. J Magn Reson Imaging, 2014, 40(1): 157-61. doi: 10.1002/jmri.24372 [16] Bickel H, Pinker K, Polanec S, et al. Diffusion-weighted imaging of breast lesions: region-of-interest placement and different ADC parameters influence apparent diffusion coefficient values[J]. Eur Radiol, 2017, 27(5): 1883-92. doi: 10.1007/s00330-016-4564-3 [17] Ma C, Guo XY, Liu L, et al. Effect of region of interest size on ADC measurements in pancreatic adenocarcinoma[J]. Cancer Imaging, 2017, 17(1): 13. doi: 10.1186/s40644-017-0116-6 [18] Jafari-Khouzani K, Paynabar K, Hajighasemi F, et al. Effect of region of interest size on the repeatability of quantitative brain imaging biomarkers[J]. IEEE Trans Biomed Eng, 2019, 66(3): 864-72. doi: 10.1109/TBME.2018.2860928 [19] Nenonen M, Hakulinen U, Brander A, et al. Possible confounding factors on cerebral diffusion tensor imaging measurements[J]. Acta Radiol Open, 2015, 4(2): 2047981614546795. doi: 10.1177/2047981614546795 [20] Liu L, Ma C, Li J, et al. Comparison of the diagnostic performances of three techniques of ROI placement for ADC measurements in pancreatic adenocarcinoma[J]. Acad Radiol, 2015, 22(11): 1385-92. doi: 10.1016/j.acra.2015.06.017 [21] Ahn SJ, Shin HJ, Chang JH, et al. Differentiation between primary cerebral lymphoma and glioblastoma using the apparent diffusion coefficient: comparison of three different ROI methods[J]. PLoS One, 2014, 9(11): e112948. doi: 10.1371/journal.pone.0112948 [22] Sun YQ, Xiao Q, Hu FX, et al. Diffusion kurtosis imaging in the characterisation of rectal cancer: utilizing the most repeatable region-of-interest strategy for diffusion parameters on a 3T scanner [J]. Eur Radiol, 2018, 28(12): 5211-20. doi: 10.1007/s00330-018-5495-y [23] Toktas ZO, Tanrıkulu B, Koban O, et al. Diffusion tensor imaging of cervical spinal cord: a quantitative diagnostic tool in cervical spondylotic myelopathy[J]. J Craniovertebr Junction Spine, 2016, 7 (1): 26-30. doi: 10.4103/0974-8237.176617 [24] Temur HO, Yurtsever I, Yesil G, et al. Correlation between DTI findings and volume of corpus callosum in children with AUTISM [J]. Curr Med Imaging Rev, 2019, 15(9): 895-9. doi: 10.2174/1573405614666181005114315 [25] Lawrence KE, Nabulsi L, Santhalingam V, et al. Age and sex effects on advanced white matter microstructure measures in 15,628 older adults: a UK biobank study[J]. Brain Imaging Behav, 2021, 15(6): 2813-23. doi: 10.1007/s11682-021-00548-y [26] Liang KN, Feng PY, Feng XR, et al. Diffusion tensor imaging and fiber tractography reveal significant microstructural changes of cervical nerve roots in patients with cervical spondylotic radiculopathy[J]. World Neurosurg, 2019,126: e57-e64. doi: 10.1016/j.wneu.2019.01.154 [27] Turna O, Turna IF. Quantitative assessment of cervical spinal cord by diffusion tensor tractography in 3.0 T[J]. La Radiol Med, 2021,126(1): 83-8. doi: 10.1007/s11547-020-01224-9 [28] Hofstadler B, Bäumer P, Schwarz D, et al. MR neurography: normative values in correlation to demographic determinants in children and adolescents[J]. Clin Neuroradiol, 2020, 30(4): 671-7. doi: 10.1007/s00062-019-00834-9 [29] Tanitame K, Iwakado Y, Akiyama Y, et al. Effect of age on the fractional anisotropy (FA) value of peripheral nerves and clinical significance of the age-corrected FA value for evaluating polyneuropathies[J]. Neuroradiology, 2012, 54(8): 815-21. doi: 10.1007/s00234-011-0981-9 [30] Chen YY, Lin XF, Zhang F, et al. Diffusion tensor imaging of symptomatic nerve roots in patients with cervical disc herniation[J]. Acad Radiol, 2014, 21(3): 338-44. doi: 10.1016/j.acra.2013.11.005 [31] Shi Y, Zou YF, Feng Y, et al. A quantitative and clinical evaluation of nerve roots in lumbosacral radiculopathy using diffusion tensor imaging[J]. Jpn J Radiol, 2020, 38(3): 222-30. doi: 10.1007/s11604-019-00913-4 [32] Wang K, Chen Z, Zhang F, et al. Evaluation of DTI parameter ratios and diffusion tensor tractography grading in the diagnosis and prognosis prediction of cervical spondylotic myelopathy[J]. Spine (Phila Pa 1976), 2017, 42(4): E202-E210. doi: 10.1097/BRS.0000000000001784 [33] Wu WF, Liang J, Ru N, et al. Microstructural changes in compressed nerve roots are consistent with clinical symptoms and symptom duration in patients with lumbar disc herniation[J]. Spine (Phila Pa 1976), 2016, 41(11): E661-E666. doi: 10.1097/BRS.0000000000001354 [34] Iliescu BF, Gutu P, Dabija MG. Traumatic subaxial cervical spine injury - Improving initial evaluation through correlation of diffusion tensor imaging and subaxial cervical spine injury classification SLIC score[J]. Surg Neurol Int, 2021, 12: 10. doi: 10.25259/SNI_274_2020 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 166
- HTML全文浏览量: 103
- PDF下载量: 17
- 被引次数: 0