



Application value of magnetic resonance in the diagnosis of idiopathic central precocity in girls and its correlation with sex hormones
-
摘要:
目的 研究磁共振在诊断女童特发性中枢性性早熟中的应用价值及其与性激素的相关性。 方法 选取2019年9月~2021年10月我院收治的特发性中枢性性早熟女童58例作为性早熟组,再分别选取同期在我院体检的单纯乳房发育女童和健康女童58例作为乳房发育组和健康对照组,所有女童均进行垂体磁共振检查。比较3组临床体征、血清性激素水平及垂体情况,采用Pearson相关性分析法分析特发性中枢性性早熟女童垂体情况与体征和血清性激素水平的相关性。 结果 性早熟组身高、体质量、骨龄超前指数及垂体高度均高于乳房发育组、健康对照组(P < 0.05)。性早熟组血清雌二醇水平高于乳房发育组和健康对照组,乳房发育组高于健康对照组(P < 0.05),性早熟组血清黄体生成素水平、黄体生成素/卵泡刺激素高于乳房发育组(P < 0.05)。性早熟组垂体形态Ⅳ~Ⅴ级女童占比(84.48%)高于乳房发育组和健康对照组(15.52%、20.69%,P < 0.05)。Pearson相关性分析结果显示,特发性中枢性性早熟女童身高、体质量、骨龄超前指数及血清雌二醇、黄体生成素水平、黄体生成素/卵泡刺激素与垂体高度和垂体形态呈显著正相关关系(r=0.694、0.884、0.838、0.937、0.895、0.799和0.784、0.895、0.835、0.947、0.884、0.905,P < 0.05)。 结论 与单纯乳房发育女童和健康女童相比,特发性中枢性性早熟女童身高、体质量、超前骨龄指数、血清性激素水平及垂体高度、垂体形态分级均更高,特发性中枢性性早熟女童垂体高度、垂体形态分级与身高、体质量、超前骨龄指数、血清性激素水平均呈显著正相关关系。 Abstract:Objective To explore the application value of magnetic resonance in diagnosis of idiopathic central precocity in girls and its correlation with sex hormones. Methods Fifty-eight girls with idiopathic central precocious puberty admitted to our hospital from September 2019 to October 2021 were selected as the precocious puberty group, and 58 girls with simple breast development and 58 healthy girls who were examined in our hospital during the same period were selected as the breast development group and the healthy control group respectively. All girls underwent pituitary MRI. The clinical signs, serum levels of sex hormone and pituitary status of the three groups were compared, and the correlation between pituitary status, physical signs and serum levels of sex hormone of girls with idiopathic central precocious puberty was analyzed by Pearson correlation analysis. Results The height, weight, bone age advance index and pituitary height of the precocious puberty group were higher than those of the breast development group and the healthy control group (P < 0.05). The level of E2 in the precocious puberty group was higher than that in the breast development group and the healthy control group, and that in the breast development group was higher than that in the healthy control group (P < 0.05). The level of serum luteinizing hormone and luteinizing hormone/follicle stimulating hormone in the precocious puberty group were higher than that in the breast development group (P < 0.05). The proportion of patients with pituitary morphology of grade Ⅳ-Ⅴ in the precocious puberty group (84.48%) was higher than that in the breast development group and the healthy control group (15.52%, 20.69%, P < 0.05). Pearson correlation analysis showed that height, body mass, advanced bone age index, serum levels of E2, luteinizing hormone, luteinizing hormone/follicle stimulating hormone were positively correlated with pituitary height and morphology in girls with idiopathic central precocious puberty (r=0.694, 0.884, 0.838, 0.937, 0.895, 0.799 and 0.784, 0.895, 0.835, 0.947, 0.884, 0.905, P < 0.05). Conclusion Compared to girls with simple breast development and healthy girls, girls with idiopathic central precocious puberty have higher height, weight, advanced bone age index, serum sex hormone level, pituitary height and pituitary morphological classification, and girls with idiopathic central precocity had a significant positive correlation between pituitary height and pituitary morphological grading and height, weight, premature bone age index and serum sex hormone levels. -
Key words:
- idiopathic central precocity /
- girls /
- magnetic resonance imaging /
- application value /
- sex hormones /
- correlation
-
表 1 一般资料比较
Table 1. Comparison of general data (n=58, Mean±SD)
组别 年龄(岁) 身高(cm) 体质量(kg) 骨龄指数超前 性早熟组 7.19±0.73 151.74±11.73*# 40.00±9.83*# 1.39±0.45*# 乳房发育组 7.25±0.69 130.47±13.85 31.50±8.58 1.09±0.12 健康对照组 7.20±0.79 129.83±12.73 31.74±6.84 0.96±0.14 F 0.080 55.046 18.779 35.781 P 0.923 < 0.001 < 0.001 < 0.001 *P < 0.05 vs乳房发育组; #P < 0.05 vs健康对照组.  下载: 导出CSV
下载: 导出CSV
表 2 性激素水平比较
Table 2. Comparison of sex hormone levels (n=58, Mean±SD)
组别 E2(pg/mL) LH(mU/mL) LH/FSH 性早熟组 28.90±4.70*# 10.81±0.09# 1.18±0.14# 乳房发育组 20.19±0.78* 2.77±0.15 0.24±0.08 健康对照组 15.18±0.15 - - F/t 369.126 29.222 6.499 P < 0.001 < 0.001 < 0.001 *P < 0.05 vs乳房发育组; #P < 0.05 vs健康对照组; E2: 雌二醇; LH: 黄体生成素; FSH: 卵泡刺激素.
下载: 导出CSV
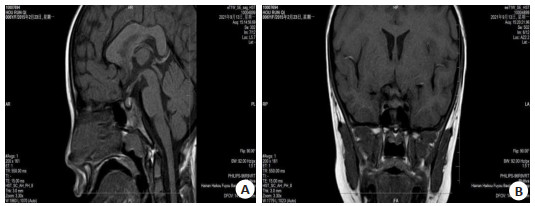
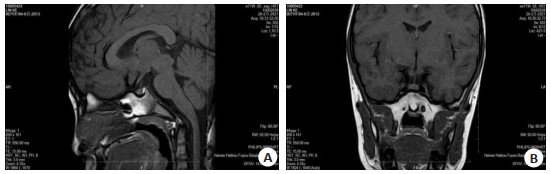
表 3 垂体情况比较
Table 3. Comparison of pituitary among (n=58)
组别 垂体高度(mm, Mean±SD) 垂体形态[n(%)] Ⅰ~Ⅲ级 Ⅳ~Ⅴ级 性早熟组 5.11±0.85*# 9(15.52)*# 49(84.48)*# 乳房发育组 4.12±0.47 49(84.48) 9(15.52) 健康对照组 4.08±0.53 46(79.31) 12(20.69) F/χ2 48.383 71.177 P < 0.001 < 0.001 *P < 0.05 vs乳房发育组; #P < 0.05 vs健康对照组.
下载: 导出CSV
表 4 特发性中枢性性早熟女童垂体情况与体征、性激素水平的相关性分析
Table 4. Correlation analysis of pituitary condition, signs and sex hormone levels in girls with idiopathic central precocious puberty
体征、性激素 垂体高度 垂体形态 r P r P 身高 0.694 < 0.05 0.784 < 0.05 体质量 0.884 < 0.05 0.895 < 0.05 骨龄指数超前 0.838 < 0.05 0.835 < 0.05 E2 0.937 < 0.05 0.947 < 0.05 LH 0.895 < 0.05 0.884 < 0.05 LH/FSH 0.799 < 0.05 0.905 < 0.05
下载: 导出CSV
-
[1] Leka-Emiri S, Chrousos GP, Kanaka-Gantenbein C. The mystery of puberty initiation: genetics and epigenetics of idiopathic central precocious puberty (ICPP)[J]. J Endocrinol Invest, 2017, 40(8): 789-802. doi: 10.1007/s40618-017-0627-9 [2] Furtado CLM, Iannetta R, Ferriani RA, et al. Telomere length is not altered in girls with idiopathic central precocious puberty treated with a GnRH analog-leuprolide acetate[J]. Gynecol Endocrinol, 2020, 36(12): 1119-23. doi: 10.1080/09513590.2020.1770212 [3] 王琰华, 赵忻, 刘冀琴. 天津市女童单纯乳房早发育及特发性中枢性性早熟发病危险因素的分析[J]. 中国儿童保健杂志, 2018, 26(4): 444-7. https://www.cnki.com.cn/Article/CJFDTOTAL-ERTO201804029.htm [4] 中华医学会儿科学分会内分泌遗传代谢学组. 对中枢性(真性)性早熟诊断和治疗的建议[J]. 中华儿科杂志, 2003, 41(4): 272-3. doi: 10.3760/j.issn:0578-1310.2003.04.010 [5] 李钱程, 张欣贤, 李成龙, 等. 磁共振在特发性中枢性性早熟女童临床诊断中的应用分析[J]. 医学影像学杂志, 2018, 28(10): 1601-4, 1681. https://www.cnki.com.cn/Article/CJFDTOTAL-XYXZ201810005.htm [6] 戴艺, 黄雪艳, 覃佩云, 等. 7~9岁特发性中枢性性早熟女童的骨骼营养情况[J]. 广西医学, 2020, 42(8): 954-6. https://www.cnki.com.cn/Article/CJFDTOTAL-GYYX202008007.htm [7] Tencer J, Lemaire P, Brailly-Tabard S, et al. Serum inhibin B concentration as a predictor of age at first menstruation in girls with idiopathic central precocious puberty[J]. PLoS One, 2018, 13(12): e0205810. doi: 10.1371/journal.pone.0205810 [8] Lee YB, Lee JA, Lee HL. Herbal medicine for idiopathic central precocious puberty: a systematic review and meta-analysis[J]. J Altern Complementary Med, 2020, 26(11): 976-99. doi: 10.1089/acm.2019.0312 [9] Seraphim CE, Canton APM, Montenegro L, et al. Genotypephenotype correlations in central precocious puberty caused by MKRN3 mutations[J]. J Clin Endocrinol Metab, 2021, 106(4): 1041-50. doi: 10.1210/clinem/dgaa955 [10] Lee HY, Lee YJ, Ahn MB, et al. The effect of overweight on the luteinizing hormone level after gonadorelin stimulation test in girls with idiopathic central precocious puberty[J]. Ann Pediatr Endocrinol Metab, 2018, 23(4): 215-9. doi: 10.6065/apem.2018.23.4.215 [11] Chung LY, Nam HK, Rhie YJ, et al. Prevalence of idiopathic scoliosis in girls with central precocious puberty: effect of a gonadotropin-releasing hormone agonist[J]. Ann Pediatr Endocrinol Metab, 2020, 25(2): 92-6. doi: 10.6065/apem.1938164.082 [12] 刘珍珍, 徐露莲, 蒋莉, 等. 特发性中枢性性早熟对比单纯乳房发育女童垂体发育及性激素表达临床差异性分析[J]. 中国性科学, 2019, 28(3): 103-6. https://www.cnki.com.cn/Article/CJFDTOTAL-XKXZ201903031.htm [13] 张莹, 王龙胜. 中枢性性早熟女童腺垂体前叶高度与体内性激素水平的相关性研究[J]. 安徽医学, 2020, 41(4): 417-20. doi: 10.3969/j.issn.1000-0399.2020.04.016 [14] Lee HL, Lee YB, Choi JY, et al. Herbal medicine for idiopathic central precocious puberty: a protocol for a systematic review of controlled trials[J]. Medicine, 2018, 97(13): e0267. doi: 10.1097/MD.0000000000010267 [15] Dayal D, Yadav J, Seetharaman K, et al. Etiological spectrum of precocious puberty: data from northwest India[J]. Indian Pediatr, 2020, 57(1): 63-4. doi: 10.1007/s13312-020-1705-1 [16] 朱晓雷, 陈璐, 陆文丽, 等. 474例中枢性性早熟女童不同年龄段垂体MRI影像学异常比例分析[J]. 诊断学理论与实践, 2019, 18(3): 286-90. https://www.cnki.com.cn/Article/CJFDTOTAL-ZDLS201903011.htm [17] Ge W, Wang HL, Shao HJ, et al. Evaluation of serum makorin ring finger protein 3 (MKRN3) levels in girls with idiopathic central precocious puberty and premature thelarche[J]. Physiol Res, 2020, 69(1): 127-33. http://www.ncbi.nlm.nih.gov/pubmed/31852205/ [18] Altıncık A, Sayın O. Serum nesfatin-1 levels in girls with idiopathic central precocious puberty[J]. J Clin Res Pediatr Endocrinol, 2018, 10(1): 8-12. doi: 10.4274/jcrpe.4677 [19] Vurallı D, Özön A, Gönç EN, et al. Gender-related differences in etiology of organic central precocious puberty[J]. Turk J Pediatr, 2020, 62(5): 763-9. doi: 10.24953/turkjped.2020.05.007 [20] Zhao Y, Long WJ, Du CQ, et al. Prevalence of vitamin D deficiency in girls with idiopathic central precocious puberty[J]. Front Med, 2018, 12(2): 174-81. doi: 10.1007/s11684-017-0544-5 [21] 张倩茹, 陈瑞敏, 蔡春艳, 等. 促性腺激素释放激素类似物治疗对特发性中枢性性早熟女性患儿远期糖脂代谢及性腺轴功能影响观察[J]. 中国实用儿科杂志, 2017, 32(12): 933-6. https://www.cnki.com.cn/Article/CJFDTOTAL-ZSEK201712013.htm [22] Aiello F, Cirillo G, Cassio A, et al. Molecular screening of PROKR2 gene in girls with idiopathic central precocious puberty[J]. Ital J Pediatr, 2021, 47(1): 5. doi: 10.1186/s13052-020-00951-z -

 点击查看大图
点击查看大图
计量
- 文章访问数: 167
- HTML全文浏览量: 131
- PDF下载量: 3
- 被引次数: 0