



Diagnostic value and serious evaluation of bedside accidents for community-acquired slip
-
摘要:
目的探讨床旁超声检查对于诊断社区获得性肺炎老年患者的诊断价值。 方法选取本院2019年8月~2020年6月收治的120例社区获得性肺炎老年患者作为感染组、60例健康志愿者作为对照组,两组分别接受床旁超声的检查,对比两组的肺部超声征象(A线征象、B线征象、肺实变征象)及肺部超声评分,并根据患者病情程度进行分层对比,采用ROC曲线分析肺部超声评分诊断肺部感染的价值。 结果感染组的A线征象、B线征象、肺实变征象检出率及肺部超声评分均高于对照组,差异具有统计学意义(P < 0.05). CPIS评分>6分的感染组患者的肺实变征象检出率及肺部超声评分均高于CPIS评分≤6分的患者,差异具有统计学意义(P < 0.05);CPIS评分>6分的感染组患者的A线征象、B线征象与CPIS评分≤6分的患者比较,差异无统计学意义(P> 0.05);死亡组患者的B线征象、肺实变征象检出率及肺部超声评分均高于存活患者,差异具有统计学意义(P < 0.05);肺部超声评分诊断肺部感染的敏感度为89.87%,特异性为83.36%,漏诊率为10.13%,误诊率为16.64%,ROC曲线下面积值为0.913。 结论床旁超声检查对于诊断社区获得性肺炎老年患者及病情判断均具有较高的临床价值。 Abstract:ObjectiveTo explore the clinical value of bedside ultrasound in diagnosing elderly patients with community-acquired pneumonia. MethodsA total of 120 elderly patients with community-acquired pneumonia admitted to Chongqing Dazu District People's Hospital from August 2019 to June 2020 were selected as the infection group and 60 healthy volunteers as the control group. The patients received bedside ultrasound examinations. The lung ultrasound signs (A-line signs, B-line signs, lung consolidation signs) and lung ultrasound scores, and stratified comparison according to the patient's condition between two groups were compared. ROC curve was used to analyze the value of pulmonary ultrasound score in the diagnosis of pulmonary infection. ResultsThe detection rate of A-line signs, B-line signs, lung consolidation signs and lung ultrasound scores of the infection group were significantly higher than those of the control group(P < 0.05). The detection rate of lung consolidation signs and lung ultrasound scores of patients in the infection group with a CPIS score >6 points were significantly higher than those of patients with a CPIS score ≤6 points(P < 0.05). The A-line signs and B-line signs of patients in the infection group with a CPIS score >6 were compared with those with a CPIS score of ≤6, (P>0.05). The detection rate of B-line signs, lung consolidation signs, and lung ultrasound scores of patients in the death group were significantly higher than those of the surviving patients (P < 0.05). The sensitivity of lung ultrasound scoring to diagnose lung infection was 89.87%, specificity was 83.36%, missed diagnosis rate was 10.13%, misdiagnosis rate was 16.64%, and the AUC value of the area under the ROC curve was 0.913. ConclusionBedside ultrasound examination has high clinical value for diagnosing elderly patients with community-acquired pneumonia and judging their condition. -
Key words:
- bedside ultrasound /
- diagnosis /
- community-acquired pneumonia /
- lung ultrasound
-
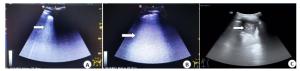
图 1 左下肺孤立B线(A)、右下肺重度B线(B)及左肺实变伴有胸腔积液(C)的影像学表现
Figure 1. Imaging of isolated left lower lung (A), severe right lower lung (B) and left lung solid transformation with pleural effusion (C).
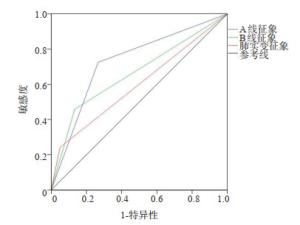
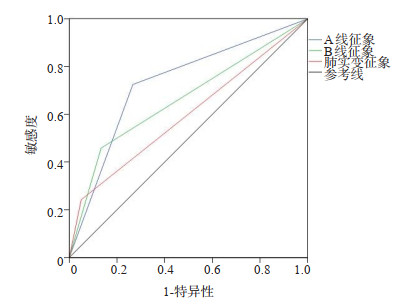
图 2 A线征象、B线征象、肺实变征象检出率诊断肺部感染的ROC曲线
Figure 2. ROC curve for the detection rate of A-line signs, B-line signs, and lung consolidation signs for the diagnosis of lung infection.
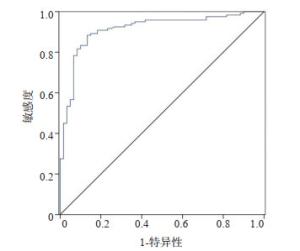
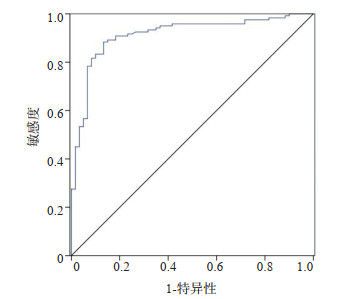
图 3 肺部超声评分诊断肺部感染的ROC曲线
Figure 3. ROC curve of lung ultrasound scoring for diagnosis of lung infection.
表 1 两组研究对象的一般资料比较
Table 1. Comparison of general data between the two groups[n(%)]
组别 感染组(n=120) 对照组(n=60) t/χ2 P 年龄(岁,Mean±SD) 75.3±8.4 73.8±7.0 1.19 0.23 身高(cm,Mean±SD) 166.5±6.2 164.8±5.5 1.79 0.07 体质量(kg,Mean±SD) 64.8±5.7 66.0±6.0 -1.30 0.19 性别 0.41 0.51 男 74(61.67) 34(56.67) 女 46(38.33) 26(43.33) 吸烟 1.45 0.22 是 47(39.17) 18(30.00) 否 73(60.83) 42(70.00) 饮酒 2.82 0.09 是 36(30.00) 11(18.33) 否 84(70.00) 49(81.67) 高血压 0.62 0.42 是 26(21.67) 10(16.67) 否 94(78.33) 50(83.33) 糖尿病 1.13 0.28 是 19(15.83) 6(10.00) 否 101(84.17) 54(90.00) 病原学 - - 非病毒性 72(60.00) - 病毒性 48(40.00) -  下载: 导出CSV
下载: 导出CSV
表 2 感染组和对照组的超声征象比较
Table 2. Comparison of ultrasound signs between infection group and control group[n(%)]
组别 A线征象 B线征象 肺实变征象 肺部超声评分(分, Mean±SD) 阳性 阴性 阳性 阴性 阳性 阴性 感染组(n=120) 87(72.5) 33(27.5) 55(45.83) 65(54.17) 29(24.17) 91(75.83) 16.5±3.9 对照组(n=60) 16(26.67) 44(73.33) 8(13.33) 52(86.67) 3(5.00) 57(95.00) 3.4±1.1 t/χ2 34.32 18.57 10.05 25.48 P < 0.01 < 0.01 0.01 < 0.01
下载: 导出CSV
表 3 不同感染病情患者超声征象比较
Table 3. Comparison of ultrasound signs in patients with different infectious diseases[n(%)]
CPIS评分 A线征象 B线征象 肺实变征象 肺部超声评分(分, Mean±SD) 阳性 阴性 阳性 阴性 阳性 阴性 ≤6分(n=77) 52(67.53) 25(32.47) 31(40.26) 46(59.74) 11(14.29) 66(85.71) 13.7±3.7 >6分(n=43) 35(81.40) 8(18.60) 24(55.81) 19(44.19) 18(41.86) 25(58.14) 21.5±3.8 t/χ2 2.66 2.68 11.44 -10.05 P 0.10 0.10 0.01 0.00 CPIS: 临床肺部感染评分.
下载: 导出CSV
表 4 不同预后结局患者超声征象比较
Table 4. Comparison of ultrasound signs in patients with different prognosis outcomes[n(%)]
预后结局 A线征象 B线征象 肺实变征象 肺部超声评分(分, Mean±SD) 阳性 阴性 阳性 阴性 阳性 阴性 存活(n=101) 71(70.3) 30(29.7) 42(41.58) 59(58.42) 19(18.81) 82(81.19) 14.8±3.7 死亡(n=19) 16(84.21) 3(15.79) 13(68.42) 6(31.58) 10(52.63) 9(47.37) 22.1±3.5 t/χ2 1.55 4.63 9.98 -7.95 P 0.21 0.03 0.00 0.00
下载: 导出CSV
表 5 肺部超声诊断肺部感染的价值
Table 5. The value of lung ultrasound in diagnosing pulmonary infection
指标 敏感度(%) 特异性(%) 漏诊率(%) 误诊率(%) AUC值 A线征象 72.50 73.33 27.50 26.67 0.729 B线征象 45.83 86.67 54.17 13.33 0.663 肺实变征象 24.17 95.00 75.83 5.00 0.596 肺部超声评分 89.87 83.36 10.13 16.64 0.913
下载: 导出CSV
-
[1] Garin N, Marti C, Scheffler M, et al. Computed tomography scan contribution to the diagnosis of community-acquired pneumonia[J]. Curr Opin Pulm Med, 2019, 25(3): 242-8. doi: 10.1097/MCP.0000000000000567 [2] 鲁佾, 肖贞良. 肺超声在诊断社区获得性肺炎中的应用[J]. 四川医学, 2018, 39(2): 216-8. https://www.cnki.com.cn/Article/CJFDTOTAL-SCYX201802031.htm [3] Del Rio-Pertuz G, Gutiérrez JF, Triana AJ, et al. Usefulness of sputum gram stain for etiologic diagnosis in community-acquired pneumonia: a systematic review and meta-analysis[J]. BMC Infect Dis, 2019, 19(1): 403. doi: 10.1186/s12879-019-4048-6 [4] Zhao X, Zhang M, Wang Y, et al. Diagnostic value of lung ultrasound for pregnant women with community-acquired pneumonia[J]. J Pak Med Assoc, 2020, 70[Special Issue](9): 57-63. http://www.researchgate.net/publication/347579441_Diagnostic_value_of_lung_ultrasound_for_pregnant_women_with_community-acquired_pneumonia [5] 李晓燕, 薄建萍. 社区获得性肺炎诊疗新进展[J]. 国际呼吸杂志, 2020, 40(6): 470-6. doi: 10.3760/cma.j.cn131368-20191018-01433 [6] 瞿介明, 曹彬. 中国成人社区获得性肺炎诊断和治疗指南(2016年版) 修订要点[J]. 中华结核和呼吸杂志, 2016, 39(4): 241-2. doi: 10.3760/cma.j.issn.1001-0939.2016.04.001 [7] 李永宁, 任延波, 康健, 等. 老年社区获得性肺炎合并新型冠状病毒肺炎患者的诊疗与思考: 附1例分析[J]. 中华危重病急救医学, 2020, 32 (10): 1178-82. doi: 10.3760/cma.j.cn121430-20200804-00623 [8] Caiulo VA, Gargani L, Caiulo S, et al. The role of ultrasound in community-acquired pneumonia[J]. Pediatr Pulmonol, 2013, 48 (10): 1043-4. doi: 10.1002/ppul.22787 [9] Caiulo VA, Gargani L, Caiulo S, et al. Lung ultrasound characteristics of community-acquired pneumonia in hospitalized children[J]. Pediatr Pulmonol, 2013, 48(3): 280-7. doi: 10.1002/ppul.22585 [10] Jolobe OMP. Pulmonary tuberculosis in the differential diagnosis of community-acquired pneumonia[J]. Eur Respir J, 2012, 40(1): 279. doi: 10.1183/09031936.00004312 [11] 殷勇, 陆权. 充分认识临床综合评估对儿童社区获得性肺炎诊断的重要性[J]. 中华实用儿科临床杂志, 2020, 35(16): 1201-5. doi: 10.3760/cma.j.cn101070-20200506-00773 [12] 张超凡, 程英春, 董海, 等. 重症患者床旁超声显示双肺不对称征象的临床意义[J]. 中华危重病急救医学, 2020, 32(9): 1118-20. doi: 10.3760/cma.j.cn121430-20200108-00117 [13] 牛慧敏, 高洁, 于明月, 等. 肺超声对小儿社区获得性肺炎的诊断可靠性分析[J]. 临床肺科杂志, 2019, 24(7): 1180-4. doi: 10.3969/j.issn.1009-6663.2019.07.005 [14] Reissig A, Copetti R, Mathis G, et al. Lung ultrasound in the diagnosis and follow-up of community-acquired pneumonia[J]. Chest, 2012, 142(4): 965-72. doi: 10.1378/chest.12-0364 [15] D'Amato M, Rea G, Carnevale V, et al. Assessment of thoracic ultrasound in complementary diagnosis and in follow up of community-acquired pneumonia (cap)[J]. BMC Med Imaging, 2017, 17(1): 52. doi: 10.1186/s12880-017-0225-5 [16] Stadler JAM, Andronikou S, Zar HJ. Lung ultrasound for the diagnosis of community-acquired pneumonia in children[J]. Pediatr Radiol, 2017, 47(11): 1412-9. doi: 10.1007/s00247-017-3910-1 [17] Bourcier JE, Braga S, Garnier D. Lung ultrasound will soon replace chest radiography in the diagnosis of acute community-acquired pneumonia[J]. Curr Infect Dis Rep, 2016, 18(12): 43. doi: 10.1007/s11908-016-0550-9 [18] 范蕾, 薛克栋. 老年社区获得性肺炎诊治1例报告[J]. 中国实用内科杂志, 2019, 39(5): 485-6. https://www.cnki.com.cn/Article/CJFDTOTAL-SYNK201905024.htm [19] Buda N, Hajduk A, Jaworska J, et al. Lung ultrasonography as an accurate diagnostic method for the diagnosis of community-acquired pneumonia in the elderly population[J]. Ultrasound Q, 2020, 36(2): 111-7. doi: 10.1097/RUQ.0000000000000499 [20] Lutfiyya MN, Henley E, Chang LF, et al. Diagnosis and treatment of community-acquired pneumonia[J]. Am Fam Physician, 2006, 73 (3): 442-50. -

 点击查看大图
点击查看大图

计量
- 文章访问数: 369
- HTML全文浏览量: 164
- PDF下载量: 5
- 被引次数: 0