



Diagnostic value of high frequency ultrasound for wrist and knuckle lesions in patients with rheumatoid arthritis
-
摘要:
目的 分析高频超声对类风湿性关节炎(RA)患者腕、指关节病变的诊断价值。 方法 回顾性收集2019年1月~2020年12月北京市海淀医院收治的60例RA患者的临床资料作为RA组,另选取在北京市海淀医院进行体检的60例健康体检者的体检资料作为健康对照组,所有患者均进行高频超声检查。比较两组一般资料、各关节滑膜厚度及关节积液、肌腱腱鞘炎、滑膜增厚、骨侵蚀及血管翳检出情况,统计RA患者各关节滑膜增厚、血管翳分布情况。 结果 RA组腕关节、掌指关节、近节指间关节滑膜厚度均厚于健康对照组(P < 0.05)。RA组各关节关节积液、肌腱腱鞘炎、滑膜增厚、骨侵蚀及血管翳检出率(20.53%、1.89%、36.59%、3.56%、5.83%)均高于健康对照组(7.95%、0.15%、2.58%、0.38%、0.53%,P < 0.05)。RA患者腕关节滑膜增厚、血管翳(64.17%、18.33%)高于掌指关节、近节指间关节(52.00%、7.17%,31.50%、5.83%,P < 0.05),掌指关节高于近节指间关节(P < 0.05)。 结论 高频超声可较好显示RA患者腕关节和指关节病变情况,已经成为诊断RA的有效影像学检查方法。 Abstract:Objective To analyze the diagnostic value of high frequency ultrasound for wrist and knuckle lesions in patients with rheumatoid arthritis (RA). Methods Clinical data of 60 patients with RA admitted to Beijing Haidian Hospital from January 2019 to December 2020 were retrospectively collected as the RA group.The physical data of 60 healthy patients who underwent physical examination in Beijing Haidian Hospital were selected as the healthy control group. All patients underwent high- frequency ultrasound examination. The general data, synovial thickness, joint effusion, tenosynovitis, synovial thickening, bone erosion and pannus were compared between the two groups, and the distribution of synovial thickening and pannus in the joints of RA patients statistically analyzed. Results Synovial thickness of carpal joint, metacarpophalangeal joint and proximal interphalangeal joint in the RA group were higher than those in the healthy control group (P < 0.05). The detection rates of joint effusion, tenosynovitis, synovial thickening, bone erosion and pannus of each joint in the RA group (20.53%, 1.89%, 36.59%, 3.56%, 5.83%) were higher than those in the healthy control group (7.95%, 0.15%, 2.58%, 0.38%, 0.53%, P < 0.05). The synovial thickening and pannus distribution of various joints in RA patients were higher in carpal joint (64.17%, 18.33%) than in metacarpophalangeal joint (52.00%, 7.17%, 31.50%, 5.83%, P < 0.05), and which in metacarpophalangeal joint was higher than in proximal interphalangeal joint (P < 0.05). Conclusion High-frequency ultrasound could better display the pathological conditions of wrist and knuckle joints in RA patients, and had become an effective imaging examination method for RA diagnosis. -
Key words:
- rheumatoid arthritis /
- high-frequency ultrasound /
- wrist joint /
- finger joint /
- value
-

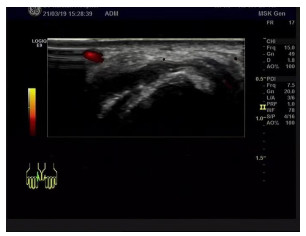
图 1 掌指关节高频超声检查图分析
Figure 1. Analysis of high frequency ultrasonic examination of metacarpophalangeal joint

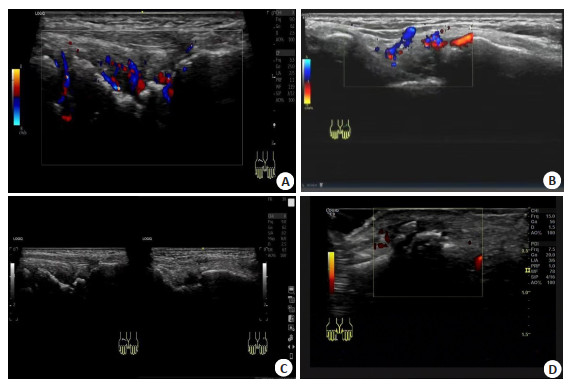
图 2 腕关节高频超声检查图分析
A: 患者女, 50岁, 类风湿关节炎10年, 近日加重来诊. 患者腕关节腔积液、滑膜增厚、血供丰富(炎症活跃期); B: 患者女, 39岁, 类风湿关节炎3年, 反复发作. 患者腕关节腔积液、滑膜增厚、血供丰富(炎症活跃期); C: 患者女, 70岁, 类风湿关节炎病史15年. 腕关节双侧对比扫查, 双侧腕关节腔积液, 滑膜增厚, 右侧腕关节骨侵蚀明显; D: 患者女, 59岁, 类风湿关节炎病史6年, 右手第二指近节指间关节少量积液、滑膜增厚, 骨侵蚀.
Figure 2. Analysis of high-frequency ultrasound of wrist joint
表 1 两组患者一般资料比较
Table 1. Comparison of general data between the two groups (n=60, Mean±SD)
组别 性别[n(%)] 年龄(岁) BMI(kg/m2) 收缩压(mmHg) 舒张压(mmHg) 男 女 RA组 35(58.33) 25(41.67) 48.43±12.45 24.73±3.66 126.55±13.10 79.74±9.31 健康对照组 37(61.67) 23(38.33) 49.55±13.67 25.86±3.97 125.71±14.73 81.10±9.64 χ2/t 0.139 1.931 1.621 0.330 0.786 P 0.709 0.056 0.108 0.742 0.433 RA: 类风湿性关节炎  下载: 导出CSV
下载: 导出CSV
表 2 两组各关节滑膜厚度比较
Table 2. Comparison of synovial thickness between the two groups (n=60, mm, Mean±SD)
组别 腕关节 掌指关节 近节指间关节 RA组 2.56±0.85 2.34±0.68 1.51±0.38 健康对照组 1.96±0.31 1.94±0.55 0.85±0.39 t 5.137 3.543 9.389 P < 0.001 0.001 < 0.001
下载: 导出CSV
表 3 两组各关节关节积液、肌腱腱鞘炎、滑膜增厚、骨侵蚀及血管翳检出情况比较
Table 3. Comparison of joint effusion, tenosynovitis, synovial thickening, bone erosion and pannus between the two groups[n(%)]
组别 关节数 关节积液 肌腱腱鞘炎 滑膜增厚 骨侵蚀 血管翳 RA组 1320 271(20.53) 25(1.89) 483(36.59) 47(3.56) 77(5.83) 健康对照组 1320 105(7.95) 2(0.15) 34(2.58) 5(0.38) 7(0.53) χ2 - 84.729 19.795 484.904 34.605 61.863 P _ < 0.001 < 0.001 < 0.001 < 0.001 < 0.00
下载: 导出CSV
表 4 RA患者各关节滑膜增厚、血管翳分布情况
Table 4. Distribution of synovial thickening and pannus in RA patients[n(%)]
关节名称 滑膜增厚 血管翳 腕关节(n=120) 77(64.17) 22(18.33) 掌指关节(n=600) 312(52.00)* 43(7.17)* 近节指间关节(n=600) 189(31.50)*# 35(5.83)*# χ2 73.492 29.732 P < 0.001 < 0.001 *P < 0.05 vs腕关节; #P < 0.05 vs掌指关节
下载: 导出CSV
-
[1] England BR, Thiele GM, Anderson DR, et al. Increased cardiovascular risk in rheumatoid arthritis: mechanisms and implications[J]. BMJ, 2018, 361: k1036. [2] 秦龙燕, 罗英亮, 刘俊, 等. 血清sPD-1和sPD-L1对类风湿关节炎的诊断价值及其与疾病活动度的相关性[J]. 贵州医科大学学报, 2021, 46(7): 805-11. https://www.cnki.com.cn/Article/CJFDTOTAL-GYYB202107010.htm [3] Giannini D, Antonucci M, Petrelli F, et al. One year in review 2020: pathogenesis of rheumatoid arthritis[J]. Clin Exp Rheumatol, 2020, 38(3): 387-97. [4] Croia C, Bursi R, Sutera D, et al. One year in review 2019: pathogenesis of rheumatoid arthritis[J]. Clin Exp Rheumatol, 2019, 37(3): 347-57. [5] 中华医学会风湿病学分会. 类风湿关节炎诊断及治疗指南[J]. 中华风湿病学杂志, 2010, 14(4): 265-70. doi: 10.3760/cma.j.issn.1007-7480.2010.04.014 [6] Wasserman A. Rheumatoid arthritis: common questions about diagnosis and management[J]. Am Fam Physician, 2018, 97(7): 455-62. [7] Derksen VFAM, Huizinga TWJ, van der Woude D. The role of autoantibodies in the pathophysiology of rheumatoid arthritis[J]. Semin Immunopathol, 2017, 39(4): 437-46. doi: 10.1007/s00281-017-0627-z [8] De Cock D, Hyrich K. Malignancy and rheumatoid arthritis: Epidemiology, risk factors and management[J]. Best Pract Res Clin Rheumatol, 2018, 32(6): 869-86. doi: 10.1016/j.berh.2019.03.011 [9] Abbasi M, Mousavi MJ, Jamalzehi S, et al. Strategies toward rheumatoid arthritis therapy; the old and the new[J]. J Cell Physiol, 2019, 234(7): 10018-31. doi: 10.1002/jcp.27860 [10] van der Woude D, van der Helm-van Mil AHM. Update on the epidemiology, risk factors, and disease outcomes of rheumatoid arthritis[J]. Best Pract Res Clin Rheumatol, 2018, 32(2): 174-87. doi: 10.1016/j.berh.2018.10.005 [11] Cramp F. The role of non-pharmacological interventions in the management of rheumatoid-arthritis-related fatigue[J]. Rheumatology: Oxford, 2019, 58(suppl 5): v22-8. http://www.researchgate.net/publication/337030526_The_role_of_non-pharmacological_interventions_in_the_management_of_rheumatoid-arthritis-related_fatigue/download [12] 张天成, 戚子荣, 余俊文. 从少阳经论治类风湿性关节炎探析[J]. 环球中医药, 2019, 12(7): 1048-50. doi: 10.3969/j.issn.1674-1749.2019.07.014 [13] Evangelatos G, Fragoulis GE, Koulouri V, et al. MicroRNAs in rheumatoid arthritis: From pathogenesis to clinical impact[J]. Autoimmun Rev, 2019, 18(11): 102391. doi: 10.1016/j.autrev.2019.102391 [14] 朱艳, 俞红五, 潘喻珍, 等. 艾灸强壮穴治疗类风湿关节炎[J]. 长春中医药大学学报, 2020, 36(1): 99-102 https://www.cnki.com.cn/Article/CJFDTOTAL-CZXX202001028.htm [15] Lin YJ, Anzaghe M, Schülke S. Update on the pathomechanism, diagnosis, and treatment options for rheumatoid arthritis[J]. Cells, 2020, 9(4): 880. doi: 10.3390/cells9040880 [16] Forsyth C, Kouvari M, D'Cunha NM, et al. The effects of the Mediterranean diet on rheumatoid arthritis prevention and treatment: a systematic review of human prospective studies[J]. Rheumatol Int, 2018, 38(5): 737-47. doi: 10.1007/s00296-017-3912-1 [17] Amaral JK, Bilsborrow JB, Schoen RT. Chronic chikungunya arthritis and rheumatoid arthritis: what they have in common[J]. Am J Med, 2020, 133(3): e91-7. doi: 10.1016/j.amjmed.2019.10.005 [18] 刘淑清, 吉缤郡, 葛华迅, 等. 益气补肾活血方对肾虚血瘀型类风湿关节炎患者IL-6和IL-17的影响[J]. 中医药信息, 2020, 37(6): 93-6. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYXN202006021.htm [19] 蔡军. 联合检测类风湿因子IgM-RF、IgG-RF、IgA-RF及抗环瓜氨酸肽抗体对早期诊断类风湿性关节炎的价值研究[J]. 贵州医药, 2021, 45(4): 522-4. doi: 10.3969/j.issn.1000-744X.2021.04.006 [20] 任燕, 张斐娜. 类风湿关节炎患者血红蛋白水平与疾病活动度相关性分析[J]. 贵州医药, 2021, 45(2): 183-5. doi: 10.3969/j.issn.1000-744X.2021.02.005 [21] Aletaha D, Smolen JS. Diagnosis and management of rheumatoid arthritis: a review[J]. JAm MedAssoc, 2018, 320(13): 1360-72. doi: 10.1001/jama.2018.13103 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 176
- HTML全文浏览量: 117
- PDF下载量: 2
- 被引次数: 0