



Application of 64-slice spiral CT combined with multi-mode image reconstruction in preoperative resectability evaluation of hilar cholangiocarcinoma
-
摘要:
目的探究64排螺旋CT联合多模式重建图像在肝门部胆管癌(HCCA)可切除性术前评估中的应用价值。 方法回顾性分析2017年5月~2019年3月本院收治的180例HCCA患者的临床资料,所有患者术前均接受64排螺旋CT扫描检查,对患者进行鉴别诊断、TNM分期Bismuth-corlette分型和可切除性判断,并与临床病理学诊断结果进行比较,分析其在HCCA诊断、分型、分期及可切除性判断中的准确性。 结果64排螺旋CT联合多模式重建图像对HCCA的检出准确率为100%;所有患者CT检查结果显示肝内胆管扩张,大部分患者以肿瘤近侧端胆管扩张为主,14例患者伴有不同程度的肝叶萎缩,38例患者伴有肝门部淋巴结肿大,16例患者伴有肝转移,CT扫描检查结果与手术病理检查结果比较,差异无统计学意义(P>0.05);两种检查方法对HCCA临床Bismuth-Corlett分型、TNM分期及手术可切除性分析结果比较,差异无统计学意义(P>0.05)。 结论64排螺旋CT联合多模式重建图像在HCCA诊断、分型及临床分期中具有较高的准确率,可更直观、准确地评估HCCA的可切除性,在制定个性化手术方案、提高手术安全性方面,具有重要的临床价值。 Abstract:ObjectiveTo explore the application value of 64-slice spiral CT combined with multi-mode image reconstruction in preoperative resectability evaluation of hilar cholangiocarcinoma (HCCA). MethodsThe clinical data of 180 patients with HCCA who were admitted and treated in the hospital from May 2017 to March 2019 were retrospectively analyzed. All patients completed 64-slice spiral CT scanning before surgery. Differential diagnosis, TNM staging, Bismuth-corlette typing and resectability evaluation were carried out, and the results were compared with clinical pathological diagnosis results. The accuracy rates in diagnosis, classification, staging and resectability evaluation of HCCA were analyzed. ResultsThe accuracy of 64-slice spiral CT combined with multi-mode image reconstruction in detecting HCCA was 100%. CT examination results of all patients showed intrahepatic bile duct dilatation. Most patients had bile duct dilatation at the proximal end of the tumor. 14 patients had different degrees of hepatic lobe atrophy, 38 patients had hilar lymph node enlargement, and 16 patients had liver metastases. There were no significant differences between CT scanning results and surgical pathological results (P>0.05). Differences in results of clinical Bismuth-Corlett classification, TNM staging and resectability evaluation between the two methods were not statistically significant (P>0.05). Conclusion64-slice spiral CT combined with multi-mode image reconstruction has a high accuracy rate in the diagnosis, classification and clinical staging of HCCA. It can more intuitively and accurately evaluate the resectability of HCCA, which can be used in the development of personalized surgical plans and improvement of surgical safety. -
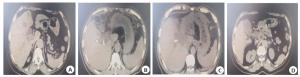
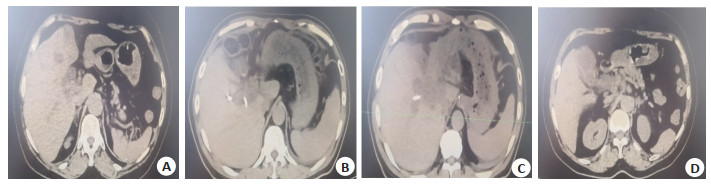
图 1 HCCA患者CT图像MPR重建
A:动脉期轻度强化; B:门静脉期; C:动脉期病灶边缘轻度强化; D:门脉期及延迟期不均匀强化, 强化范围增加.
Figure 1. MPR reconstruction of CT images of patients with HCCA.
表 1 64排螺旋CT检查与手术病理检查对HCCA诊断结果比较(n)
Table 1. Comparison of the diagnostic results of HCCA between 64- slice spiral CT and surgical pathological examination
检查方法 肝叶萎缩(n=14) 淋巴结肿大 肝转移 肝左叶 肝右叶 64排螺旋CT 11 3 38 16 手术病理检查 11 3 42 18 HCCA: Hilar cholangiocarcinoma.  下载: 导出CSV
下载: 导出CSV
表 2 64排螺旋CT检查与手术病理检查对HCCA临床Bismuth-Corlett分型结果比较(n, n= 180)
Table 2. Comparison of clinical Bismuth-Corlett classification results of HCCA between 64-slice spiral CT and surgical pathological examination
检查方法 Ⅰ型 Ⅱ型 Ⅲa型 Ⅲb型 Ⅳ型 64排螺旋CT 38 34 42 25 41 手术病理检查 38 34 39 19 50
下载: 导出CSV
表 3 64排螺旋CT检查与手术病理检查对HCCA临床TNM分期结果比较[n=180, n(%)]
Table 3. Comparison of clinical TNM staging results of HCCA between 64- slice spiral CT and surgical pathological examination
检查方法 Ⅰ期 Ⅱ期 Ⅲ期 Ⅳ期 64排螺旋CT 33(18.33) 27(15.00) 64(35.56) 56(31.11) 手术病理检查 25(13.89) 31(17.22) 68(37.78) 56(31.11)
下载: 导出CSV
表 4 64排螺旋CT检查与手术病理检查对HCCA手术可切除性分析(n=180)
Table 4. Resectability analysis of HCCA by 64-slice spiral CT and surgical pathological examination
检查方法 可切除 不可切除 64排螺旋CT 88 92 手术病理检查 79 101
下载: 导出CSV
-
[1] Schmidt A, Bloechinger M, Weber A, et al. Short- term effects and adverse events of endoscopically applied radiofrequency ablation appear to be comparable with photodynamic therapy in hilar cholangiocarcinoma[J]. United European Gastroenterol J, 2016, 4 (4): 570-9. doi: 10.1177/2050640615621235 [2] 戴海粟, 别平, 王曙光, 等.联合肝动脉切除重建在肝门部胆管癌根治术中的临床研究[J].中华外科杂志, 2018, 56(1): 41-6. [3] 晏益核, 黄玉斌.肝门部胆管癌的外科治疗现状[J].中国普通外科杂志, 2017, 26(2): 246-51. [4] 余璠, 鲁正.三维可视化技术在肝门部胆管癌术前评估中的应用[J].中国肿瘤临床, 2017, 44(8): 390-4. doi: 10.3969/j.issn.1000-8179.2017.08.249 [5] 严福华, 李卫侠, 罗先富. CT检查在肝门部胆管癌诊断与可切除性评估中的价值[J].中华消化外科杂志, 2014, 13(6): 441-6. doi: 10.3760/cma.j.issn.1673-9752.2014.06.008 [6] Sofia C, Magno C, Silipigni S, et al. Value of three-dimensional volume rendering images in the assessment of the centrality index for preoperative planning in patients with renal masses[J]. Clin Radiol, 2017, 72(1): 33-40. doi: 10.1016/j.crad.2016.09.010 [7] Bismuth H, Nakache R, Diamond T. Management strategies in resection for hilar cholangiocarcinoma[J]. Ann Surg, 1992, 215(1): 31-8. doi: 10.1097/00000658-199201000-00005 [8] Keung EZ, Gershenwald JE. The eighth edition american joint committee on cancer (AJCC) melanoma staging system: implications for melanoma treatment and care[J]. Expert Rev Anticancer Ther, 2018, 18(8): 775-84. doi: 10.1080/14737140.2018.1489246 [9] Buettner S, van Vugt JL, Gani F, et al. A comparison of prognostic schemes for perihilar cholangiocarcinoma[J]. J Gastrointest Surg, 2016, 20(10): 1716-24. doi: 10.1007/s11605-016-3203-2 [10] Fontán FJ, Reboredo ÁR, Siso AR. Accuracy of contrast-enhanced ultrasound in the diagnosis of bile duct obstruction[J]. Ultrasound Int Open, 2015, 1(1): E12-8. doi: 10.1055/s-0035-1555880 [11] 黄强, 杨骥, 林先盛, 等. CT三维重建在肝门部胆管癌的诊疗中的应用价值[J].中国普通外科杂志, 2017, 26(8): 960-7. [12] 陆谦, 王胤达, 陈佳慧, 等.三维重建技术在Bismuth Ⅲ、Ⅳ型肝门部胆管癌术前可切除性评估和手术规划中的应用[J].中华普通外科杂志, 2017, 32(3): 265-7. doi: 10.3760/cma.j.issn.1007-631X.2017.03.026 [13] 方驰华, 李乔林, 蔡伟.三维可视化技术在肝门部胆管癌诊断与治疗中的转化应用[J].中华消化外科杂志, 2018(4): 343-6. doi: 10.3760/cma.j.issn.1673-9752.2018.04.005 [14] Joo I, Lee JM, Yoon JH. Imaging diagnosis of intrahepatic and perihilar cholangiocarcinoma: recent advances and challenges[J]. Radiology, 2018, 288(1): 7-13. doi: 10.1148/radiol.2018171187 [15] 李章柱, 赵巨如, 姜相森, 等. 256层CT动态增强扫描及三维重建在肝门部胆管癌诊治中的临床应用[J].医学影像学杂志, 2018, 28(7): 1142-6. [16] 曹宪炳, 连镇炎, 杨静, 等.吲哚菁绿荧光影像技术在肝胆胰外科疾病诊治中的应用进展[J].分子影像学杂志, 2020, 43(2): 193-6. doi: 10.12122/j.issn.1674-4500.2020.02.03 [17] 倪其泓, 张赟和, 何敏, 等.多排螺旋CT三维重建技术在肝门部胆管癌术前可切除性评估与手术规划中的应用[J].中华肝胆外科杂志, 2016, 22(7): 489-90. doi: 10.3760/cma.j.issn.1007-8118.2016.07.017 [18] Zeng N, Tao H, Fang C, et al. Individualized preoperative planning using three-dimensional modeling for Bismuth and Corlette type Ⅲ hilar cholangiocarcinoma[J]. World J Surg Oncol, 2016, 14(1): 44. doi: 10.1186/s12957-016-0794-8 [19] 林科灿, 曾永毅, 黎蕴通, 等.三维重建虚拟手术规划在肝门部胆管癌手术中的应用价值[J].中华消化外科杂志, 2018, 17(4): 383-8. doi: 10.3760/cma.j.issn.1673-9752.2018.04.012 [20] 季顾惟, 朱飞鹏, 李相成.三维影像学技术在复杂肝胆外科手术中的应用进展[J].中华外科杂志, 2017, 55(4): 316-20. doi: 10.3760/cma.j.issn.0529-5815.2017.04.016 [21] Shinohara K, Ebata T, Shimoyama Y, et al. Proposal for a new classification for perihilar cholangiocarcinoma based on tumour depth[J]. Br J Surg, 2019, 106(4): 427-35. doi: 10.1002/bjs.11063 [22] Takagi K, Nanashima A, Abo T, et al. Three- dimensional printing model of liver for operative simulation in perihilar cholangiocarcinoma[J]. Hepatogastroenterology, 2014, 61(136): 2315-6. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 393
- HTML全文浏览量: 200
- PDF下载量: 6
- 被引次数: 0