



Assessment of local microcirculatory status and infarct type in patients with severe stenosis or occlusion of the middle cerebral artery via cerebral perfusion imaging
-
摘要:
目的 利用双源CT脑灌注成像(CTP)技术,探讨大脑中动脉重度狭窄或闭塞的所致脑梗死灶分布类型与侧支循环建立相关性,并进一步探索不同侧支血管建立缺血区域微循环状态。 方法 收集经CT血管造影证实单侧大脑中动脉狭窄率 > 70%、症状性猝中的患者80例。在弥散加权成像上,将脑梗死类型分为穿支动脉梗死、大面积梗死、皮质供血区梗死、分水岭梗死、多发脑梗塞及无梗死灶。经CTP成像,将所有患者分为侧支循环良好组(n=48)与不良组(n=32),分析两组灌注参数差异及相关危险因素,并用半影计算软件分析缺血半暗带区与核心梗死区,对比弥散加权成像高信号区与核心梗死区是否差异及脑梗死类型分布与侧支循环相关性。 结果 侧支循环不良组男性比例及高血压患者比例高于侧支循环良好组(P < 0.05)。所有患者CTP结果均为阳性,核心梗死区阳性66例,弥散加权成像阳性为68例,两种方法对急性脑梗死诊断具有一致性,侧支循环良好组脑梗死类型以穿支动脉梗死为著,侧支循环不良组以分水岭梗死为著。对于两组间缺血半暗带区灌注参数进行比较,脑血流量值的差异无统计学意义(P > 0.05),侧支循环良好组脑血容量增加,平均通过时间和达峰时间缩短,差异有统计学意义(P < 0.05)。 结论 大脑中动脉重度狭窄或闭塞的所致脑梗死灶分布类型与侧支循环建立有关,CTP成像可较早发现缺血区域,精准评估责任血管的狭窄程度及局部血流动力学信息,半影计算模式可更快捷地评估缺血核心梗死区及缺血半暗带区。 Abstract:Objective To explore the correlation between the distribution of cerebral infarction caused by severe stenosis or occlusion of the middle cerebral artery and the establishment of collateral circulation using dual-source CT cerebral perfusion imaging (CTP), and further explore the state of microcirculation in the area of ischemia established by different collateral vessels. Methods 80 patients with unilateral middle cerebral artery stenosis > 70% and symptomatic sudden stroke confirmed by CT angiography were collected. On the diffusion-weighted image, the types of cerebral infarction were divided into perforating artery infarction, large area infarction, cortical blood supply area infarction, watershed infarction and multiple cerebral infarction and no infarcts. After CTP imaging, all patients were divided into two groups with good collateral circulation and poor circulation, and differences in perfusion parameters and related risk factors between the two groups were analyzed. Penumbra calculation software was used to analyze the ischemic penumbra area and core infarct area, and to compare whether the diffusion-weighted image high signal area was different from the core infarct area and whether distribution of cerebral infarction correlates with collateral circulation. Results The proportion of males and the proportion of hypertension patients were significantly higher in the group with poor collateral circulation than that in the group with good collateral circulation (P < 0.05). CTP results of all patients were positive, 66 cases were positive for core infarct area in 68 cases in diffusion weighted image. Two methods were consistent in the diagnosis of acute cerebral infarction. The type of cerebral infarction in the group with good collateral circulation being predominantly penetrating artery infarction, and the group with poor collateral circulation being predominantly watershed infarction. For the comparison of the perfusion parameters of the ischemic penumbra area between the two groups, the difference in cerebral blood flow value was not significant (P > 0.05), while the increase in cerebral blood volume, and the decrease in mean transit time and time to peak in the group with good collateral circulation were statistically significant (P < 0.05). Conclusion The distribution type of cerebral infarction caused by severe stenosis or occlusion of the middle cerebral artery is related to the establishment of collateral circulation. CTP imaging can detect the ischemic areas earlier, accurately assess the degree of stenosis of the responsible blood vessel and local hemodynamic information. The shadow calculation mode allows faster assessment of the ischemic core infarct area and the ischemic penumbra area. -

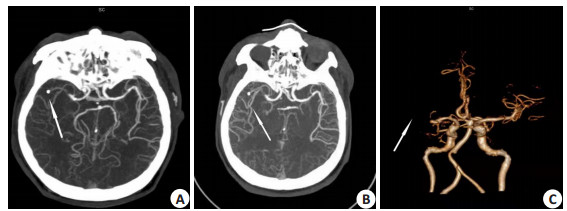
图 1 多时相CTA图
患者男, 56岁, 突发左侧肢体无力5 h; A~B: 多时相CTA MIP重建图, 箭头所示右侧大脑中动脉闭塞及周边多支侧支血管影; C: 动脉峰值VR重建图.
Figure 1. Multi-phase CTA diagram.

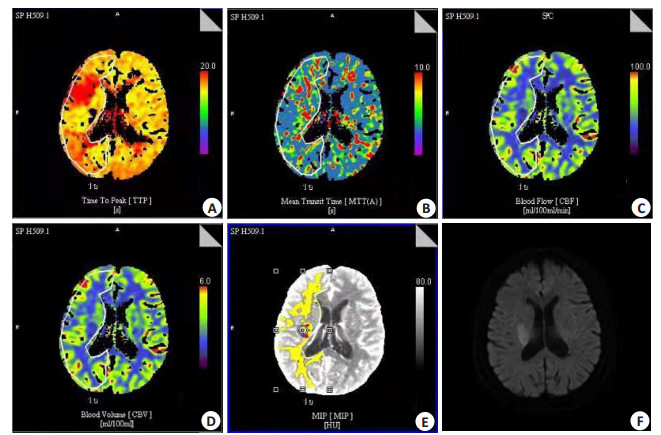
图 2 脑灌注参数图
A~D: 灌注伪彩图TTP、MTT、CVF、CBV; E: 半影计算图; F: MRI-DWI图. 该患者侧支循环建立良好,图A示右侧大脑半球见大面积灌注减低区, 但图E显示核心梗死区(红色区域)较小, 周边存在大范围缺血半暗带区(黄色区域), 经DWI成像(F)证实示右侧基底节区小斑片状高信号影与图E红色区域位置相符.
Figure 2. Diagram of cerebral perfusion parameters.
表 1 侧支循环良好组和侧支循环不良组基线资料比较
Table 1. Comparison of baseline data between good collateral circulation group and poor collateral circulation group [n(%)]
项目 侧支循环良好组 侧支循环不良组 检验值 P 年龄(岁, Mean±SD) 63.47±7.61 64.13±5.82 0.143 0.089 男性 16 (62.72) 23 (76.51) 4.890 0.023 高血脂 20 (80.61) 24 (83.13) 0.157 0.679 糖尿病 9 (35.78) 8 (26.45) 0.878 0.357 高血压 10 (37.67) 18 (60.00) 0.373 0.033 冠心病 2 (10.00) 4 (13.89) 0.067 0.829 吸烟史 6 (23.47) 8 (26.45) 3.749 0.127  下载: 导出CSV
下载: 导出CSV
表 2 核心梗死区与DWI诊断脑梗死一致性
Table 2. The consistency of the diagnosis of cerebral infarction between NVT area and DWI (n)
DWI 核心梗死区 合计 阳性 阴性 阳性 66 2 68 阴性 0 12 12 合计 66 14 80 注: 经筛选80例患者, 由2位观察者采用核心梗死区诊断脑梗死66例, DWI诊断脑梗死68例; DWI: 弥散加权成像.
下载: 导出CSV
表 3 侧支循环良好组和不良组脑梗死灶类型分布
Table 3. Distribution of cerebral infarction focus in the good collateral circulation group and poor collateral circulation group[n(%)]
组别 穿支动脉梗死 皮质支动脉梗死 大面积梗死 分水岭梗死 多发性脑梗死 无脑梗死灶 侧支循环良好组(n=48) 17 (35.4) 9 (18.3) 3 (6.3) 6 (12.6) 5 (10.4) 9 (18.3) 侧支循环不良组(n=32) 4 (12.5) 4 (12.5) 8 (25.0) 9 (28.1) 4 (12.5) 3 (9.3)
下载: 导出CSV
表 4 侧支循环良好组和不良组缺血半暗带区血流动力学值比较结果
Table 4. Comparison results of hemodynamic values in the TAR area between the good collateral circulation group and the poor collateral circulation group (Mean±SD)
组别 CBF (mL·100g-1) CBV[mL·100/ (g·min)] MTT (s) TTP (s) 侧支循环良好组(n=48) 47.32±41.35 5.46±2.27 7.98±9.26 16.73±1.62 侧支循环不良组(n=32) 41.05±24.33 3.18±1.99 12.01±8.76 25.09±0.63 t 6.126 2.364 0.018 -0.021 P 0.071 0.042 0.028 0.031 CBF:脑血流量; CBV: 脑血容量; MTT: 平均通过时间; TTP: 达峰时间.
下载: 导出CSV
-
[1] 王宇, 谭乔芮, 张元, 等. 动态功能连接分析在脑卒中近5年的应用现状[J]. 分子影像学杂志, 2021, 44(4): 714-7. doi: 10.12122/j.issn.1674-4500.2021.04.28 [2] 吴水天, 霍杰坤, 张飞. CTA、CTP对急性缺血性卒中患者梗死体积的评估价值[J]. 影像研究与医学应用, 2020, 4(14): 69-71. doi: 10.3969/j.issn.2096-3807.2020.14.030 [3] 吴晓玲, 温孟皇, 杨粤龙, 等. 源于全模型迭代CTP的多期相CTA在烟雾病中的诊断价值[J]. 临床放射学杂志, 2020, 39(1): 211-6. https://www.cnki.com.cn/Article/CJFDTOTAL-LCFS202001047.htm [4] 周建国, 符大勇, 卢明聪, 等. 3D ASL在不同程度颈动脉狭窄患者脑分水岭灌注评估中的临床应用[J]. 分子影像学杂志, 2021, 44(1): 59-62. doi: 10.12122/j.issn.1674-4500.2021.01.11 [5] 李晗, 王希明. 基于多模态CT评估缺血性脑卒中侧支循环的研究进展[J]. 中国中西医结合影像学杂志, 2021, 19(2): 184-7. doi: 10.3969/j.issn.1672-0512.2021.02.023 [6] Lindsay E. Thrombectomy 6 to 24 hours after stroke with a mismatch between defcit and infarct[J]. J Emerg Med, 2018, 54(4): 583-4. doi: 10.1016/j.jemermed.2018.02.029 [7] 张铭思, 黎红华, 骆文静, 等. 大脑中动脉重度狭窄或闭塞患者侧支循环与梗死病灶类型及脑灌注的相关研究[J]. 中国脑血管病杂志, 2019, 16(1): 16-21, 28. doi: 10.3969/j.issn.1672-5921.2019.01.005 [8] Guo LH, Hu RY, Gong WW, et al. Research progress of stroke risk factors[J]. Chin J Gerontol, 2017, 37(17): 4413-5. [9] 孙凤涛, 张厚宁, 禹璐, 等. 多模式CT检查在缺血性脑卒中侧支循环评估中的价值[J]. 放射学实践, 2021, 36(5): 584-9. https://www.cnki.com.cn/Article/CJFDTOTAL-FSXS202105009.htm [10] Lu SS, Zhang X, Xu XQ, et al. Comparison of CT angiography collaterals for predicting target perfusion profile and clinical outcome in patients with acute ischemic stroke[J]. Eur Radiol, 2019, 29(9): 4922-9. doi: 10.1007/s00330-019-06027-9 [11] 朱石柱, 黄立雪, 程浩, 等. CT血管成像和MRI对急性缺血性脑卒中侧支循环的诊断价值分析[J]. 实用医院临床杂志, 2021, 18(3): 60-4. https://www.cnki.com.cn/Article/CJFDTOTAL-YYLC202103020.htm [12] 钟迪, 张舒婷, 吴波. 《中国急性缺血性脑卒中诊治指南2018》解读[J]. 中国现代神经疾病杂志, 2019, 19(11): 897-901. doi: 10.3969/j.issn.1672-6731.2019.11.015 [13] 郝璐, 陈欢, 王红. MRI-PWI对症状性卒中患者脑血流灌注及侧支循环建立评价[J]. 磁共振成像, 2020, 11(10): 904-7. doi: 10.12015/issn.1674-8034.2020.10.014 [14] Jia BX, Feng L, Liebeskind DS, et al. Mechanical thrombectomy and rescue therapy for intracranial large artery occlusion with underlying atherosclerosis[J]. J NeuroIntervent Surg, 2018, 10(8): 746-50. doi: 10.1136/neurintsurg-2017-013489 [15] 侯聪, 侯姗姗, 张俊, 等. 动脉自旋标记技术在急性脑梗死中的应用进展[J]. 分子影像学杂志, 2020, 43(4): 563-7. doi: 10.12122/j.issn.1674-4500.2020.04.02 [16] 郭丽花, 胡如英, 龚巍巍, 等. 脑卒中危险因素研究进展[J]. 中国老年学杂志, 2017, 37(17): 4413-6. doi: 10.3969/j.issn.1005-9202.2017.17.119 [17] D'Esterre CD, Trivedi A, Pordeli P, et al. Regional comparison of multiphase computed tomographic angiography and computed tomographic perfusion for prediction of tissue fate in ischemic stroke[J]. Stroke, 2017, 48(4): 939-45. doi: 10.1161/STROKEAHA.116.015969 [18] 闫海清, 王桂华, 岳军艳, 等. 颅内大动脉狭窄性缺血性脑卒中患者不同时间点侧支循环的功能评价[J]. 脑与神经疾病杂志, 2020, 28(4): 230-4. https://www.cnki.com.cn/Article/CJFDTOTAL-LYSJ202004009.htm [19] 叶国伟, 许兵, 邹建勋, 等. 多模式CT定量评估急性缺血性脑卒中侧支循环及缺血半暗带与预后的应用[J]. 医学影像学杂志, 2020, 30 (10): 1757-60. https://www.cnki.com.cn/Article/CJFDTOTAL-XYXZ202010002.htm [20] 刘蓉, 朱江涛, 龚建平, 等. 利用CTA的侧支循环评分预测大脑中动脉M1段闭塞后脑梗死体积及分布情况[J]. 放射学实践, 2016, 31 (10): 919-23. https://www.cnki.com.cn/Article/CJFDTOTAL-FSXS201610004.htm [21] 周坤元, 李水彬, 成钢卫, 等. 进展性缺血性卒中患者的影像学特点及与脑动脉狭窄之间的关系[J]. 中国医药科学, 2016, 6(7): 25-8. https://www.cnki.com.cn/Article/CJFDTOTAL-GYKX201607009.htm -

 点击查看大图
点击查看大图
计量
- 文章访问数: 266
- HTML全文浏览量: 192
- PDF下载量: 6
- 被引次数: 0