



Correlation of Ki-67 expression with MSCT signs and risk grading in small intestinal stromal tumors
-
摘要:
目的探讨小肠间质瘤(SIST)组织中的Ki-67表达与多层螺旋CT(MSCT)表现、危险分级的相关性。 方法回顾性分析87例经手术病理证实的SIST的临床病理、免疫组化及影像学资料,探讨SIST组织中Ki-67表达与CT表现、危险分级的关系。 结果在单因素方差分析中,Ki-67表达在部位、形态、大小、浸润转移、病理分组及核分裂像方面差异具有统计学意义(P < 0.05);性别、年龄、临床特征、囊变或坏死、溃疡、生长方式、是否为肠系膜上动脉供血、动脉期强化程度、静脉期或延迟期强化方式均无统计学意义(P > 0.05)。多因素Logistic回归分析显示Ki-67表达5%~10%为亚组时,大小差异具有统计学意义(P < 0.05),以 < 2 cm为对照,其中2~5 cm分组OR值为2.179,5~10 cm分组OR值为4.345, > 10 cm分组OR值为7.698。 > 10%亚组,其中回肠与大小是影响高表达的独立影响因素(P < 0.05),回肠OR值为17.622;以 < 2 cm为对照,其中2~5 cm分组OR值为2.179,5~10 cm分组OR值为4.345, > 10 cm分组OR值为7.698。 结论SIST组织中的Ki-67表达与MSCT征象有一定的相关性,并且高危组、核分裂数较大的组织Ki-67表达更高,对SIST的临床治疗方案选择、预后判断具有一定的辅导意义。 Abstract:ObjectiveTo investigate the correlation of Ki-67 expression with MSCT findings and risk grade in small intestinal stromal tumor (SIST). MethodsThe clinicopathological, immunohistochemical and imaging data of 87 cases of SIST confirmed by surgery and pathology were retrospectively analyzed to explore the relationship between Ki-67 expression and CT findings and risk classification. ResultsIn one-way ANOVA, Ki-67 expression was significantly different in location, shape, size, invasion and metastasis, pathological group and mitotic image (P < 0.05); There was no significant difference in gender, age, clinical features, cystic degeneration or necrosis, ulcer, growth pattern, whether it was supplied by superior mesenteric artery, enhancement degree in arterial phase, enhancement mode in venous phase or delayed phase (P > 0.05). The Results of multivariate logistic regression analysis showed that the expression of Ki-67 was 5% to 10% in subgroups, the size was statistically significant (P < 0.05), and the control was less than 2 cm, of which the or value of 2-5 cm group was 2.179, or value of 5-10 cm group was 4.345, or value of greater than 10 cm group was 7.698. The or value of ileum was 17.622 in greater than 10% subgroup (P < 0.05), the or value of 2-5 cm subgroup was 2.179, 5-10 cm subgroup was 4.345, and greater than 10 cm subgroup was 7.698. ConclusionThe expression of Ki-67 in SIS is correlated with MSCT signs, and the expression of Ki-67 is higher in high-risk group and tissues with larger mitosis number, which has certain guiding significance for the selection of clinical treatment and prognosis of SIST. -
Key words:
- small intestine /
- stromal tumor /
- Ki-67 index /
- pathological risk classification /
- multi slice spiral CT
-
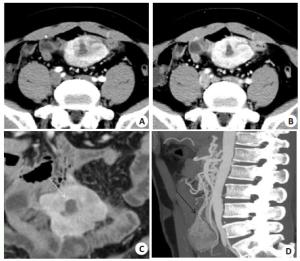
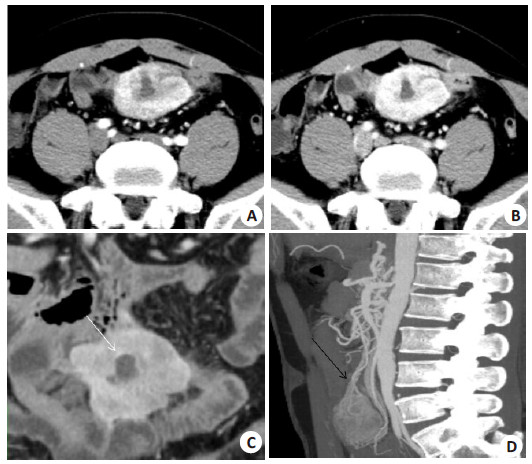
图 1 回肠间质瘤(低危险度)影像学表现
男,42岁,腹痛.A:动脉期显示病灶不均匀强化;B:静脉期渐进性强化;C:病灶呈分叶状,其内可见囊变区(白箭);D:矢状位可见肠系膜上动脉供血(黑箭).
Figure 1. Imaging of a 42 year old man with abdominal pain and ileal stromal tumor(low risk).
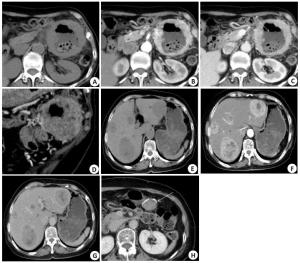
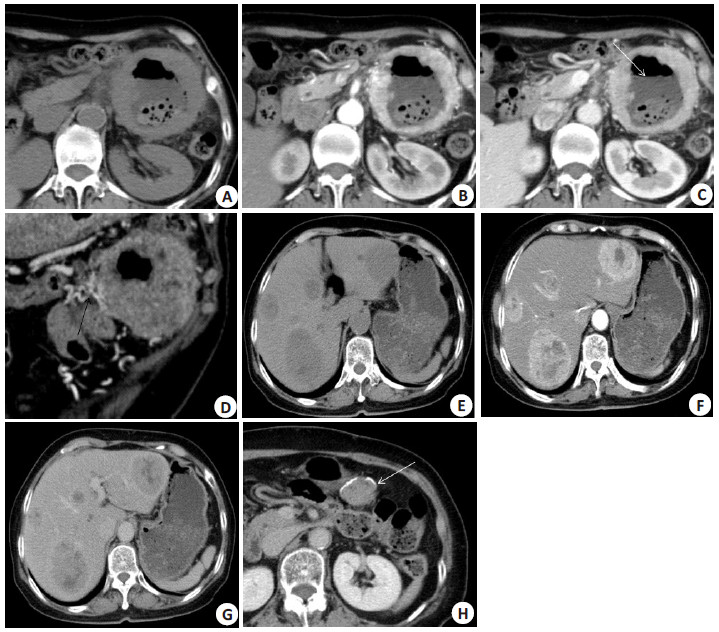
图 2 空肠间质瘤(高危险度)影像学表现
患者女,71岁,黑便。A~D:病灶内可见积气、坏死及液平(白箭),增强扫描病灶边缘呈明显强化,肿瘤周边见较多供血动脉(黑箭);E~H:患者术后4年复查,肝脏多发转移灶,术区未见肿瘤复发(白箭).
Figure 2. Imaging of jejunal stromal tumor (high risk).
表 1 Ki-67表达与患者MSCT征象的关系
Table 1. Relationship between Ki-67 expression and MSCT features[n(%)]
MSCT征象 Ki-67表达 χ2/F P 5%(n=36) 5%~10%(n=27) > 10(n=24) 部位 12.60 0.01 回肠 9(25.0) 4(14.8) 12(50.0) 空肠 20(55.6) 12(44.4) 10(41.7) 十二指肠 7(19.4) 11(40.7) 2(8.3) 形态 8.10 0.01 分叶状或不规则 16(44.4) 20(74.1) 18(75.0) 圆形或椭圆形 20(55.6) 7(25.9) 6(25.0) 大小(cm,Mean±SD) 5.71±4.79 8.13±5.74 10.20±6.19 4.91 0.01 囊变或坏死 2.87 0.23 有 16(44.4) 14(51.9) 16(66.7) 无 36(55.6) 27(48.1) 24(33.3) 溃疡 0.29 0.86 有 3(8.3) 3(11.1) 3(12.5) 无 33(91.7) 24(88.9) 21(87.5) 生长方式 7.82 0.09 腔内外型 12(33.3) 16(59.3) 15(62.5) 腔内型 10(27.8) 3(11.1) 2(8.3) 腔外型 14(38.9) 8(29.6) 7(29.2) 肠系膜上动脉分支供血 7.82 0.09 有 18(50.0) 17(63.0) 15(62.5) 无 18(50.0) 10(37.0) 9(37.5) 浸润或转移 7.63 0.02 有 6(16.7) 8(29.6) 12(50.0) 无 30(83.3) 19(70.4) 12(50.0) 动脉期强化程度(Hu) 2.01 0.73 < 20 6(16.7) 2(7.4) 5(20.8) 20~40 10(27.8) 9(33.3) 7(29.2) > 40 20(55.6) 16(59.3) 12(50.0) 静脉期及延迟期强化方式 2.31 0.31 减退 15(41.7) 16(59.3) 10(41.7) 渐进性强化 21(58.3) 11(40.7) 14(58.3)  下载: 导出CSV
下载: 导出CSV
表 2 Ki-67表达与临床及病理特征的关系
Table 2. Relationship between Ki-67 expression and clinical and pathological features[n(%)]
临床病理特征 Ki-67表达 χ2 P < 5%(n=36) 5%~10%(n=27) > 10%(n=24) 性别 4.95 0.08 男 21(58.3) 10(37.0) 16(66.7) 女 15(41.7) 17(63.0) 8(33.3) 年龄(岁,Mean±SD) 55.50±13.67 53.11±10.78 59.13±13.23 1.43 0.24 临床特征 3.04 0.56 消化道出血 21(58.3) 19(70.4) 13(54.2) 腹痛腹部不适 10(27.8) 7(25.9) 9(37.5) 无症状 5(13.9) 1(13.9) 2(8.3) 病理分组 21.20 < 0.01 高危组 10(27.8) 19(70.4) 20(83.3) 低危组 26(72.2) 8(29.6) 4(16.7) 核分裂像(个) 16.33 0.03 < 5 33(91.7) 17(63.0) 22(50.0) 5~10 2(5.6) 7(25.9) 5(20.8) > 10 1(2.8) 3(11.1) 7(29.2)
下载: 导出CSV
表 3 Ki-67表达影响因素的多元logistic回归
Table 3. Multiple logistic regression analysis on the influencing factors of Ki-67 expression
变量 β 标准误 Wald df P OR 95%CI 5%~10% 部位 回肠 1.043 1.097 0.903 1 0.342 2.836 0.330~24.351 空肠 0.716 0.751 0.909 1 0.340 2.047 0.470~8.922 十二指肠 对照 形态 分叶状或不规则 -0.081 0.857 0.009 1 0.924 0.922 0.172~4.945 圆形或椭圆形 对照 大小(cm) < 2 对照 2~5 0.779 0.713 8.129 0.034 2.179 0.539~8.811 5~10 1.469 0.892 8.752 < 0.001 4.345 0.757~24.953 > 10 2.041 0.901 10.991 < 0.001 7.698 1.317~45.015 浸润或转移 是 -0.030 0.909 0.001 1 0.974 0.970 0.163~5.760 否 对照 病理分组 高危组 -1.103 1.509 0.534 1 0.465 0.332 0.017~6.394 低危组 对照 核分裂像(个) < 5 1.816 1.286 1.993 1 0.158 6.148 0.494~76.511 5~10 0.393 1.533 0.066 1 0.798 1.482 0.073~29.916 > 10 对照 > 10% 部位 十二指肠 对照 回肠 2.869 1.052 7.439 1 0.006 17.622 2.242~138.509 空肠 1.373 .806 2.903 1 0.088 3.949 0.813~19.171 形态 圆形或椭圆形 对照 分叶状或不规则 -0.771 0.916 0.709 1 0.400 0.462 0.077~2.784 大小(cm) < 2 对照 2~5 0.779 0.713 8.129 0.034 2.179 0.539~8.811 5~10 1.469 0.892 8.752 < 0.001 4.345 0.757~24.953 > 10 2.041 0.901 10.991 < 0.001 7.698 1.317~45.015 浸润或转移 否 对照 是 1.226 0.875 1.963 1 0.161 3.409 0.613~18.959 病理分组 低危组 对照 高危组 0.833 1.655 0.253 1 0.615 2.300 0.090~58.913 核分裂像(个) > 10 对照 < 5 0.983 1.018 0.932 1 0.334 2.672 0.363~19.649 5~10 0.960 1.164 0.681 1 0.409 2.613 0.267~25.584
下载: 导出CSV
-
[1] Cameron S, Beham A, Schildhaus HU. Current standard and future perspectives in the treatment of gastrointestinal stromal tumors[J]. Digestion, 2017, 95(4): 262-8. doi: 10.1159/000455835 [2] 章锦伟, 刘啸峰, 钱彬, 等. 小肠间质瘤多层螺旋CT表现与恶性程度相关性分析[J]. 中华肿瘤防治杂志, 2019, 26(23): 1795-9. https://www.cnki.com.cn/Article/CJFDTOTAL-QLZL201923010.htm [3] Booth DG, Takagi M, Sanchez-Pulido L, et al. Ki-67 is a PP1-interacting protein that organises the mitotic chromosome periphery[J]. Elife, 2014, 3: e01641. doi: 10.7554/eLife.01641 [4] Turkel Kucukmetin N, Cicek B, Saruc M, et al. Ki67 as a prognostic factor for long-term outcome following surgery in gastrointestinal stromal tumors[J]. Eur J Gastroenterol Hepatol, 2015, 27(11): 1276-80. doi: 10.1097/MEG.0000000000000454 [5] 张丽静, 陈德强, 张春谦, 等. 基于CT图像的放射组学特征联合CT征象的GIST危险度分级的列线图模型的初步研究[J]. 临床放射学杂志, 2020, 39(9): 1790-5. [6] 汪明, 曹晖. 从2020年国内外主要指南更新变化解读胃肠间质瘤精准诊治[J]. 中国实用外科杂志, 2021, 41(2): 125-9. [7] Mazur MT, Clark HB. Gastric stromal tumors Reappraisal of histogenesis[J]. Am J Surg Pathol, 1983, 7(6): 507-20. doi: 10.1097/00000478-198309000-00001 [8] 雷志毅, 祁明珠, 孟巴音. 27例小肠间质瘤原发及复发转移的CT征象分析[J]. 医学影像学杂志, 2017, 27(7): 1303-6. https://www.cnki.com.cn/Article/CJFDTOTAL-XYXZ201707028.htm [9] 陈世雄, 周莉, 黄吉成, 等. MSCT在胃间质瘤患者鉴别诊断中的应用[J]. 中国CT和MRI杂志, 2020, 18(11): 134-6. https://www.cnki.com.cn/Article/CJFDTOTAL-CTMR202011043.htm [10] 宋学林, 杨世锋, 顾慧, 等. 对比胃与小肠间质瘤多层螺旋CT征象及病理学特点[J]. 中国医学影像技术, 2021, 37(1): 76-80. [11] Nakamura N, Yamamoto H, Yao T, et al. Prognostic significance of expressions of cell-cycle regulatory proteins in gastrointestinal stromal tumor and the relevance of the risk grade[J]. Hum Pathol, 2005, 36(7): 828-37. doi: 10.1016/j.humpath.2005.03.012 [12] Tang J, Gui C, Qiu S, et al. The clinicopathological significance of Ki67 in papillary thyroid carcinoma: a suitable indicator? [J]. World J Surg Oncol, 2018, 16(1): 100. doi: 10.1186/s12957-018-1384-8 [13] 任爱雄, 卫美辰, 杨玉庆, 等. 血清KI-67抗原(ki67)水平检测及用于浸润性乳腺癌临床诊断的评价[J]. 细胞与分子免疫学杂志, 2020, 36 (12): 1124-8. [14] 韩帅, 孟帆, 张宏凯, 等. Ki-67、Ck19与肝细胞癌临床病理特征和磁共振成像表观扩散系数的相关性分析[J]. 中华医学杂志, 2021, 101 (11): 798-802. doi: 10.3760/cma.j.cn112137-20210108-00058 [15] 何海栋, 柴秀娟, 徐卫华, 等. PD-L1、Ki67与非小细胞肺癌患者临床病理特征及预后的关系[J]. 中国现代医学杂志, 2020, 30(16): 39-44. https://www.cnki.com.cn/Article/CJFDTOTAL-ZXDY202016008.htm [16] 唐军梅, 张启芳, 陈勇昌, 等. 胃癌患者Hp感染及与Ki67表达的相关性研究[J]. 中国中西医结合消化杂志, 2020, 28(11): 855-8. doi: 10.3969/j.issn.1671-038X.2020.11.07 [17] Liang YM, Li XH, Li WM, et al. Prognostic significance of PTEN, Ki-67 and CD44s expression patterns in gastrointestinal stromal tumors[J]. World J Gastroenterol, 2012, 18(14): 1664-71. http://labs.europepmc.org/articles/pmc3325534 [18] 张秋杰. 胃癌组织中CDX2表达及其与KI67的关系分析[J]. 实用癌症杂志, 2016, 31(7): 1062-4. https://www.cnki.com.cn/Article/CJFDTOTAL-SYAZ201607006.htm [19] 桑蝶, 王佳玉, 徐兵河. 增殖细胞核抗原Ki67与乳腺癌新辅助化疗疗效的关系[J]. 中华乳腺病杂志: 电子版, 2015, 9(1): 50-3. https://www.cnki.com.cn/Article/CJFDTOTAL-ZHRD201501013.htm [20] 金一, 姜大庆, 马特, 等. 新辅助内分泌治疗后腋窝转移淋巴结中Ki-67蛋白表达对绝经后乳腺癌预后的影响[J]. 肿瘤学杂志, 2016, 21(12): 1042-7. https://www.cnki.com.cn/Article/CJFDTOTAL-XHON201612012.htm [21] Joensuu H. Risk stratification of patients diagnosed with gastrointestinal stromal tumor[J]. Hum Pathol, 2008, 39(10): 1411-9. http://europepmc.org/abstract/MED/18774375 [22] 年中国胃肠道间质瘤病理诊断共识专家组. 中国胃肠道间质瘤病理诊断共识(2013年版)解读[J]. 中华病理学杂志, 2015, 44(1): 3-8. [23] 吴炼, 陈道荣. 胃间质瘤组织中Ki-67表达与危险度分级的关系[J]. 山东医药, 2018, 58(41): 51-4. https://www.cnki.com.cn/Article/CJFDTOTAL-SDYY201841014.htm [24] 孟美玲, 房良, 刁泽园, 等. 胃肠道间质瘤CT表现与Ki-67指数及危险分层相关性[J]. 青岛大学学报: 医学版, 2020, 56(1): 17-21. https://www.cnki.com.cn/Article/CJFDTOTAL-BATE202001006.htm [25] 方海英, 祝跃明, 黄小燕. 29例胃肠道间质瘤CT诊断及血供分析[J]. 肿瘤学杂志, 2010, 16(11): 902-4. https://www.cnki.com.cn/Article/CJFDTOTAL-XHON201011024.htm [26] 陈媛慧, 张进华, 胡道予, 等. 胃底间质瘤增强MSCT影像特征分析[J]. 放射学实践, 2020, 35(11): 1458-63. https://www.cnki.com.cn/Article/CJFDTOTAL-FSXS202011027.htm [27] DeMatteo RP, Lewis JJ, Leung D, et al. Two hundred gastrointestinal stromal tumors: recurrence patterns and prognostic factors for survival [J]. Ann Surg, 2000, 231(1): 51-8. http://www.tandfonline.com/servlet/linkout?suffix=CIT0004&dbid=8&doi=10.1586%2Fera.12.86&key=10636102 [28] 庞典付, 龚腊梅, 张克难. 胃肠道间质瘤48例临床分析[J]. 中国普通外科杂志, 2010, 19(10): 1159-61. https://www.cnki.com.cn/Article/CJFDTOTAL-ZPWZ201010036.htm -

 点击查看大图
点击查看大图
计量
- 文章访问数: 429
- HTML全文浏览量: 201
- PDF下载量: 3
- 被引次数: 0