



Value of dual-phase bronchial artery 64-slice CT in the diagnosis of benign and malignant pulmonary nodules
-
摘要:
目的分析64排CT支气管动脉双期扫描技术对肺结节的良、恶性诊断价值。 方法选取2016年9月~2020年9月我院行64排螺旋CT常规扫描发现肺结节(直径在3 cm以下)患者120例,均行支气管动脉双期增强扫描及病变靶扫描,经病理证实为肺恶性结节65例(记为恶性组)、浸润前病变结节(原位癌)30例(记为浸润前病变组)、肺良性结节25例(记为良性组),比较3组CT征象检出率,对比3组支气管动脉形态、图像质量、平扫与增强扫描CT值、双时相增强扫描后强化程度,分析支气管动脉双期增强扫描对肺恶性结节的诊断价值。 结果恶性组深分叶征、毛刺征、棘状突起、血管纠集征、空泡征、胸膜凹陷征占比较高,肺磨玻璃影中血管与支气管分型以Ⅱ、Ⅲ型为主,浸润前病变组钙化、卫星灶占比较高,肺磨玻璃影中血管与支气管分型以Ⅳ型为主,良性组方形征占比较高,肺磨玻璃影中血管与支气管分型以Ⅰ、Ⅱ型为主,差异均有统计学意义(P < 0.05);恶性组支气管动脉形态为血管湖比例高于浸润前病变组、良性组(P < 0.05),3组成团、迂曲、中断比例比较差异无统计学意义(P>0.05);3组图像质量比较差异无统计学意义(P>0.05);3组平扫CT值比较差异无统计学意义(P>0.05),恶性组、良性组增强扫描30~45 s、90~ 120 s的CT值均高于浸润前病变组(P < 0.05),恶性组增强扫描90~120 s的CT值低于良性组(P < 0.05);3组双期增强扫描后强化程度差异有统计学意义(P < 0.05),其中恶性组以中度、明显强化为主,且呈快升快降模式;64排CT支气管动脉双期增强扫描诊断肺结节恶性的敏感度、特异性、准确度分别为84.61%、76.36%、80.83%。 结论64排CT支气管动脉双期扫描对肺结节良恶性有一定诊断价值,依据其CT征象、肺磨玻璃影中血管与支气管分型及支气管形态、强化程度等可作出准确诊断。 Abstract:ObjectiveTo analyze the diagnostic value of dual-phase bronchial artery 64-slice CT for pulmonary nodules. MethodsA total of 120 patients with pulmonary nodules (under 3 cm in diameter) found by 64-slice spiral CT in our hospital between September 2016 and September 2020 were enrolled in the study. All of them were subjected to bronchial artery dualphase enhanced scan and targeted scan of the lesion. Pathology confirmed that there were 65 cases with malignant pulmonary nodules (malignant group), 30 cases with preinvasive nodules (carcinoma in situ) (preinvasive group), and 25 cases with benign pulmonary nodules (benign group). The detection rates of CT signs, bronchial artery morphology, image quality, CT values of plain scan and enhanced scan, and enhancement after dual-phase enhanced scan were compared between the two groups. The diagnostic value of bronchial artery dual-phase enhanced scan for malignant pulmonary nodules was analyzed. ResultsIn the malignant group, the proportions of deep lobulation sign, spicule sign, spiculate protuberance, blood vessel pack sign, vacuole sign, and pleural indentation sign were higher, the blood vessels and bronchi in pulmonary ground glass shadow mainly were type Ⅱ and Ⅲ. In the preinvasive group, the proportions of calcification and satellite lesions were higher, the blood vessels and bronchi in pulmonary ground glass shadow mainly were type Ⅳ. In the benign group, the proportion of square signs was higher, the blood vessels and bronchi in the pulmonary ground glass shadow mainly were type Ⅰ and Ⅱ (P < 0.05). The proportion of vascular lake was higher in the malignant group than in the preinvasive group and the benign group (P < 0.05). There were no statistically significant differences in the proportions of aggregation, tortuosity and interruption, image quality and CT value of plain scan among the 3 groups (P>0.05). The CT values of enhance scan at 30-45 s and 90-120 were higher in the malignant group and the benign group than in the preinvasive group (P < 0.05), and CT values of enhanced scan at 90~120 s were lower in the malignant group than in the benign group (P < 0.05). Statistically significant differences were found in enhancement after dual-phase enhanced scan among the 3 groups (P < 0.05). Besides, moderate and obvious enhancement was the majority in the malignant group, showing a fast-rising and fast-falling pattern. The sensitivity, specificity and accuracy of bronchial artery dual-phase 64-slice CT for diagnosing the malignancy of pulmonary nodules were 84.61%, 76.36%, and 80.83%, respectively. ConclusionThe bronchial artery dual-phase 64-slice CT has certain value in the diagnosis of benign and malignant pulmonary nodules. Accurate diagnosis can be made based on the CT signs, vascular and bronchial types in pulmonary ground glass shadow, bronchial morphology, and the degree of enhancement. -
Key words:
- 64-slice CT /
- bronchial artery /
- dual-phase scan /
- pulmonary nodules /
- benign and malignant /
- diagnostic value
-
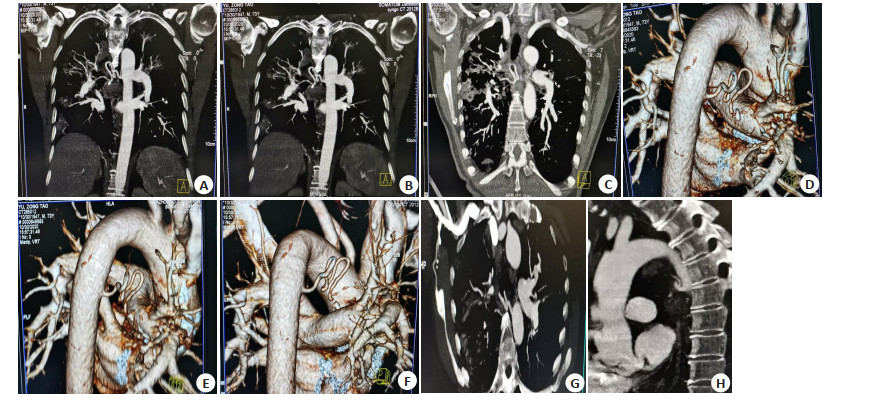
图 1 典型病例
患者男, 73岁, 咯血入院治疗, 病理证实为肺腺癌, 结节恶性.A~B: 右侧支气管动脉所示; C: 左侧支气管动脉所示, 可见深分叶、棘状突起, 增强扫描时支气管动脉期中度强化, 平衡期对比剂仍维持较高水平; D~F: 彩色支气管所示, 增强扫描时支气管动脉期中度强化, 平衡期对比剂仍维持较高水平, G~H: 靶扫描所示,可见卫星灶、钙化.
Figure 1. Typical cases
表 1 CT征象比较
Table 1. Comparison of CT signs among the three groups [n(%)]
组别 恶性组(n=65) 浸润前病变组(n=30) 良性组(n=25) χ2/Z P 深分叶征 61(93.85) 2(6.67)* 5(20.00)* 80.826 < 0.001 毛刺征 63(96.92) 6(20.00)* 9(36.00)* 65.064 < 0.001 棘状突起 54(83.08) 5(16.67)* 8(32.00)* 43.985 < 0.001 血管纠集征 51(78.46) 3(10.00)* 3(12.00)* 54.542 < 0.001 空泡征 26(40.00) 2(6.67)* 0(0)* 22.363 < 0.001 胸膜凹陷征 42(64.62) 2(6.67)* 1(4.00)* 44.532 < 0.001 钙化 3(4.62) 17(56.67)* 0(0)*# 46.367 < 0.001 空洞 9(13.85) 5(16.67) 3(12.00) 0.264 0.88 卫星灶 3(4.62) 20(66.67)* 5(20.00)*# 44.385 < 0.001 方形征 0(0) 3(10.00)* 11(44.00)*# 34.035 < 0.001 肺磨玻璃影中血管分型 42.914 < 0.001 Ⅰ型 0(0) 0(0) 4(16.00) Ⅱ型 40(61.54) 2(6.67) 18(72.00) Ⅲ型 21(32.31) 21(7.000) 3(12.00) Ⅳ型 4(6.15) 7(23.33) 0(0) 肺磨玻璃影中支气管分型 60.641 < 0.001 Ⅰ型 0(0) 1(3.33) 5(20.00) Ⅱ型 18(27.69) 0(0) 16(64.00) Ⅲ型 43(66.15) 6(20.00) 4(16.00) Ⅳ型 2(3.08) 23(76.67) 0(0) Ⅴ型 2(3.08) 0(0) 0(0) *P < 0.05 vs恶性组; #P < 0.05 vs浸润前病变组.  下载: 导出CSV
下载: 导出CSV
表 2 支气管形态比较
Table 2. Comparison of bronchial morphology among the three groups [n(%)]
组别 血管湖 成团 迂曲 中断 恶性组(n=65) 18(27.69) 9(13.85) 38(58.46) 5(7.69) 浸润前病变组(n=30) 1(3.33)* 2(6.67) 22(73.33) 6(20.00) 良性组(n=25) 0(0)* 1(4.00) 20(80.00) 4(16.00) χ2 15.087 2.445 4.574 3.207 P < 0.001 0.295 0.102 0.202 *P < 0.05 vs恶性组.
下载: 导出CSV
表 3 图像质量比较
Table 3. Comparison of image quality among the three groups [n(%)]
组别 优 良 中 差 恶性组(n=65) 43(66.15) 18(27.69) 4(6.15) 0(0) 浸润前病变组(n=30) 25(83.33) 3(10.00) 2(6.67) 0(0) 良性组(n=25) 19(76.00) 4(16.00) 2(8.00) 0(0) χ2 2.667 P 0.264
下载: 导出CSV
表 4 增强扫描前后CT值比较
Table 4. Comparison of CT values among the three groups before and after enhanced scan (Hu, Mean±SD)
组别 平扫CT值 增强扫描30~45 s 增强扫描90~120 s 恶性组(n=65) 34.06±3.85 54.18±5.57 58.67±5.93 浸润前病变组(n=30) 34.56±3.52 41.56±4.29* 40.16±4.27* 良性组(n=25) 32.59±3.45 53.78±5.46# 71.06±7.28*# F 2.114 63.721 196.584 P 0.115 < 0.001 < 0.001 *P < 0.05 vs恶性组; #P < 0.05 vs浸润前病变组.
下载: 导出CSV
表 5 双期增强扫描后强化程度比较
Table 5. Comparison of the enhancement degree among the three groups after dual-phase enhanced scan [n(%)]
组别 无强化 轻度强化 中度强化 明显强化 环形强化 恶性组(n=65) 1(1.54) 6(9.23) 40(61.54) 16(24.62) 2(3.08) 浸润前病变组(n=30) 11(36.67) 12(40.00) 2(6.67) 0(0) 5(16.67) 良性组(n=25) 0(0) 1(4.00) 13(52.00) 11(44.00) 0(0) χ2 77.664 P < 0.001
下载: 导出CSV
-
[1] Wong MCS, Lao XQ, Ho KF, et al. Incidence and mortality of lung cancer: global trends and association with socioeconomic status[J]. Sci Rep, 2017, 7(1): 14300. doi: 10.1038/s41598-017-14513-7 [2] Siegel RL, Miller KD, JemalA. Cancer statistics, 2017[J]. CA Cancer J Clin, 2017, 67(1): 7-30. doi: 10.3322/caac.21387 [3] Cruickshank A, Stieler G, Ameer F. Evaluation of the solitary pulmonary nodule[J]. Intern Med J, 2019, 49(3): 306-15. doi: 10.1111/imj.14219 [4] 任占丽, 贺太平, 杨创勃, 等. 磁共振3D-VIBE序列和STAR-VIBE序列对肺结节显示能力的比较研究[J]. 磁共振成像, 2019, 10(1): 14-7. https://www.cnki.com.cn/Article/CJFDTOTAL-CGZC201901006.htm [5] Divisi D, Barone M, Bertolaccini L, et al. Standardized uptake value and radiological density attenuation as predictive and prognostic factors in patients with solitary pulmonary nodules: our experience on 1, 592 patients[J]. J Thorac Dis, 2017, 9(8): 2551-9. doi: 10.21037/jtd.2017.06.124 [6] Wang XM, Lv L, Zheng QY, et al. Differential diagnostic value of 64- slice spiral computed tomography in solitary pulmonary nodule[J]. Exp Ther Med, 2018, 15(6): 4703-8. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC5958795/ [7] 王万勤, 刘斌, 周勇, 等. 良恶性肺结节多排CT征象分析[J]. 安徽医药, 2018, 22(8): 1491-6. doi: 10.3969/j.issn.1009-6469.2018.08.017 [8] Travis WD, Brambilla E, Noguchi M, et al. International association for the study of lung cancer/American thoracic society/European respiratory society international multidisciplinary classification of lung adenocarcinoma[J]. J Thorac Oncol, 2011, 6(2): 244-85. doi: 10.1097/JTO.0b013e318206a221 [9] 李凤, 沈晶, 薛昌辉, 等. 肺磨玻璃结节与邻近血管及支气管的关系与分型对其良恶性鉴别诊断的价值[J]. 大连医科大学学报, 2017, 39 (5): 446-51. https://www.cnki.com.cn/Article/CJFDTOTAL-DLYK201705007.htm [10] 周丹静, 许建铭, 姜彦, 等. 迭代模型重建技术在低剂量胸部CT双期增强扫描中的可行性[J]. 中国医学影像技术, 2017, 33(5): 768-72. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYXX201705043.htm [11] 谢万明, 黄升云, 肖哲, 等. Q. STATIC呼吸门控与非门控扫描肺结节的临床价值: 65例前瞻性研究[J]. 分子影像学杂志, 2020, 43(4): 639-42. doi: 10.12122/j.issn.1674-4500.2020.04.18 [12] Palumbo B, Bianconi F, Palumbo I, et al. Value of shape and texture features from 18F-FDG PET/CT to discriminate between benign and malignant solitary pulmonary nodules: an experimental evaluation [J]. Diagnostics (Basel), 2020, 10(9): E696. doi: 10.3390/diagnostics10090696 [13] Barta JA, Henschke CI, Flores RM, et al. Lung cancer diagnosis by fine needle aspiration is associated with reduction in resection of nonmalignant lung nodules[J]. Ann Thorac Surg, 2017, 103(6): 1795-801. doi: 10.1016/j.athoracsur.2016.11.055 [14] Pelgrim GJ, van Hamersvelt RW, Willemink MJ, et al. Accuracy of iodine quantification using dual energy CT in latest generation dual source and dual layer CT[J]. Eur Radiol, 2017, 27(9): 3904-12. doi: 10.1007/s00330-017-4752-9 [15] Ko JP, Azour L. Management of incidental lung nodules[J]. Semin Ultrasound CT MR, 2018, 39(3): 249-59. doi: 10.1053/j.sult.2018.02.006 [16] 汤砺, 刘成平, 何茂, 等. 64排螺旋CT对肺内占位良恶性的鉴别诊断价值[J]. 河北医药, 2019, 41(20): 3063-8. doi: 10.3969/j.issn.1002-7386.2019.20.004 [17] Anderson IJ, Davis AM. Incidental pulmonary nodules detected on CT images[J]. JAMA, 2018, 320(21): 2260-1. doi: 10.1001/jama.2018.16336 [18] 杨超, 黄显龙, 杨华, 等. 64排螺旋CT多期增强扫描联合血管成像对肺内肿块的诊断价值[J]. 重庆医学, 2015, 44(7): 916-8. doi: 10.3969/j.issn.1671-8348.2015.07.018 [19] Lv Y, Jin YR, Xu DG, et al. Assessment of 64-slice spiral computed tomography with perfusion weighted imaging in the early diagnosis of ground-glass opacity lung cancer[J]. J BUON, 2016, 21(4): 954-7. http://europepmc.org/abstract/med/27685919 [20] 张轩斌, 金博, 彭飞. MSCT下病灶内支气管动脉形态特征对肺部良恶性疾病的诊断价值研究[J]. 癌症进展, 2017, 15(11): 1293-5. https://www.cnki.com.cn/Article/CJFDTOTAL-AZJZ201711016.htm [21] 高益萍, 黎良山, 沈志炜, 等. 肺结节CT靶扫描及重建技术对肺腺癌支气管改变的诊断价值分析[J]. 中国医学计算机成像杂志, 2019, 25 (2): 129-32. doi: 10.3969/j.issn.1006-5741.2019.02.008 [22] 李红艳, 韩伟. 64排螺旋CT低剂量扫描在肺孤立小结节良恶性鉴别诊断中应用研究[J]. 中国医疗设备, 2017, 32(S2): 140-1. https://www.cnki.com.cn/Article/CJFDTOTAL-YLSX2017S2168.htm [23] 张振显, 杨爱莲, 吴爱军, 等. 多层螺旋CT动脉扫描及三维重建在孤立性肺小结节诊断中的应用比较[J]. 中国医学装备, 2018, 15(9): 62-5. doi: 10.3969/J.ISSN.1672-8270.2018.09.017 [24] 苏保民, 谢晓霞, 陈文军, 等. 螺旋CT支气管动脉期与平衡期双期增强扫描结合靶扫描对肺结节的良、恶性诊断价值[J]. 中国防痨杂志, 2015, 37(3): 318-21. doi: 10.3969/j.issn.1000-6621.2015.03.020 [25] 胡星, 刘含秋, 张家文, 等. 孤立性肺结节与血管和支气管关系: 多层螺旋CT与病理对照初步研究[J]. 中国医学计算机成像杂志, 2015, 21(2): 105-10. https://www.cnki.com.cn/Article/CJFDTOTAL-YJTY201502005.htm [26] 吕海蓉, 苏林强, 高燕军, 等. 多层螺旋CT低剂量胸部扫描对肺结节的诊断价值[J]. 海南医学, 2020, 31(6): 751-3. doi: 10.3969/j.issn.1003-6350.2020.06.022 [27] 梁斌, 孙井松, 陈慧红, 等. 多层螺旋CT和直接数字成像系统诊断不同类型肺结核的价值[J]. 分子影像学杂志, 2020, 43(3): 428-33. doi: 10.12122/j.issn.1674-4500.2020.03.12 [28] 田素升, 张炜, 范海涛, 等. 多样化CT征象鉴别周围性肺癌与肺结核[J]. 分子影像学杂志, 2018, 41(1): 11-5. doi: 10.3969/j.issn.1674-4500.2018.01.03 [29] Lv Y, Jin Y, Yan Q, et al. The value of 64-slice spiral CT perfusion imaging in the treatment of liver cancer with argon-helium cryoablation[J]. Oncol Lett, 2016, 126(6): 4584-8. http://europepmc.org/articles/PMC5228367/ -

 点击查看大图
点击查看大图
计量
- 文章访问数: 952
- HTML全文浏览量: 279
- PDF下载量: 14
- 被引次数: 0