



86 b/min may be a reliable clinical indicator between hypertensive emergency and hypertensive urgency
-
摘要:
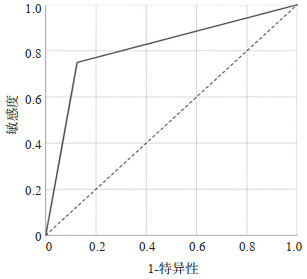
目的 分析在急诊科首诊的高血压危象的患者的心率及血压参数,探讨心率在高血压急症与高血压亚急症的不同变化。 方法 选取2019年1~12月于我院急诊科首诊的高血压危象患者186例,根据是否存在急性靶器官损害将患者分为高血压急症组(n=82)及高血压亚急症组(n=104),分析两组间的临床特点、服用药物种类及数量、服药依从性、血压参数与心率的差异;分析主要不同类型的高血压急症患者的血压参数和心率的组间差异;分析高血压急症组及高血压亚急症组中存在差异的因素对高血压危象中高血压急症患者的预测价值及心率对高血压危象患者中高血压急症的诊断价值。 结果 186例急诊科首诊的窦性心律并高血压急象患者中,高血压急症占44.1%,高血压亚急症占55.9%。女性平均心率高于男性(93±16.7次/min vs 85±18.2次/min,P=0.002)。高血压急症组的平均心率高于亚急症组(98±20.5次/min vs 82 ±12.7次/min,P < 0.001)。与亚急症组相比,高血压急症组中合并糖尿病比例高、服药依从性较差;两组收缩压、舒张压、平均动脉压、脉压差等血压参数比较,差异均无统计学意义(P>0.05)。糖尿病史与心率对高血压危象患者发生高血压急症存在预测价值,心率诊断高血压急症的最佳切点为86次/ min,曲线下面积为0.813。 结论 高血压急症特别是合并急性心衰的患者的平均心率高于高血压亚急症的平均心率,以心率86次/min为阈值可能是鉴别高血压危象中高血压急症或亚急症的简易临床指标,特别适合急诊科诊治思维特点;合并糖尿病的高血压危象患者,更易发生高血压急症。 Abstract:Objective To explore differences of heart rate between hypertensive emergency and hypertensive urgency. Methods The data of patients with hypertensive crisis presenting to emergency department of Shantou Central Hospital between January 2019 and December 2019 was documented. Based on the presence or absence of acute target organ involvement, clustering of hypertensive crisis into emergency or urgency. The relationship between clinical characteristics, types and quantities of medications taken, medication compliance, blood pressure parameters and heart rate were analyzed. The differences in blood pressure parameters and heart rate among different types of hypertensive emergency patients were analyzed. The different predictors between hypertensive emergency and hypertensive urgency were used to analyze the predictive value for hypertensive emergency patients in hypertensive crisis. The value of heart rate in diagnosing hypertensive emergency was analyzed. Results A total of 186 patients of hypertensive crisis in sinus rhythm presenting to emergency department were enrolled. Hypertensive emergency accounted for 44.1%, and hypertensive urgency accounted for 55.9%. The average heart rate of women was higher than men (P=0.002). The average heart rate of the hypertensive emergency was higher than those with urgency (P < 0.001). Compared with urgency, hypertensive emergency has a higher proportion of diabetes and poor medication compliance; and hemodynamic parameters including systolic blood pressure, diastolic blood pressure, mean arterial pressure, and pulse pressure relates neither to urgency nor to emergency. Finally, hypertensive emergency in hypertensive crisis patients may be predicted by diabetes mellitus and heart rate. The area under the curve and optimal cut-off value of heart rate to diagnose hypertensive emergency were 0.813 and 86 b/min. Conclusion Hemodynamic parameters relate neither to hypertensive emergency nor to urgency. The mean heart rate of hypertensive emergencies, especially those with acute heart failure, is higher than that of hypertension urgencies. The heart rate threshold of 86 b/min may be a reliable clinical indicator for distinguishing hypertensive emergency or urgency in hypertensive crisis. It is especially suitable for the clinical thinking of diagnosis and treatment in emergency department. In addition, hypertensive crisis patients with diabetes are more prone to emergency. -
Key words:
- hypertensive crisis /
- heart rate /
- hypertensive emergency /
- hypertensive urgency
-

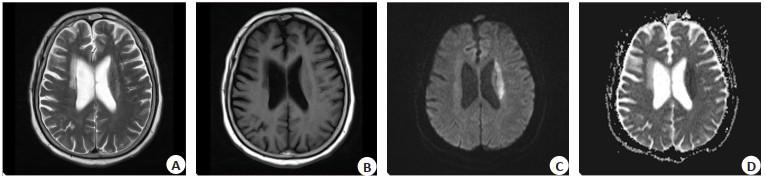
图 2 左侧放射冠斑片状新近脑梗塞1例
A: T2WI显示左侧放射冠斑片状呈稍高信号; B: T1WI显示左侧放射冠斑片状呈稍低信号; C: DWI显示左侧放射冠斑片状呈高信号; D: ADC显示左侧放射冠斑片状呈低信号.
Figure 2. A case of patchy recent cerebral infarction in the left radial crown.
表 1 高血压急症组与亚急症组临床特点比较
Table 1. Clinical characteristics between hypertensive emergency and urgency
变量 HE组(n=82) HU组(n=104) F/t/χ2 P 性別(男/女, n) 52/30 63/41 0.156 0.692 年龄(岁,Mean±SD) 58.6±12.5 53.4±11.4 2.103 0.412 是否吸烟[是,n(%)] 67(81.7) 83(79.8) 0.106 0.745 BMI(kg/m2, Mean±SD) 22.7±5.2 21.3±7.2 1.653 0.502 高血压病程(月) 42(1-250) 45(1-280) 2.634 0.308 合并糖尿病[n(%)] 53(64.6) 23(22.1) 34.3 < 0.001 服用药物种类[n(%)] β-RB 26(31.7) 28 (26.9) 0.509 0.475 ACEI 12(14.6) 17(16.3) 0.102 0.749 ARB 28(34.1) 29(27.9) 0.846 0.358 CCB 29(35.4) 33(31.74) 0.273 0.602 α-RB 6(7.3) 8(7.7) 0.009 0.923 阿司匹林 12(14.6) 9(8.7) 1.637 0.201 氯吡格雷 18(22.0) 15 (14.4) 1.780 0.182 他汀类 11(13.4) 10(9.6) 0.661 0.416 服用药物种类数量[n(%)] 未服药 9(8.4) 10(9.6) 0.092 0.761 服1种药物 34(41.5) 42(40.4) 0.022 0.882 服2种药物 28(34.1) 37(35.6) 0.041 0.839 服3种或以上药物 11(13.4) 12(11.5) 0.149 0.700 服药依从性差 22(26.8) 13(12.5) 6.163 0.013 合并的急性靶器官损害类型[n(%)] AS 26(31.7) 0 - - AHF 22(26.8) 0 - - ACS 16(19.5) 0 - - ACH 12(14.6) 0 - - AAD 5(6.1) 0 - - AKI 6 (7.3) 0 - - 2种及以上靶器官损害 5(6.1) 0 - - HE: 高血压急症; HU: 高血压亚急症; β-RB: β受体阻滞剂; ACEI: 血管紧张素转化酶抑制剂; ARB: 血管紧张素Ⅱ受体拮抗剂; CCB: 钙通道阻滞剂; α-RB: α受体阻滞剂; AS: 急性脑卒中; AHF: 急性心力衰竭; ACS: 急性冠脉综合征; ACH: 急性脑出血; AAD: 急性主动脉夹层; AKI: 急性肾损伤.  下载: 导出CSV
下载: 导出CSV
表 2 高血压急症与亚急症的心率及血压参数的比较
Table 2. Heart rate and hemodynamic parameters between hypertensive emergency and urgency (Mean±SD)
组别 心率(次/min) 收缩压(mmHg) 舒张压(mmHg) 平均动脉压(mmHg) 脉压差(mmHg) HE组(n=82) 98±20.5 201±17.7 112±16.5 142±14.5 87±21.3 HU组(n=104) 82±12.7 204±16.4 108±12.5 139±15.3 84±22.4 t 6.530 1.216 1.881 1.358 0.927 P < 0.001 0.226 0.062 0.176 0.355
下载: 导出CSV
表 3 不同主要高血压急症类型亚组心率及血压参数的比较
Table 3. Heart rate and hemodynamic variables among different main types of hypertensive emergency groups (Mean±SD)
不同主要高血压急症 心率(次/min) 收缩压(mmHg) 舒张压(mmHg) 平均动脉压(mmHg) 脉压差(mmHg) AS(n=26) 89±18* 198±11.2 106±18.1 136±11.9 89±16.1 AHF(n=22) 108±17 202±19.6 108±17.4 139±13.8 86±16.2 ACS(n=16) 90±16* 196±16.4 106±12.4 134±12.8 90±19.8 ACH(n=12) 92±21* 199±11 106±17.4 138±11.6 94±15.2 F 6.622 0.741 0.924 1.345 1.512 P < 0.001 0.445 0.700 0.423 0.565 *P < 0.05 vs AHF(LSD法多重两两比较). AS: 急性脑卒中; AHF: 急性心力衰竭; ACS: 急性冠脉综合征; ACH: 急性脑出血.
下载: 导出CSV
表 4 高血压急症多因素回归分析
Table 4. Multivariate regression analysis of hypertensive emergency
因变量 β SE Wald χ2 P OR 95%CI 糖尿病史 0.762 0.286 7.099 0.008 2.413 1.223~3.753 心率 0.567 0.234 15.798 0.002 2.346 1.789~5.542
下载: 导出CSV
-
[1] Cooper CM, Fenves AZ. Hypertensive urgencies and emergencies in the hospital setting[J]. Hosp Pract: 1995, 2016, 44(1): 21-7. http://www.onacademic.com/detail/journal_1000038465098610_f245.html [2] Lagi A, Cencetti S. Hypertensive emergencies: a new clinical approach[J]. Clin Hypertens, 2015, 21: 20. doi: 10.1186/s40885-015-0027-4 [3] Chinese Medical Doctor Association, Chinese College of Emergency Physicians; Chinese Hypertension League; Beijing Hypertension Association; . 中国急诊高血压诊疗专家共识(2017修订版)[J]. 中国实用内科杂志, 2018, 38(5): 421-33. https://www.cnki.com.cn/Article/CJFDTOTAL-SYNK201805012.htm [4] Dzau V, Braunwald E. Resolved and unresolved issues in the prevention and treatment of coronary artery disease: a workshop consensus statement[J]. Am Heart J, 1991, 121(4 pt 1): 1244-63. [5] Larsson SC, Drca N, Mason AM, et al. Resting heart rate and cardiovascular disease[J]. Circ: Genom Precis Med, 2019, 12(3): e002459. [6] Custodis F, Gertz K, Balkaya M, et al. Heart rate contributes to the vascular effects of chronic mental stress: effects on endothelial function and ischemic brain injury in mice[J]. Stroke, 2011, 42(6): 1742-9. doi: 10.1161/STROKEAHA.110.598607 [7] 王月波, 尹潞, 成小如, 等. 我国老年人心率与死亡风险的相关性研究[J]. 中华高血压杂志, 2020, 28(3): 300. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGGZ202003036.htm [8] Fox K, Ford I, Steg PG, et al. Heart rate as a prognostic risk factor in patients with coronary artery disease and left-ventricular systolic dysfunction (BEAUTIFUL): a subgroup analysis of a randomised controlled trial[J]. Lancet, 2008, 372(9641): 817-21. doi: 10.1016/S0140-6736(08)61171-X [9] Bouabdallaoui N, O'Meara E, Bernier V, et al. Beneficial effects of ivabradine in patients with heart failure, low ejection fraction, and heart rate above 77 b. p. m[J]. ESC Heart Fail, 2019, 6(6): 1199-207. doi: 10.1002/ehf2.12513 [10] Ritter MA, Rohde A, Heuschmann PU, et al. Heart rate monitoring on the stroke unit. What does heart beat tell about prognosis? An observational study[J]. BMC Neurol, 2011, 11(1): 1-8. doi: 10.1186/1471-2377-11-1 [11] Nolte CH, Erdur H, Grittner U, et al. Impact of heart rate on admission on mortality and morbidity in acute ischaemic stroke patients-results from VISTA[J]. Eur J Neurol, 2016, 23(12): 1750-6. doi: 10.1111/ene.13115 [12] James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8[) J]. JAMA, 2014, 311(5): 507-20. doi: 10.1001/jama.2013.284427 [13] 《中国高血压防治指南》修订委员会. 中国高血压防治指南2018年修订版[J]. 心脑血管病防治, 2019, 19(1): 1-44. doi: 10.3969/j.issn.1009-816X.2019.01.001 [14] Rao D, Balagopalan JP, Sharma A, et al. BEAT survey: a crosssectional study of resting heart rate in young (18-55 year) hypertensive patients[J]. J Assoc Physicians India, 2015, 63(5): 14-7. http://en.cnki.com.cn/Article_en/CJFDTOTAL-ZGGZ201510016.htm [15] Zhao MX, Zhao Q, Zheng M, et al. Effect of resting heart rate on the risk of all-cause death in Chinese patients with hypertension: analysis of the Kailuan follow-up study[J]. BMJ Open, 2020, 10(3): e032699. doi: 10.1136/bmjopen-2019-032699 [16] Okin PM, Kjeldsen SE, Julius S, et al. All-cause and cardiovascular mortality in relation to changing heart rate during treatment of hypertensive patients with electrocardiographic left ventricular hypertrophy[J]. Eur Heart J, 2010, 31(18): 2271-9. doi: 10.1093/eurheartj/ehq225 [17] Agewall S, Tjessem LH, Rossignol P, et al. Heart rate prediction of outcome in heart failure following myocardial infarction depend on heart rhythm status an analysis from the high-risk myocardial infarction database initiative[J]. Int J Cardiol, 2017, 249: 274-81. doi: 10.1016/j.ijcard.2017.09.182 [18] Kara D, Akinci SB, Babaoglu G, et al. Increased heart rate on first day in Intensive Care Unit is associated with increased mortality[J]. Pak J Med Sci, 2016, 32(6): 1402-7. http://www.onacademic.com/detail/journal_1000041657692999_cf5d.html [19] Hoke RS, Müller-Werdan U, Lautenschläger C, et al. Heart rate as an independent risk factor in patients with multiple organ dysfunction: a prospective, observational study[J]. Clin Res Cardiol, 2012, 101(2): 139-47. doi: 10.1007/s00392-011-0375-3 [20] Bruijns SR, Guly HR, Bouamra O, et al. Heart rate and systolic blood pressure in patients with minor to moderate, nonhaemorrhagic injury versus normal controls[J]. Emerg Med J, 2013, 30(11): 901-5. doi: 10.1136/emermed-2012-201760 [21] Tridetti J, Krzesinski F, D'orio V, et al. Increased heart rate as a risk factor and treatment target in patients with heart failure[J]. Rev Med Liege, 2017, 72(2): 81-6. http://www.ncbi.nlm.nih.gov/pubmed/28387085 [22] Sciatti E, Vizzardi E, Bonadei I, et al. The role of heart rate and ivabradine in acute heart failure[J]. Monaldi Arch Chest Dis, 2019, 89(3). DOI: 10.4081/monaldi.2019.1091. [23] AlHabib KF, Sulaiman K, Al Suwaidi J, et al. Patient and systemrelated delays of emergency medical services use in acute STelevation myocardial infarction: results from the third gulf registry of acute coronary events (gulf RACE-3Ps)[J]. PLoS One, 2016, 11 (1): e0147385. doi: 10.1371/journal.pone.0147385 [24] Jensen MT, Pereira M, Araujo C, et al. Heart rate at admission is a predictor of in-hospital mortality in patients with acute coronary syndromes: Results from 58 European hospitals: The European Hospital Benchmarking by Outcomes in acute coronary syndrome Processes study[J]. Eur Heart J Acute Cardiovasc Care, 2018, 7(2): 149-57. doi: 10.1177/2048872616672077 [25] Prasun MA, Albert NM. The importance of heart rate in heart failure and reduced ejection fraction[J]. J Cardiovasc Nurs, 2018, 33(5): 453-9. doi: 10.1097/JCN.0000000000000468 [26] Dalal J, Dasbiswas A, Sathyamurthy I, et al. Heart rate in hypertension: review and expert opinion[J]. Int J Hypertens, 2019, 2019: 2087064. http://www.onacademic.com/detail/journal_1000041641783499_375c.html [27] 施仲伟, 冯颖青, 王增武, 等. β受体阻滞剂在高血压应用中的专家共识[J]. 中华高血压杂志, 2019, 27(6): 516-24. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGGZ201906009.htm [28] Palatini P. Need for a revision of the normal limits of resting heart rate[J]. Hypertension, 1999, 33(2): 622-5. doi: 10.1161/01.HYP.33.2.622 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 647
- HTML全文浏览量: 144
- PDF下载量: 9
- 被引次数: 0