



Prognostic factors of neuroendocrine carcinoma of the cervix: a retrospective study
-
摘要:
目的 探讨影响宫颈神经内分泌癌预后的因素。 方法 回顾性分析2009年12月~2020年7月收治于广州医科大学附属肿瘤医院的30例宫颈神经内分泌癌患者的临床病理资料、治疗方案,随访截止至2021年3月31日,对数据进行单因素和多因素生存分析。 结果 中位随访时间为43(9~135)月,中位无进展生存时间和总生存时间分别为16(1~102)月、19(3~102)月,中位年龄为44.5岁(21~65岁)。截至随访日期,13例(43.3%)患者存活。单因素分析表明,手术(P < 0.001)、化疗(P=0.018)、盆腔淋巴结转移(P=0.006)以及分期(P=0.014)对无进展生存时间有影响。手术和盆腔淋巴结转移对总生存时间具有影响(P < 0.001,P= 0.033)。Cox回归模型多因素分析表明,手术及化疗是影响无进展生存时间的两个独立因素(P=0.002,P=0.005),手术是影响总生存时间的唯一独立因素(P=0.002)。年龄、分期、肿瘤大小、病理类型、盆腔淋巴结转移、化疗疗程及放疗均不是影响预后的独立因素。 结论 宫颈神经内分泌癌的预后与是否行手术和化疗密切相关,适合手术的患者应行手术治疗,化疗作为辅助治疗可使患者生存受益,即使早期患者也建议联合化疗。 Abstract:Objective To analyze prognostic factors of patients with neuroendocrine carcinoma of the cervix (NECC). Methods Thirty patients with NECC between December 2009 and July 2020 in Affiliated Cancer Hospital & Institute of Guangzhou Medical University were retrospectively reviewed. Clinicopathologic characteristics and primary treatments were reviewed. The end of the follow-up time was March 31st, 2021.The factors were analyzed using Kaplan- Meier and Cox regression methods. Results With a median follow-up of 43 months (9-135 months), 13 (43.3%) patients were alive. The median PFS was 16 months (1-102 months), median OS was 19 months (3-102 months). The median age was 44.5 years (21-65 years). Univariate analysis showed that surgery (P < 0.001), chemotherapy (P=0.018), pelvic lymph node metastasis (P=0.006) and stage (P=0.014) were significant prognostic factors for PFS. For OS, only surgery and pelvic lymph node metastasis were significant prognostic factors(P < 0.001, P=0.033). In multivariate analyses, surgeryand chemotherapy were independent prognostic factors for PFS (P= 0.002, P=0.005). Surgery was the sole independent prognostic factor for OS (P=0.002). Age, stage, tumor size, histology, pelvic lymph node metastasis, cycles of chemotherapy and radiotherapy were not independent prognostic factors. Conclusion The prognosis of NECC is closely related with surgery and chemotherapy. Patients with indication for surgery should be treated with it. Chemotherapy was advised as adjuvant therapy even in early stage. -
Key words:
- neuroendocrine carcinoma of the cervix /
- surgery /
- chemotherapy /
- radiotherapy
-

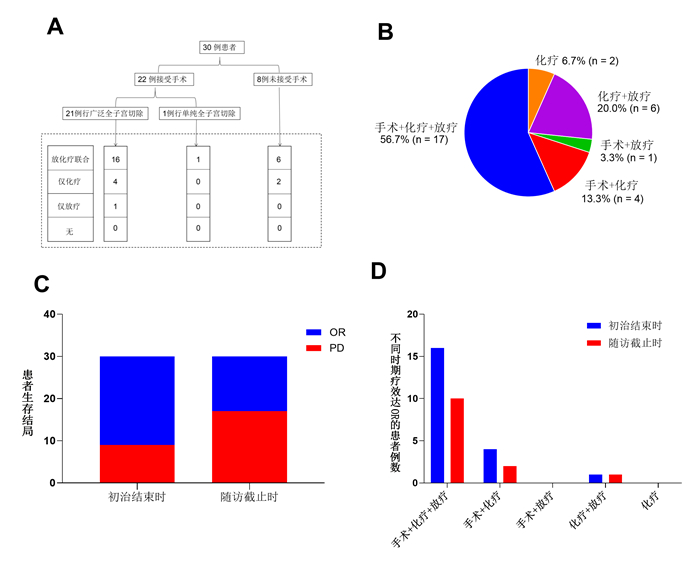
图 1 初始治疗方案及结局
A~B: 患者的初始治疗方案; C: 初始治疗和随访的结果; D: 初始治疗和随访结束后达到客观缓解的患者数.
Figure 1. The primary treatments and outcomes.

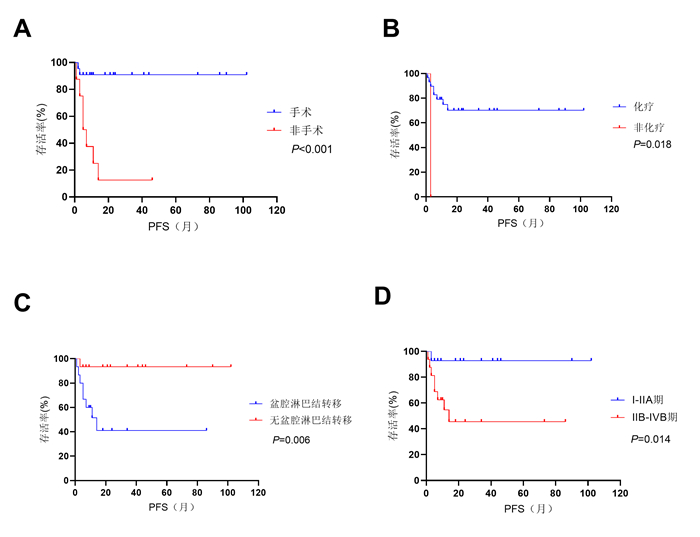
图 2 单因素分析中对PFS的有统计学意义的因素
A: 手术; B: 化疗; C: 盆腔淋巴结转移; D: 分期
Figure 2. Significant prognostic factors of progression-free survival by univariate analysis.

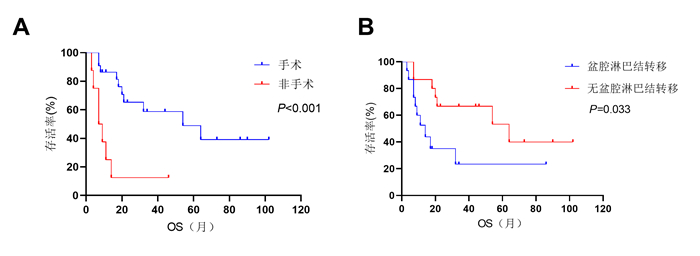
图 3 单因素分析中对OS的有统计学意义的因素
A: 手术; B: 盆腔淋巴结转移
Figure 3. Significant prognostic factors of overall survival by univariate analysis.
表 1 临床病例特征分析
Table 1. Clinicopathologic characteristics
临床病理因素 例数 百分比(%) 年龄(岁) < 45 16 53.3 > 45 14 46.7 病理组织学分型 SCNEC 29 96.7 LCNEC 1 3.3 病理组织同源性 单一型 23 76.7 混合型 7 23.3 分期(FIGO2009) I~IIA期 18 60.0 IIB~IVB期 12 40.0 分期(FIGO2018) I~IIA期 14 46.7 IIB~IVB期 16 53.3 肿瘤大小(cm) < 4 9 30.0 > 4 21 70.0 盆腔淋巴结转移 有 15 50.0 无 15 50.0 手术 有 22 73.3 无 8 26.7 化学治疗 有 29 96.7 无 1 3.3 化疗疗程 < 5疗程 19 65.5 > 5疗程 10 34.5 放射治疗 有 24 80.0 无 6 20.0 盆腔外照射放疗 有 24 100.0 无 0 0.0 后装放疗 有 7 29.2 无 17 70.8 SCNEC: 小细胞神经内分泌癌; LCNEC: 大细胞神经内分泌癌; EBRT: 外照射放射治疗; FIGO: 国际妇产科联盟.  下载: 导出CSV
下载: 导出CSV
表 2 NECC单因素分析统计结果
Table 2. Univariate analysis of prognostic factors for NECC
因素 PPFS Pos 年龄(≤45岁vs >45岁) 0.880 0.884 病理组织同源性(单一型vs混合型) 0.053 0.196 分期(I-IIA期vs IIB-IVB期) 0.014 0.142 肿瘤大小(< 4 cm vs ≥4 cm) 0.180 0.390 盆腔淋巴结转移(有vs无) 0.006 0.033 手术(有vs无) < 0.001 < 0.001 化疗(有vs无) 0.018 0.650 化疗疗程(< 5 vs ≥ 5) 0.070 0.597 放疗(有vs无) 0.755 0.684 盆腔外照射(有vs无) 0.755 0.684 后装(有vs无) 0.780 0.465
下载: 导出CSV
表 3 NECC多因素分析统计结果
Table 3. Multivariate analyses of prognostic factors for NECC
因素 手术 化疗 HR (95% CI) P HR (95% CI) P PFS 0.036 (0.004~0.299) 0.002 0.014 (0.001~0.265) 0.005 OS 0.186 (0.064~0.536) 0.002 - - PFS: 无进展生存时间; OS: 总生存时间.
下载: 导出CSV
-
[1] Tempfer CB, Tischoff I, Dogan A, et al. Neuroendocrine carcinoma of the cervix: a systematic review of the literature[J]. BMC Cancer, 2018, 18(1): 530. doi: 10.1186/s12885-018-4447-x [2] Lei J, Andrae B, Ploner A, et al. Cervical screening and risk of adenosquamous and rare histological types of invasive cervical carcinoma: population based nested case-control study[J]. BMJ, 2019, 365: l1207. http://www.researchgate.net/publication/332199726_Cervical_screening_and_risk_of_adenosquamous_and_rare_histological_types_of_invasive_cervical_carcinoma_Population_based_nested_case-control_study [3] Albores-Saavedra J, Gersell D, Gilks CB, et al. Terminology of endocrine tumors of the uterine cervix: results of a workshop sponsored by the College of American Pathologists and the National Cancer Institute[J]. Arch Pathol Lab Med, 1997, 121(1): 34-9. http://www.researchgate.net/publication/14107250_Terminology_of_endocrine_tumors_of_the_uterine_cervix_Results_of_a_workshop_sponsored_by_the_College_of_American_Pathologists_and_the_National_Cancer_Institute [4] Lee SW, Nam JH, Kim DY, et al. Unfavorable prognosis of small cell neuroendocrine carcinoma of the uterine cervix: a retrospective matched case-control study[J]. Int J Gynecol Cancer, 2010, 20(3): 411-6. doi: 10.1111/IGC.0b013e3181ce427b [5] Ishikawa M, Kasamatsu T, Tsuda H, et al. A multi- center retrospective study of neuroendocrine tumors of the uterine cervix: Prognosis according to the new 2018 staging system, comparing outcomes for different chemotherapeutic regimens and histopathological subtypes [J]. Gynecol Oncol, 2019, 155(3): 444-51. doi: 10.1016/j.ygyno.2019.09.018 [6] Gadducci A, Carinelli S, Aletti G. Neuroendrocrine tumors of the uterine cervix: a therapeutic challenge for gynecologic oncologists [J]. Gynecol Oncol, 2017, 144(3): 637-46. doi: 10.1016/j.ygyno.2016.12.003 [7] Burzawa J, Gonzales N, Frumovitz M. Challenges in the diagnosis and management of cervical neuroendocrine carcinoma[J]. Expert RevAnticancer Ther, 2015, 15(7): 805-10. doi: 10.1586/14737140.2015.1047767 [8] Cohen JG, Kapp DS, Shin JY, et al. Small cell carcinoma of the cervix: treatment and survival outcomes of 188 patients[J]. Am J Obstet Gynecol, 2010, 203(4): 347. e1-6. http://www.sciencedirect.com/science?_ob=ShoppingCartURL&_method=add&_eid=1-s2.0-S0002937810004321&originContentFamily=serial&_origin=article&_ts=1495735074&md5=ad53ed4236265ec43b754098e97cb99b [9] Zivanovic O, Leitao MM, Park KJ, et al. Small cell neuroendocrine comcarcinoma of the cervix: Analysis of outcome, recurrence pattern and the impact of platinum-based combination chemotherapy[J]. Gynecol Oncol, 2009, 112(3): 590-3. doi: 10.1016/j.ygyno.2008.11.010 [10] Margolis B, Tergas AI, Chen L, et al. Natural history and outcome of neuroendocrine carcinoma of the cervix[J]. Gynecol Oncol, 2016, 141(2): 247-54. doi: 10.1016/j.ygyno.2016.02.008 [11] Gardner GJ, Reidy-Lagunes D, Gehrig PA. Neuroendocrine tumors of the gynecologic tract: a Society of Gynecologic Oncology (SGO) clinical document [J]. Gynecol Oncol, 2011, 122(1): 190-8. doi: 10.1016/j.ygyno.2011.04.011 [12] Satoh T, Takei Y, Treilleux I, et al. Gynecologic Cancer InterGroup (GCIG) consensus review for small cell carcinoma of the cervix[J]. Int J Gynecol Cancer, 2014, 24(9 suppl 3): S102-8. http://www.onacademic.com/detail/journal_1000037563044810_0ec9.html [13] Cho WK, Park W, Kim YS, et al. Optimal treatment strategies for small cell carcinoma of the uterine cervix: a retrospective multicenter study (KROG 19-03)[J]. Eur J Obstet Gynecol Reprod Biol, 2021, 258: 396-400. doi: 10.1016/j.ejogrb.2021.01.034 [14] Lin LM, Lin Q, Liu J, et al. Prognostic factors and treatment comparison in small cell neuroendocrine carcinoma of the uterine cervix based on population analyses[J]. Cancer Med, 2020, 9(18): 6524-32. doi: 10.1002/cam4.3326 [15] Viswanathan AN, Deavers MT, Jhingran A, et al. Small cell neuroendocrine carcinoma of the cervix: outcome and patterns of recurrence[J]. Gynecol Oncol, 2004, 93(1): 27-33. doi: 10.1016/j.ygyno.2003.12.027 [16] Chan JK, Loizzi V, Burger RA, et al. Prognostic factors in neuroendocrine small cell cervical carcinoma: a multivariate analysis [J]. Cancer, 2003, 97(3): 568-74. doi: 10.1002/cncr.11086 [17] Pei X, Xiang L, Ye S, et al. Cycles of cisplatin and etoposide affect treatment outcomes in patients with FIGO stage I-II small cell neuroendocrine carcinoma of the cervix[J]. Gynecol Oncol, 2017, 147(3): 589-96. doi: 10.1016/j.ygyno.2017.09.022 [18] Atienza-Amores M, Guerini-Rocco E, Soslow RA, et al. Small cell carcinoma of the gynecologic tract: a multifaceted spectrum of lesions [J]. Gynecol Oncol, 2014, 134(2): 410-8. doi: 10.1016/j.ygyno.2014.05.017 [19] Lee JM, Lee KB, Nam JH, et al. Prognostic factors in FIGO stage IBIIA small cell neuroendocrine carcinoma of the uterine cervix treated surgically: results of a multi- center retrospective Korean study[J]. Ann Oncol, 2008, 19(2): 321-6. doi: 10.1093/annonc/mdm465 [20] Chen J, Sun Y, Chen L, et al. Prognostic factors and treatment of neuroendocrine tumors of the uterine cervix based on the FIGO 2018 staging system: a single-institution study of 172 patients[J]. PeerJ, 2021, 9: e11563. doi: 10.7717/peerj.11563 [21] Frumovitz M, Munsell MF, Burzawa JK, et al. Combination therapy with topotecan, paclitaxel, and bevacizumab improves progressionfree survival in recurrent small cell neuroendocrine carcinoma of the cervix[J]. Gynecol Oncol, 2017, 144(1): 46-50. doi: 10.1016/j.ygyno.2016.10.040 [22] Sharabi A, Kim SS, Kato S, et al. Exceptional response to nivolumab and stereotactic body radiation therapy (SBRT) in neuroendocrine cervical carcinoma with high tumor mutational burden: management considerations from the center for personalized cancer therapy at UC San diego moores cancer center [J]. Oncologist, 2017, 22(6): 631-7. doi: 10.1634/theoncologist.2016-0517 [23] Paraghamian SE, Longoria TC, Eskander RN. Metastatic small cell neuroendocrine carcinoma of the cervix treated with the PD-1 inhibitor, nivolumab: a case report[J]. Gynecol Oncol Res Pract, 2017, 4: 3 doi: 10.1186/s40661-017-0038-9 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 286
- HTML全文浏览量: 147
- PDF下载量: 5
- 被引次数: 0