



Relationship between high-resolution MRI combined with carotid ultrasound and detection of carotid stenosis in patients with acute cerebral infarction and risk factors affecting patient prognosis
-
摘要:
目的 探究高分辨率MRI联合颈动脉超声与急性脑梗死发病人群颈动脉狭窄程度检出情况的关系及影响患者预后的危险因素。 方法 本研究为前瞻性研究,选取2018年1月~2020年12月诊断为脑梗死的67例患者作为研究对象,其中颈动脉狭窄患者35例,非颈动脉狭窄患者32例。比较两组患者的颈动脉超声、3.0 T MRI的诊断差异,分析影响患者预后的危险因素。 结果 颈动脉狭窄与非颈动脉狭窄组患者的性别、年龄以及BMI的差异无统计学意义(P > 0.05),颈动脉狭窄组患者的糖尿病(χ2=7.102,P=0.007)、高血压(χ2=5.902,P=0.015)以及高脂血症(χ2=4.532,P=0.033)患者的比例高于非颈动脉狭窄组;颈动脉狭窄组患者的收缩期最大流速(PSV)(t=4.992,P < 0.001)、舒张末期血流速度(EDV)(t=15.210,P < 0.001)低于非颈动脉狭窄组,颈动脉狭窄组患者的颈动脉中膜厚度(IMT)(t=16.835,P < 0.001)高于非颈动脉狭窄组;不同颈动脉狭窄程度患者的颈动脉PSV(F= 4.968,P < 0.001)、IMT(F=16.468,P < 0.001)、EDV(F=14.791,P < 0.001)之间的差异存在统计学意义,经两两比较,患者的PSV以及EDV从高到低依次为轻度组、中度组以及重度组,IMT从高到低依次为重度组、中度组以及轻度组;颈动脉超声与MRI检查诊断一致性较强,不同预后患者的年龄(t=4.532,P < 0.001)、BMI(t=2.324,P=0.023)、糖尿病(χ2=10.602,P=0.001)、高血压(χ2= 7.502,P=0.006)、高血脂(χ2=7.202,P=0.007)、PSV(t=20.013,P < 0.001)、IMT(t=4.708,P < 0.001)、EDV(t=22.018,P < 0.001)的差异有统计学意义;通过多因素分析,年龄、BMI、高脂血症、糖尿病、高血压、PSV、IMT、EDV均是造成患者预后不良的危险因素。 结论 脑梗死患者采取颈动脉超声联合3.0T MRI检查,对于患者的疾病严重程度具有显著的意义,同时年龄较大、体质量过高、高血压、糖尿病以及高血脂均是造成患者疾病进展的重要危险因素。 Abstract:Objective To explore the relationship between high-resolution MRI combined with carotid ultrasound and the detection of carotid stenosis in patients with acute cerebral infarction and the risk factors affecting the prognosis of patients. Methods In this prospective study, 67 patients diagnosed with cerebral infarction from January 2018 to December 2020 were selected as the research objects, including 35 patients with carotid stenosis and 32 patients with non-carotid stenosis. The differences of carotid ultrasound and 3.0 T MRI diagnosis between the two groups were compared, and the risk factors affecting the prognosis of patients were analyzed. Results There was no significant difference in gender, age and BMI between patients with carotid stenosis and non-carotid stenosis group (P > 0.05). The proportion of patients with diabetes mellitus carotid stenosis group was not significant (χ2=7.102, P=0.007), hypertension (χ2=5.902, P=0.015) and hyperlipidemia (χ2=4.532, P= 0.033) was significantly higher in the carotid stenosis group than that in the non-carotid stenosis group. The maximum systolic velocity (PSV) (t=4.992, P < 0.001)and end-diastolic velocity (EDV) (t=15.210, P < 0.001) in the carotid stenosis group were significantly lower than that in the non-carotid stenosis group, and the intima-media thickness (IMT) (t=16.835, P < 0.001) in the patients with carotid stenosis was significantly higher than those in the non-carotid stenosis group. The difference in caroid PSV (F=4.968, P < 0.001), IMT (F=16.468, P < 0.001), EDV (F=14.791, P < 0.001) between patients with different degrees of carotid stenosis were statistically significant. After comparison between the two groups, PSV and EDV in the three groups were ranked from high to low were mild, moderate and severe, and IMT was in the order of severe, moderate and mild groups. There was strong diagnostic agreement between carotid ultrasound and MRI, with different prognoses for age (t=4.532, P < 0.001), BMI (t=2.324, P=0.023), diabetes (χ2=10.602, P=0.001), hypertension (χ2=7.502, P=0.006), hyperlipidemia (χ2=7.202, P= 0.007), PSV (t=20.013, P < 0.001), IMT (t=4.708, P < 0.001), EDV (t=22.018, P < 0.001). Through multivariate analysis, age, BMI, hyperlipidemia, diabetes mellitus, hypertension, PSV, IMT and EDV were all the risk factors for poor prognosis. Conclusion Carotid ultrasound combines with 3.0T MRI examination in patients with cerebral infarction is significance for the severity of the disease, while older age, high weight, hypertension, diabetes and hyperlipidemia are all important risk factors for disease progression. -
Key words:
- carotid artery stenosis /
- cerebral infarction /
- ultrasound /
- nuclear magnetic resonance /
- risk factors
-

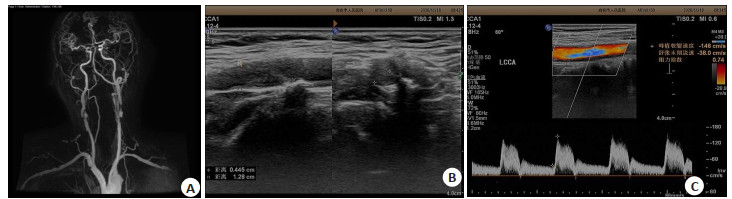
图 1 超声相关参数测量示意图
A: 患者颈内动脉多段明显狭窄; B: 常规超声观察颈动脉斑块位置、形态,该斑块位于颈总动脉分叉处,呈低回声扁平斑块, 斑块表面不光滑, 大小约12.8 mm×4.5 mm; C: 斑块所处颈动脉PSV、颈动脉EDV.
Figure 1. Diagram of ultrasonic related parameter measurement.
表 1 颈动脉狭窄与非颈动脉狭窄组患者的一般资料比较
Table 1. Comparison of general data of patients with carotid artery stenosis and non carotid artery stenosis
组别 性别(男/女) 年龄(岁) BMI (kg/m2) 糖尿病 高血压 高脂血症 狭窄组(n=35) 15/20 60.35±3.09 24.66±3.09 20 30 20 非狭窄组(n=32) 17/15 60.14±3.11 24.09±2.78 8 19 10 t/χ2 0.712 0.277 0.795 7.102 5.902 4.532 P 0.401 0.783 0.43 0.007 0.015 0.033  下载: 导出CSV
下载: 导出CSV
表 2 颈动脉狭窄与非颈动脉狭窄组患者的颈动脉超声参数比较
Table 2. Comparison of carotid ultrasound parameters between carotid stenosis group and non carotid stenosis group (Mean±SD)
组别 PSV (cm/s) IMT (mm) EDV (cm/s) 狭窄组(n=35) 50.26±9.19 0.89±0.12 12.73±1.26 非狭窄组(n=32) 60.89±8.24 0.49±0.07 20.27±2.62 t 4.992 16.835 15.210 P < 0.001 < 0.001 < 0.001 PSV: 收缩期最大流速; IMT: 颈动脉中膜厚度; EDV: 舒张末期血流速度.
下载: 导出CSV
表 3 不同颈动脉狭窄程度患者的颈动脉超声参数比较
Table 3. Comparison of carotid ultrasound parameters in patients with different degrees of carotid stenosis (Mean±SD)
组别 PSV (cm/s) IMT (mm) EDV (cm/s) 轻度组(n=12) 55.28±1.56 0.80±0.08 25.07±1.88 中度组(n=11) 50.09±2.35 0.88±0.02 19.97±2.37 重度组(n=12) 45.40±2.51 0.99±0.24 15.75±2.79 F 4.968 16.468 14.791 P < 0.001 < 0.001 < 0.001 LSD-t (轻度vs中度) 6.789 12.342 14.559 P < 0.001 < 0.001 < 0.001 LSD-t (轻度vs重度) 8.369 11.030 15.478 P < 0.001 < 0.001 < 0.001 LSD-t (重度vs中度) 9.589 12.569 19.885 P < 0.001 < 0.001 < 0.001
下载: 导出CSV
表 4 颈动脉超声与MRI检查的一致性分析
Table 4. Consistency analysis of carotid ultrasound and MRI
指标 MRI检查 轻度组 中度组 重度组 颈动脉超声 轻度组 9 2 1 中度组 1 9 1 重度组 1 2 9 Kappa 12.588 P < 0.001
下载: 导出CSV
表 5 不同预后患者的一般资料分析
Table 5. Analysis of general data of patients with different prognosis (n, Mean±SD)
组别 性别(男/女) 年龄(岁) BMI (kg/m2) 糖尿病 高血压 高脂血症 PSV (cm/s) IMT (mm) EDV (cm/s) 预后良好组(n=30) 15/15 58.45±3.11 23.62±3.12 6 17 8 60.21±1.95 0.83±0.03 12.65±1.45 预后不良组(n=37) 17/20 62.14±3.55 25.25±2.49 22 32 22 50.60±1.96 0.89±0.07 20.21±1.33 t/χ2 0.112 4.532 2.324 10.602 7.502 7.202 20.013 4.708 22.018 P 0.741 < 0.001 0.023 0.001 0.006 0.007 < 0.001 < 0.001 < 0.001
下载: 导出CSV
表 6 预后不良患者的多因素分析
Table 6. Multivariate analysis of patients with poor prognosis
因素 β S.E. Wald P OR 95%CI 年龄 0.339 2.36 1.320 < 0.001 1.022 0.900~1.931 体重指数 0.397 3.272 1.330 < 0.001 1.635 1.330~2.325 高脂血症 0.007 3.293 1.330 < 0.001 1.606 1.390~2.315 糖尿病 0.541 3.225 1.452 < 0.001 1.442 1.211~1.590 高血压 0.412 1.994 1.855 < 0.001 1.204 1.115~1.660 PSV 0.451 1.559 1.036 < 0.001 1.256 1.055~2.521 IMT 0.552 1.602 1.252 < 0.001 1.256 1.096~5.996 EDV 0.449 1.974 1.229 < 0.001 1.200 1.003~1.998 PSV: 收缩期最大流速; IMT: 颈动脉中膜厚度; EDV: 舒张末期血流速度.
下载: 导出CSV
-
[1] 张锐利, 魏晓珊, 秦晓丰, 等. 替罗非班治疗颈动脉漂浮血栓相关脑梗死[J]. 国际神经病学神经外科学杂志, 2021, 48(1): 99-102. https://www.cnki.com.cn/Article/CJFDTOTAL-GWSK202101024.htm [2] 张增平, 王伟佳, 孔憶娜, 等. 急性脑梗死患者血清脂联素、白细胞介素-8水平与颈动脉粥样硬化斑块稳定性的相关性[J]. 徐州医科大学学报, 2019, 39(4): 289-92. doi: 10.3969/j.issn.2096-3882.2019.04.014 [3] Ismail O, Abdo Elhindawy K, Eldien MM. Carotid artery stenting in high-risk patients: immediate and short-term results[J]. Egypt J Surg, 2020, 39(2): 305. doi: 10.4103/ejs.ejs_203_19 [4] 辛涛, 潘源, 贺西亮, 等. 复杂类型症状性颈动脉重度狭窄的血管内治疗[J]. 中华航海医学与高气压医学杂志, 2020, 27(4): 481-5, 492. doi: 10.3760/cma.j.cn311847-20200410-00141 [5] 潘源, 上官秀, 杨帆, 等. 彩色多普勒超声在颈动脉狭窄诊断中的应用价值分析[J]. 中华神经医学杂志, 2020, 19(11): 1149-52. doi: 10.3760/cma.j.cn115354-20200221-00098 [6] 黄亚波, 周鹏, 韩庆东, 等. 颈动脉体瘤无血手术切除技术探讨(附12例报告) J]. 中华神经外科杂志, 2020, 36(8): 823-8. doi: 10.3760/cma.j.cn112050-20200325-00159 [7] 文琼, 段依恋, 项飞翔, 等. 三维超声测量颈动脉斑块灰阶中位数值与脑梗死预测的关系[J]. 华中科技大学学报: 医学版, 2020, 49(4): 486-90. doi: 10.3870/j.issn.1672-0741.2020.04.020 [8] 吴向菊, 张春梅, 董丹, 等. 超声在颈内动脉狭窄与无症状性脑梗死相关性研究中的应用[J]. 哈尔滨医科大学学报, 2018, 52(1): 71-4. doi: 10.3969/j.issn.1000-1905.2018.01.018 [9] 童陶然, 周菁菁, 曹昌权. 颈动脉超声定量参数结合MRI对急性脑梗死患者的诊断价值[J]. 中国CT和MRI杂志, 2019, 17(7): 29-31, 49. doi: 10.3969/j.issn.1672-5131.2019.07.009 [10] 邵秋季, 李立, 李天晓, 等. LEO Baby支架在颅内宽颈动脉瘤血管内治疗中的初步应用[J]. 中华神经外科杂志, 2020, 36(5): 499-504. doi: 10.3760/cma.j.cn112050-20200102-00004 [11] 黄书翰, 刘承春, 李小树, 等. Solitaire支架半释放保护技术治疗急性颈内动脉串联闭塞患者的效果分析[J]. 中国脑血管病杂志, 2021, 18 (4): 223-33. doi: 10.3969/j.issn.1672-5921.2021.04.002 [12] Ito H, Uchida M, Takasuna H, et al. Analysis of postprocedural microembolic infarctions and global oxygen extraction fraction during balloon-protected carotid artery stenting: preliminary study [J]. Surg Neurol Int, 2021, 12: 87. doi: 10.25259/SNI_919_2020 [13] Kashyap VS, Schneider PA, Foteh M, et al. Early outcomes in the ROADSTER 2 study of transcarotid artery revascularization in patients with significant carotid artery disease[J]. Stroke, 2020, 51 (9): 2620-9. doi: 10.1161/STROKEAHA.120.030550 [14] Shimizu Y, Tsuchiya K, Fujisawa N. Intracerebral steal phenomenon induced focal reversible vasogenic edema and decrease in cerebral blood flow after carotid endarterectomy[J]. Surg Neurol Int, 2020, 11: 161. doi: 10.25259/SNI_508_2019 [15] Ravikanth R. Relevance of carotid intima-media thickness and plaque morphology in the risk assessment of patients with acute ischemic cerebral infarcts: a case-control study of large series from a single center[J]. J Med Ultrasound, 2019, 28(1): 29-34. [16] Ahn JM, Oh HJ, Oh JS, et al. Pituitary apoplexy causing acute ischemic stroke: which treatment should be given priority[J]. Surg Neurol Int, 2020, 11: 113. doi: 10.25259/SNI_82_2020 [17] Matsuyama H, Shindo A, Shimada T, et al. Chronic cerebral hypoperfusion activates AIM2 and NLRP3 inflammasome[J]. Brain Res, 2020, 1736: 146779. doi: 10.1016/j.brainres.2020.146779 [18] Nakahara M, Misaki K, Tsutsui T, et al. Effect of unilateral carotid artery stenting on cognitive function in patients with severe bilateral Stenosis[J]. World Neurosurg, 2020, 135: 188-91. doi: 10.1016/j.wneu.2019.12.068 [19] 段新平, 张俊英, 郭文博. 颈部血管彩超和MRI在脑梗死患者颈动脉狭窄检测中的应用[J]. 中国CT和MRI杂志, 2018, 16(6): 47-9. doi: 10.3969/j.issn.1672-5131.2018.06.015 [20] 王正江, 韩斯庆, 郑永强. 不同年龄层次急性脑梗死患者rt-PA静脉溶栓的临床疗效及出血风险对比[J]. 吉林医学, 2021, 42(10): 2345-7. doi: 10.3969/j.issn.1004-0412.2021.10.012 [21] 祝腊香, 庞洪波, 李雪芹. 急性脑梗死血清IL-6、hs-CRP与颈动脉粥样硬化斑块稳定性的关系[J]. 中国煤炭工业医学杂志, 2013, 16(8): 1268-70. https://www.cnki.com.cn/Article/CJFDTOTAL-ZMGY201308015.htm -

 点击查看大图
点击查看大图
计量
- 文章访问数: 158
- HTML全文浏览量: 66
- PDF下载量: 4
- 被引次数: 0